
January 12, 2026 J.P. Morgan Healthcare Conference Presentation
Forward Looking Statements The forward-looking statements in this presentation
are based upon the Company’s current expectations and beliefs, and involve known and unknown risks, uncertainties and other factors, which may cause the Company’s actual results, performance and achievements and the timing of certain events to
differ materially from the results, performance, achievements or timings discussed, projected, anticipated or indicated in any forward-looking statements. Such risks, uncertainties and other factors include, among others, the following: failure
to continue to successfully commercialize ARIKAYCE in the U.S., Europe or Japan or failure to successfully commercialize BRINSUPRI in the U.S. or Europe, or to maintain U.S., European or Japanese approval for ARIKAYCE or U.S. or E.U. approval
for BRINSUPRI; our inability to obtain full approval of ARIKAYCE from the FDA, including the risk that we will not successfully or in a timely manner complete the confirmatory post-marketing clinical trial required for full approval of
ARIKAYCE, or our failure to obtain regulatory approval to expand ARIKAYCE’s indication to a broader patient population; failure to obtain, or delays in obtaining, regulatory approvals for our product candidates in the U.S., Europe or Japan, for
ARIKAYCE outside the U.S., Europe or Japan, including separate regulatory approval for Lamira® in each market and for each usage, or for brensocatib in NCFB in the U.K. or Japan; failure to successfully commercialize our product candidates, if
approved by applicable regulatory authorities, or to maintain applicable regulatory approvals for such product candidates, if approved; uncertainties or changes in the degree of market acceptance of our marketed products or, if approved, our
product candidates, by physicians, patients, third-party payors and others in the healthcare community; our inability to obtain and maintain adequate reimbursement from government or third-party payors for our marketed products or, if approved,
our product candidates, or acceptable prices for our marketed products or, if approved, our product candidates; inaccuracies in our estimates of the size of the potential markets for our marketed products and our product candidates or in data
we have used to identify physicians, expected rates of patient uptake, duration of expected treatment, or expected patient adherence or discontinuation rates; failure of third parties on which we are dependent to manufacture sufficient
quantities of our marketed products and our product candidates for commercial or clinical needs, as applicable, to conduct our clinical trials, or to comply with our agreements or laws and regulations that impact our business; the risks and
uncertainties associated with, and the perceived benefits of, our senior secured loan with certain funds managed by Pharmakon Advisors LP and our royalty financing with OrbiMed Royalty & Credit Opportunities IV, LP, including our ability to
maintain compliance with the covenants in the agreements for the senior secured loan and royalty financing and the impact of the restrictions on our operations under these agreements; our inability to create or maintain an effective direct
sales and marketing infrastructure or to partner with third parties that offer such an infrastructure for distribution of our marketed products or any of our product candidates that are approved in the future; failure to successfully conduct
future clinical trials for our marketed products or our product candidates and our potential inability to enroll or retain sufficient patients to conduct and complete the trials or generate data necessary for regulatory approval of our product
candidates or to permit the use of ARIKAYCE in the broader population of patients with MAC lung disease, among other things; development of unexpected safety or efficacy concerns related to our marketed products or our product candidates; risks
that our clinical studies will be delayed, that serious side effects will be identified during drug development, or that any protocol amendments submitted will be rejected; failure to successfully predict the time and cost of development,
regulatory approval and commercialization for novel gene therapy products; risk that interim, topline or preliminary data from our clinical trials that we announce or publish from time to time may change as more patient data become available or
may be interpreted differently if additional data are disclosed, or that blinded data will not be predictive of unblinded data; risk that our competitors may obtain orphan drug exclusivity for a product that is essentially the same as a product
we are developing for a particular indication; our inability to attract and retain key personnel or to effectively manage our growth; our inability to successfully integrate our acquisitions and appropriately manage the amount of management’s
time and attention devoted to integration activities; risks that our acquired technologies, products and product candidates will not be commercially successful; inability to adapt to our highly competitive and changing environment; inability to
access, upgrade or expand our technology systems or difficulties in updating our existing technology or developing or implementing new technology; risk that we are unable to maintain our significant customers; risk that government healthcare
legislation or other government action materially increases our costs and damages our financial condition; business or economic disruptions due to catastrophes or other events, including natural disasters or public health crises; risk that our
current and potential future use of AI and machine learning may not be successful; deterioration in general economic conditions in the U.S., Europe, Japan and globally, including the effect of prolonged periods of inflation, affecting us, our
suppliers, third-party service providers and potential partners; the risk that we could become involved in costly intellectual property disputes, be unable to adequately protect our intellectual property rights or prevent disclosure of our
trade secrets and other proprietary information, and incur costs associated with litigation or other proceedings related to such matters; restrictions or other obligations imposed on us by agreements related to our marketed products or our
product candidates, including our license agreements with PARI and AstraZeneca AB, and failure to comply with our obligations under such agreements; the cost and potential reputational damage resulting from litigation to which we are or may
become a party, including product liability claims; risk that our operations are subject to a material disruption in the event of a cybersecurity attack or issue; changes in laws and regulations applicable to our business, including any pricing
reform and laws that impact our ability to utilize certain third parties in the research, development or manufacture of our product candidates, and failure to comply with such laws and regulations; our history of operating losses, and the
possibility that we never achieve or maintain profitability; goodwill impairment charges affecting our results of operations and financial condition; inability to repay our existing indebtedness and uncertainties with respect to our ability to
access future capital; and delays in the execution of plans to build out an additional third-party manufacturing facility approved by the appropriate regulatory authorities and unexpected expenses associated with those plans. Additional
Disclaimers: Please be aware that brensocatib in HS, TPIP, INS1201, INS1202, INS1148, and INS1033 are investigational products that have not been approved for sale or found safe or effective by the FDA or any regulatory authority. In addition,
ARIKAYCE has not been approved for the treatment of all patients with MAC lung disease and brensocatib has not been approved for the treatment of patients with non-cystic fibrosis bronchiectasis outside the U.S. and the E.U. This presentation
is not promotion or advertisement of ARIKAYCE, BRINSUPRI, brensocatib in HS, TPIP, INS1201, INS1202, INS1148, or INS1033. Insmed, ARIKAYCE and BRINSUPRI are registered trademarks of Insmed Incorporated. All other trademarks are property of
their respective owner(s). HS: Hidradenitis Suppurativa | TPIP: Treprostinil Palmitil Inhalation Powder | MAC / MAC LD: Mycobacterium avium complex lung disease | FDA: Food & Drug Administration

Patient Minute
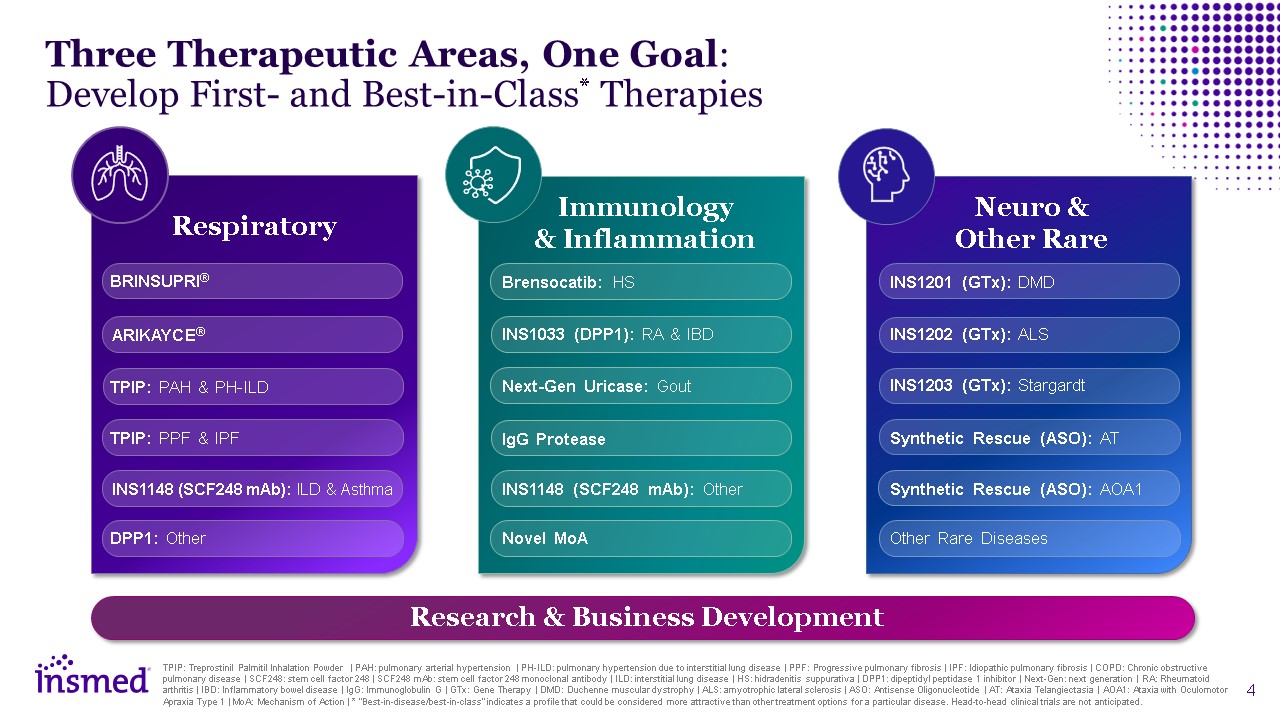
Three Therapeutic Areas, One Goal: Develop First- and Best-in-Class*
Therapies TPIP: Treprostinil Palmitil Inhalation Powder | PAH: pulmonary arterial hypertension | PH-ILD: pulmonary hypertension due to interstitial lung disease | PPF: Progressive pulmonary fibrosis | IPF: Idiopathic pulmonary fibrosis | COPD:
Chronic obstructive pulmonary disease | SCF248: stem cell factor 248 | SCF248 mAb: stem cell factor 248 monoclonal antibody | ILD: interstitial lung disease | HS: hidradenitis suppurativa | DPP1: dipeptidyl peptidase 1 inhibitor | Next-Gen:
next generation | RA: Rheumatoid arthritis | IBD: Inflammatory bowel disease | IgG: Immunoglobulin G | GTx: Gene Therapy | DMD: Duchenne muscular dystrophy | ALS: amyotrophic lateral sclerosis | ASO: Antisense Oligonucleotide | AT: Ataxia
Telangiectasia | AOA1: Ataxia with Oculomotor Apraxia Type 1 | MoA: Mechanism of Action | * “Best-in-disease/best-in-class" indicates a profile that could be considered more attractive than other treatment options for a particular disease.
Head-to-head clinical trials are not anticipated. Respiratory Immunology & Inflammation Neuro & Other Rare Research & Business Development BRINSUPRI® ARIKAYCE® TPIP: PAH & PH-ILD TPIP: PPF & IPF DPP1:
Other INS1148 (SCF248 mAb): ILD & Asthma INS1202 (GTx): ALS INS1203 (GTx): Stargardt Synthetic Rescue (ASO): AT Other Rare Diseases INS1201 (GTx): DMD Synthetic Rescue (ASO): AOA1 Brensocatib: HS INS1033 (DPP1): RA & IBD Novel
MoA Next-Gen Uricase: Gout IgG Protease INS1148 (SCF248 mAb): Other
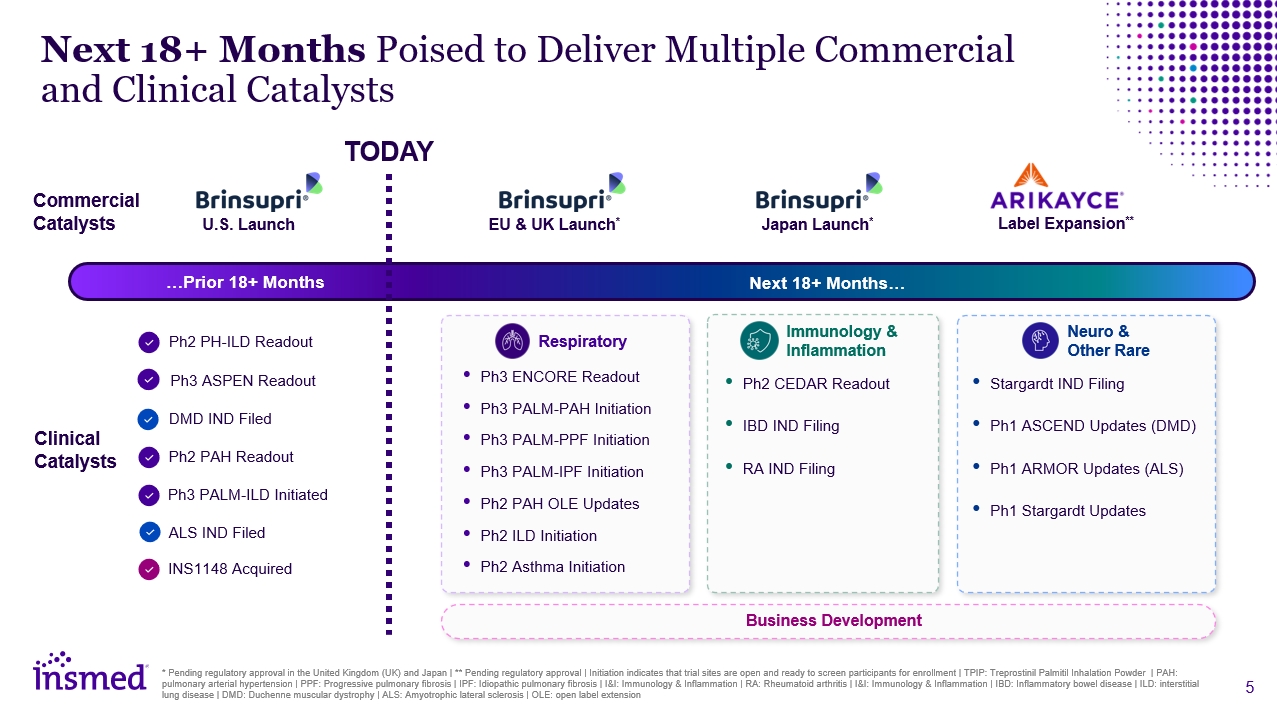
Next 18+ Months Poised to Deliver Multiple Commercial and Clinical Catalysts *
Pending regulatory approval in the United Kingdom (UK) and Japan | ** Pending regulatory approval | Initiation indicates that trial sites are open and ready to screen participants for enrollment | TPIP: Treprostinil Palmitil Inhalation Powder |
PAH: pulmonary arterial hypertension | PPF: Progressive pulmonary fibrosis | IPF: Idiopathic pulmonary fibrosis | I&I: Immunology & Inflammation | RA: Rheumatoid arthritis | I&I: Immunology & Inflammation | IBD: Inflammatory
bowel disease | ILD: interstitial lung disease | DMD: Duchenne muscular dystrophy | ALS: Amyotrophic lateral sclerosis | OLE: open label extension …Prior 18+ Months Next 18+ Months… TODAY Commercial Catalysts Clinical Catalysts U.S.
Launch EU & UK Launch* Label Expansion** Ph3 ENCORE Readout Ph3 PALM-ILD Initiation Ph3 PALM-PPF Initiation Ph3 PALM-IPF Initiation Ph2 PAH OLE Updates Ph2 ILD Initiation Ph2 Asthma Initiation Respiratory Japan Launch* Ph2
PH-ILD Readout Ph3 ASPEN Readout Ph2 PAH Readout Ph3 PALM-ILD Initiated DMD IND Filed ALS IND Filed INS1148 Acquired Immunology & Inflammation Ph2 CEDAR Readout IBD IND Filing RA IND Filing Neuro & Other Rare Stargardt
IND Filing Ph1 ASCEND Updates (DMD) Ph1 ARMOR Updates (ALS) Ph1 Stargardt Updates Business Development
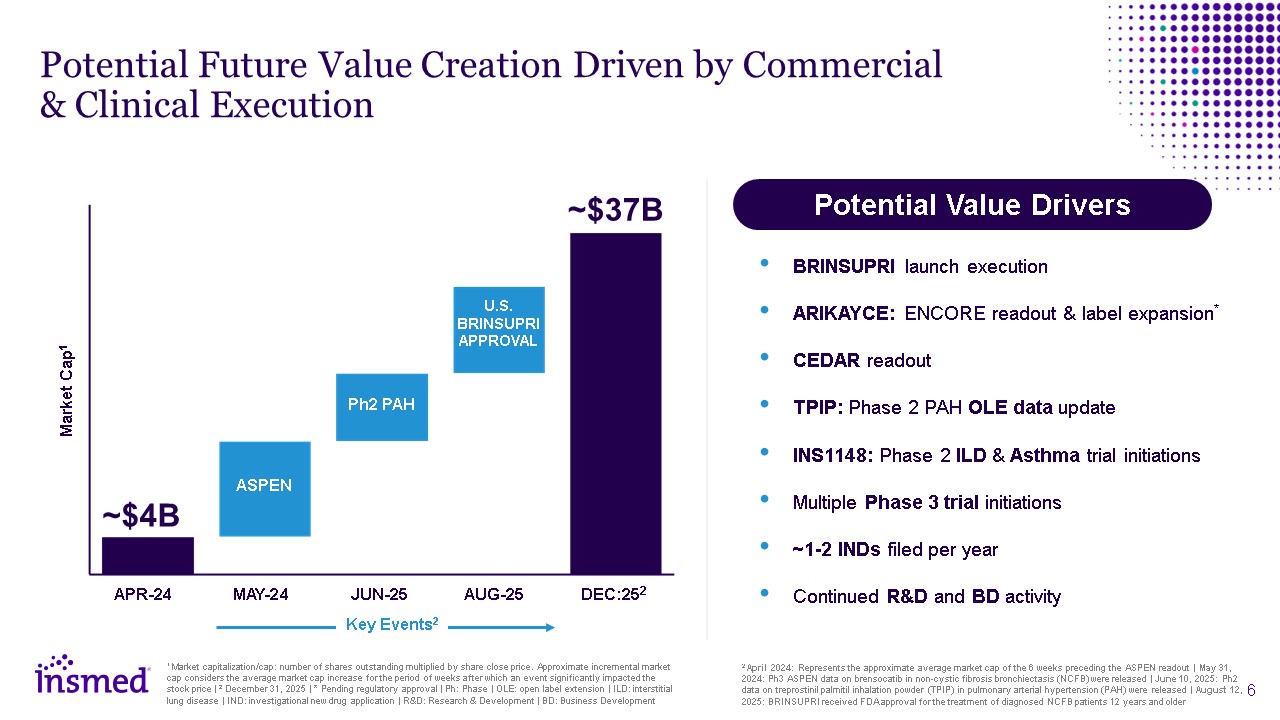
Potential Value Drivers BRINSUPRI launch execution ARIKAYCE: ENCORE readout
& label expansion* CEDAR readout TPIP: Phase 2 PAH OLE data update INS1148: Phase 2 ILD & Asthma trial initiations Multiple Phase 3 trial initiations ~1-2 INDs filed per year Continued R&D and BD activity Potential Future
Value Creation Driven by Commercial & Clinical Execution 2 April 2024: Represents the approximate average market cap of the 6 weeks preceding the ASPEN readout | May 31, 2024: Ph3 ASPEN data on brensocatib in non-cystic fibrosis
bronchiectasis (NCFB) were released | June 10, 2025: Ph2 data on treprostinil palmitil inhalation powder (TPIP) in pulmonary arterial hypertension (PAH) were released | August 12, 2025: BRINSUPRI received FDA approval for the treatment of
diagnosed NCFB patients 12 years and older 1 Market capitalization/cap: number of shares outstanding multiplied by share close price. Approximate incremental market cap considers the average market cap increase for the period of weeks after
which an event significantly impacted the stock price | 2 December 31, 2025 | * Pending regulatory approval | Ph: Phase | OLE: open label extension | ILD: interstitial lung disease | IND: investigational new drug application | R&D: Research
& Development | BD: Business Development Market Cap1 APR-24 MAY-24 JUN-25 AUG-25 DEC:252 ASPEN Ph2 PAH ~$37B ~$4B U.S. BRINSUPRI APPROVAL Key Events2

Respiratory T H E R A P E U T I C A R E A
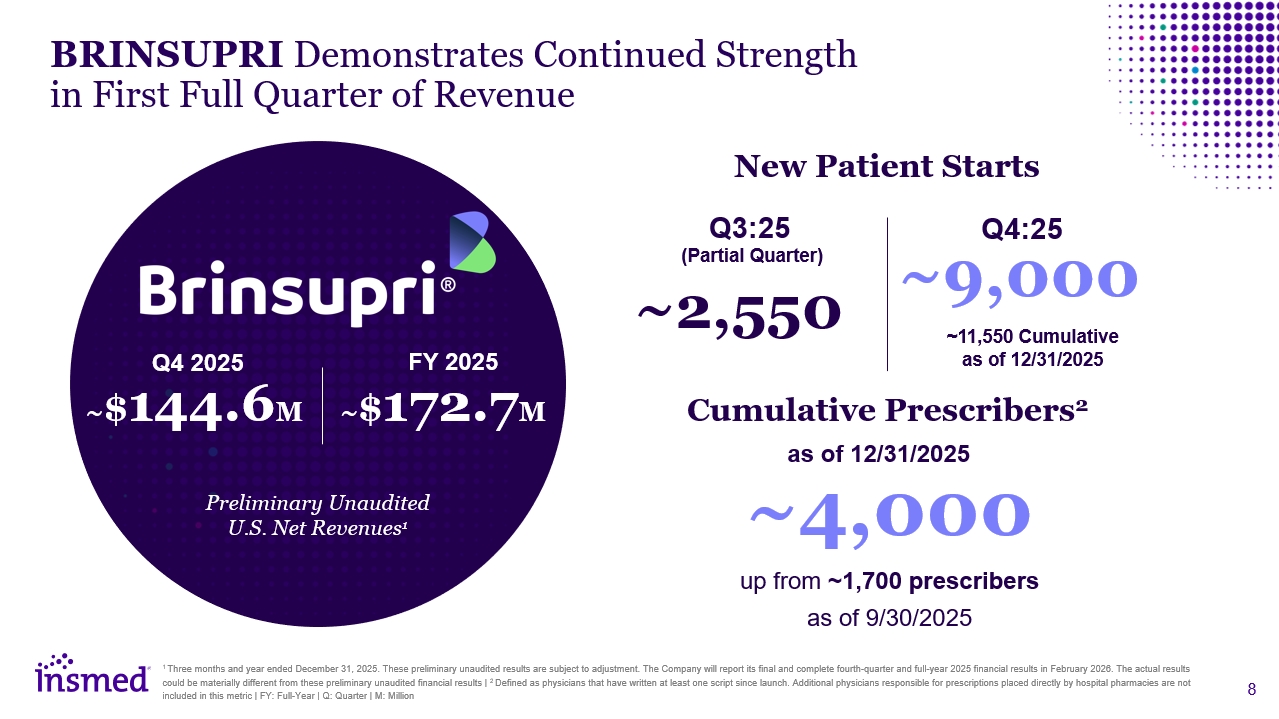
BRINSUPRI Demonstrates Continued Strength in First Full-Quarter of
Revenue Preliminary Unaudited U.S. Net Revenues1 ~$144.6M Q4 2025 FY 2025 ~$172.7M New Patient Starts Cumulative Prescribers2 ~4,000 up from ~1,700 prescribers as of 9/30/2025 as of 12/31/2025 Q3:25 ~2,550 (Partial
Quarter) ~9,000 Q4:25 (Full Quarter) 1 Three months and year ended December 31, 2025. These preliminary unaudited results are subject to adjustment. The Company will report its final and complete fourth-quarter and full-year 2025 financial
results in February 2026. The actual results could be materially different from these preliminary unaudited financial results | 2 Defined as physicians that have written at least one script since launch. Additional physicians responsible for
prescriptions placed directly by hospital pharmacies are not included in this metric | FY: Full-Year | Q: Quarter | M: Million
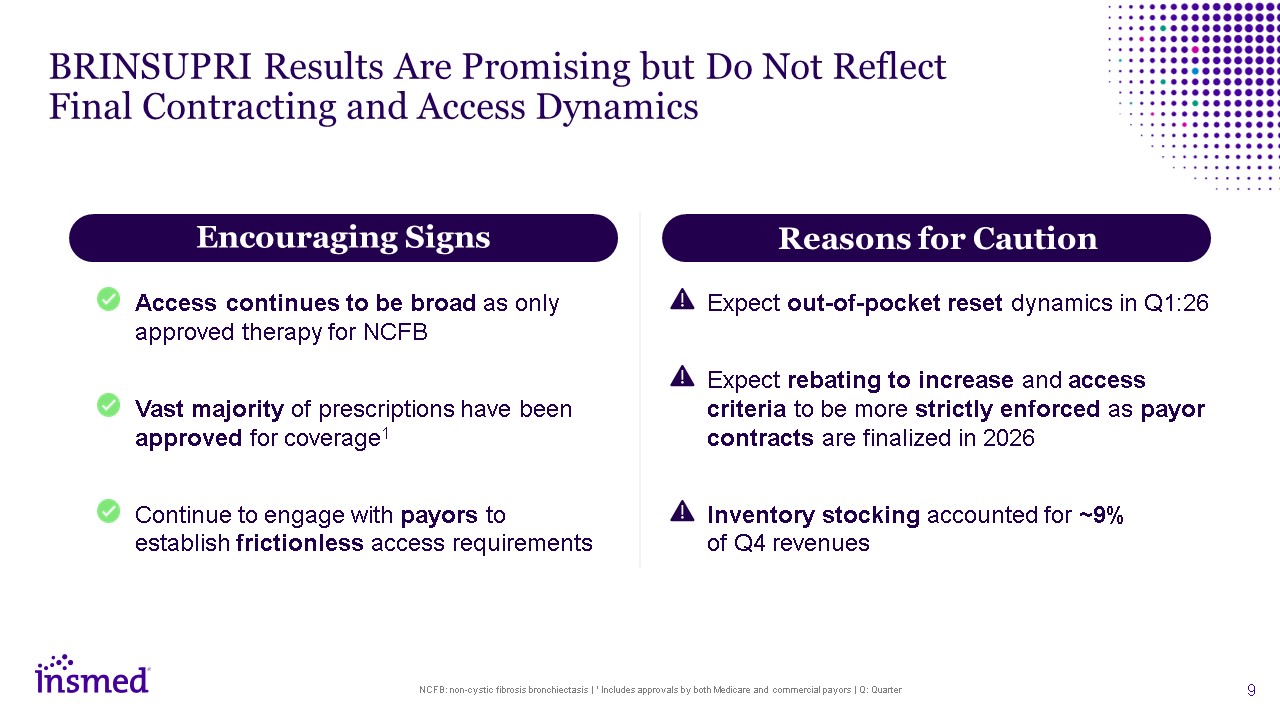
BRINSUPRI Results Are Promising but Do Not Reflect Final Contracting and Access
Dynamics NCFB: non-cystic fibrosis bronchiectasis | 1 Includes approvals by both Medicare and commercial payors | Q: Quarter Access continues to be broad as only approved therapy for NCFB Vast majority of prescriptions have been approved for
coverage1 Continue to engage with payors to establish frictionless access requirements Expect out-of-pocket reset dynamics in Q1:26 Expect rebating to increase and access criteria to be more strictly enforced as payor contracts are finalized
in 2026 Inventory stocking accounted for ~9% of Q4 revenues Encouraging Signs Reasons for Caution
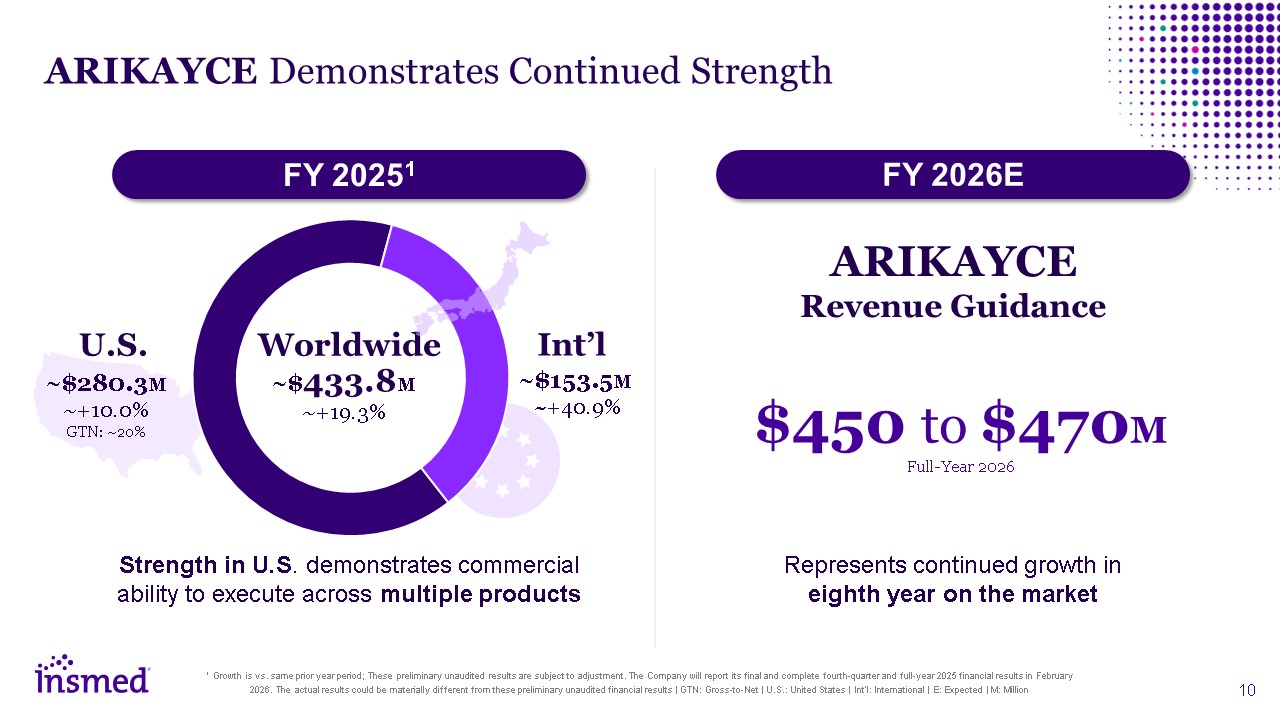
ARIKAYCE Demonstrates Continued Strength 1 Growth is vs. same prior year period;
These preliminary unaudited results are subject to adjustment. The Company will report its final and complete fourth-quarter and full-year 2025 financial results in February 2026. The actual results could be materially different from these
preliminary unaudited financial results | GTN: Gross-to-Net | U.S.: United States | Int’l: International | E: Expected | M: Million Strength in U.S. demonstrates commercial ability to execute across multiple
products U.S. ~$280.3M ~+10.0% GTN: ~20% Int’l ~$153.5M ~+40.9% Worldwide ~$433.8M ~+19.3% FY 20251 $450 to $470M Full-Year 2026 ARIKAYCE Revenue Guidance FY 2026E Represents continued growth in eighth year on the market
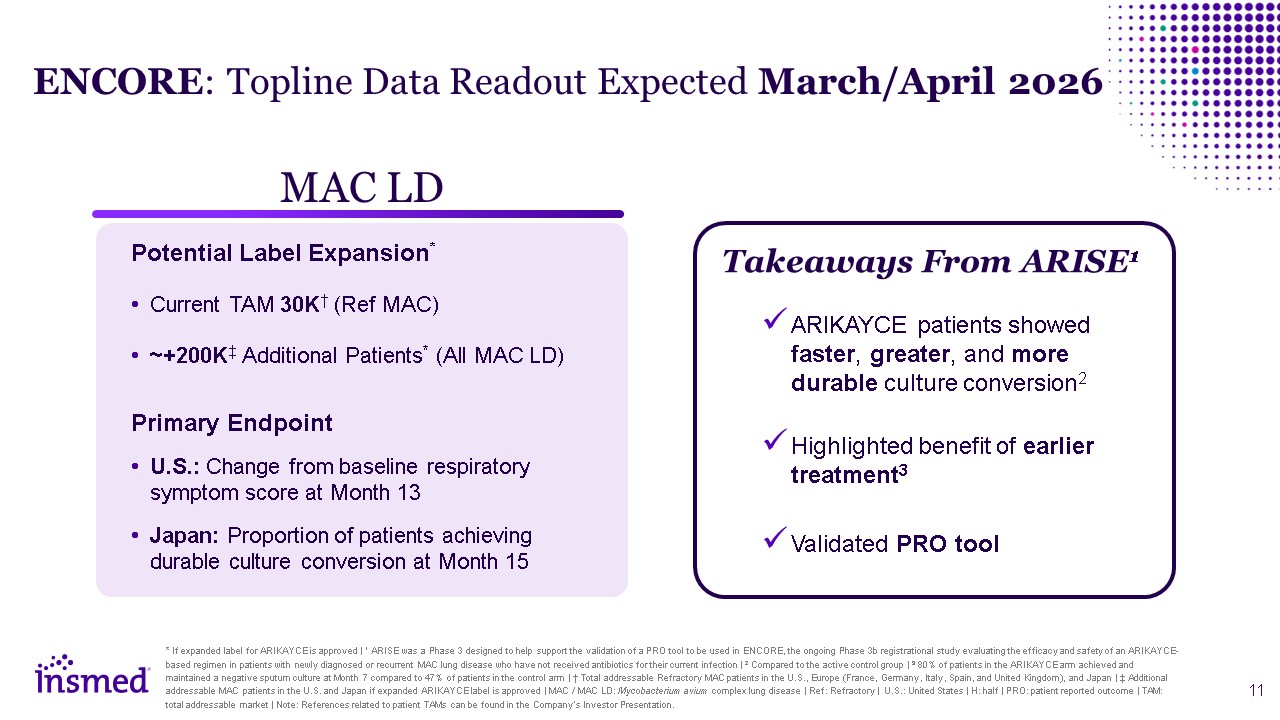
* If expanded label for ARIKAYCE is approved | 1 ARISE was a Phase 3 designed to
help support the validation of a PRO tool to be used in ENCORE, the ongoing Phase 3b registrational study evaluating the efficacy and safety of an ARIKAYCE-based regimen in patients with newly diagnosed or recurrent MAC lung disease who have
not received antibiotics for their current infection | 2 Compared to the active control group | 3 80% of patients in the ARIKAYCE arm achieved and maintained a negative sputum culture at Month 7 compared to 47% of patients in the control arm |
† Total addressable Refractory MAC patients in the U.S., Europe (France, Germany, Italy, Spain, and United Kingdom), and Japan | ‡ Additional addressable MAC patients in the U.S. and Japan if expanded ARIKAYCE label is approved | MAC / MAC LD:
Mycobacterium avium complex lung disease | Ref: Refractory | U.S.: United States | H: half | PRO: patient reported outcome | TAM: total addressable market | Note: References related to patient TAMs can be found in the Company's Investor
Presentation. ENCORE: Topline Data Readout Expected March/April 2026 MAC LD Potential Label Expansion* Current TAM 30K† (Ref MAC) ~+200K‡ Additional Patients* (All MAC LD) Primary Endpoint U.S.: Change from baseline respiratory symptom
score at Month 13 Japan: Proportion of patients achieving durable culture conversion at Month 15 ARIKAYCE patients showed faster, greater, and more durable culture conversion2 Highlighted benefit of earlier treatment3 Validated PRO
tool Takeaways From ARISE1 11
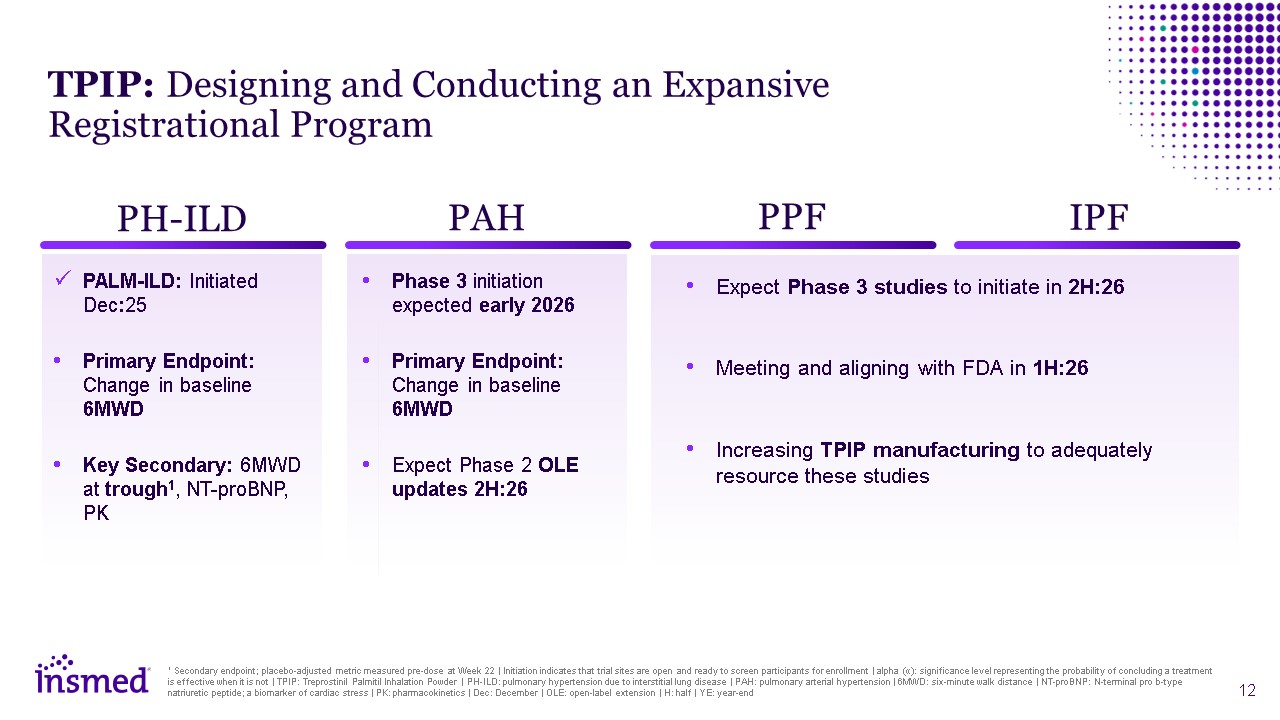
PALM-ILD: Initiated Dec:25 Primary Endpoint: Change in baseline 6MWD Key
Secondary: 6MWD at trough1, NT-proBNP, PK Phase 3 initiation expected early 2026 Primary Endpoint: Change in baseline 6MWD Expect Phase 2 OLE updates 2H:26 Expect Phase 3 studies to initiate in 2H:26 Meeting and aligning with FDA in
1H:26 Increasing TPIP manufacturing to adequately resource these studies PH-ILD PAH PPF IPF TPIP: Designing and Conducting an Expansive Registrational Program 1 Secondary endpoint; placebo-adjusted metric measured pre-dose at Week 22 |
Initiation indicates that trial sites are open and ready to screen participants for enrollment | alpha (α): significance level representing the probability of concluding a treatment is effective when it is not | TPIP: Treprostinil Palmitil
Inhalation Powder | PH-ILD: pulmonary hypertension due to interstitial lung disease | PAH: pulmonary arterial hypertension | 6MWD: six-minute walk distance | NT-proBNP: N-terminal pro b-type natriuretic peptide; a biomarker of cardiac stress |
PK: pharmacokinetics | Dec: December | OLE: open-label extension | H: half | YE: year-end
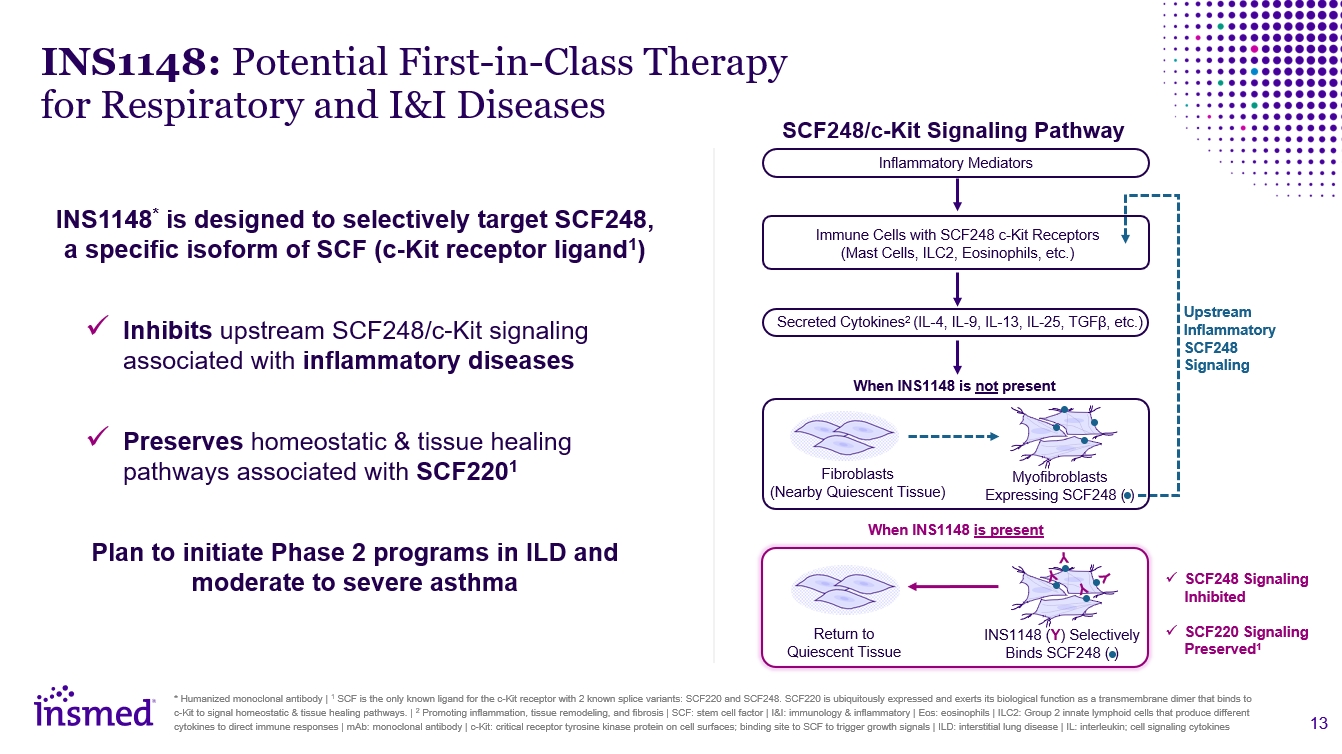
INS1148: Potential First-in-Class Therapy for Respiratory and I&I Diseases *
Humanized monoclonal antibody | 1 SCF is the only known ligand for the c-Kit receptor with 2 known splice variants: SCF220 and SCF248. SCF220 is ubiquitously expressed and exerts its biological function as a transmembrane dimer that binds to
c-Kit to signal homeostatic & tissue healing pathways. | 2 Promoting inflammation, tissue remodeling, and fibrosis | SCF: stem cell factor | I&I: immunology & inflammatory | Eos: eosinophils | ILC2: Group 2 innate lymphoid cells
that produce different cytokines to direct immune responses | mAb: monoclonal antibody | c-Kit: critical receptor tyrosine kinase protein on cell surfaces; binding site to SCF to trigger growth signals | ILD: interstitial lung disease | IL:
interleukin; cell signaling cytokines INS1148* is designed to selectively target SCF248, a specific isoform of SCF and a c-Kit receptor ligand1 INS1148 has the potential to… Inhibit upstream SCF248/c-Kit signaling associated with
inflammatory diseases Preserve homeostatic & tissue healing pathways associated with SCF2201 Plan to initiate Phase 2 programs in ILD and moderate-to-severe asthma Inflammatory Mediators SCF248/c-Kit Signaling Pathway Upstream
Inflammatory SCF248 Signaling Secreted Cytokines2 (IL-4, IL-9, IL-13, IL-25, TGFβ, etc.) Immune Cells with SCF248 c-Kit Receptors (Mast Cells, ILC2, Eosinophils, etc.) When INS1148 is not present When INS1148 is present SCF248 Signaling
Inhibited SCF220 Signaling Preserved1 Return to Quiescent Tissue INS1148 (Y) Selectively Binds SCF248 ( ) Y Y Y Y Fibroblasts (Nearby Quiescent Tissue) Myofibroblasts Expressing SCF248 ( )
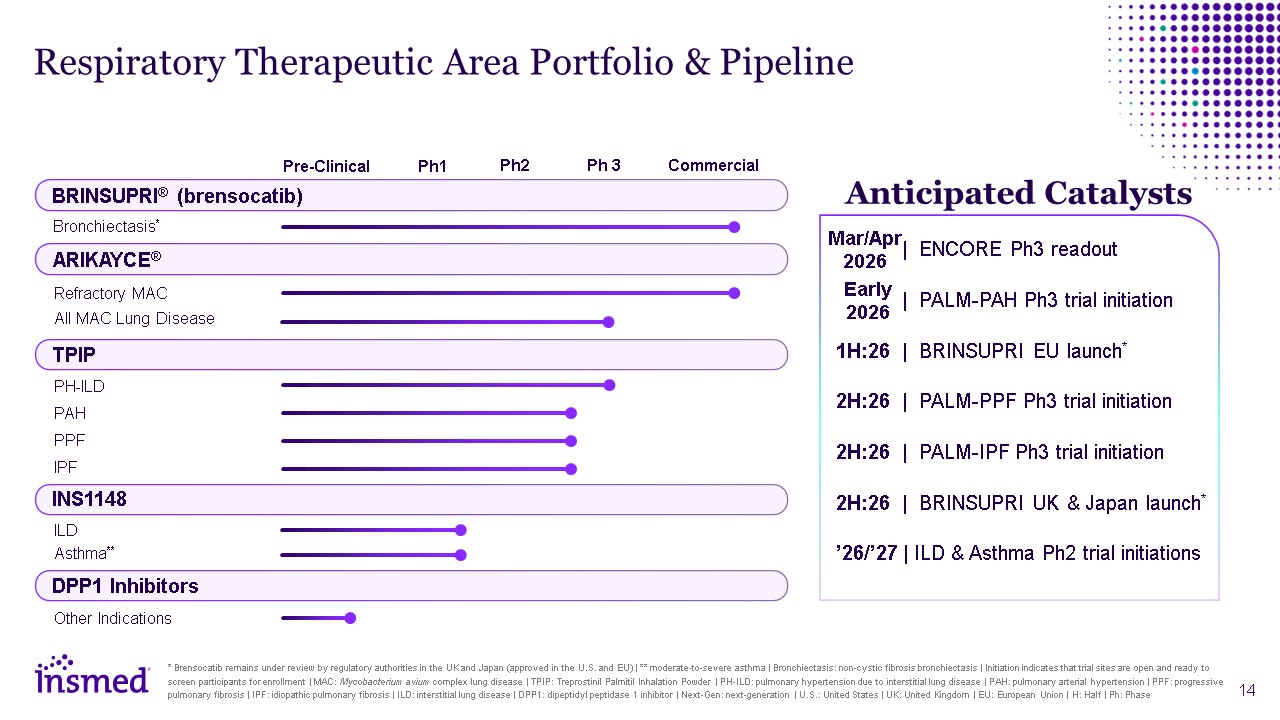
Respiratory Therapeutic Area Portfolio & Pipeline * Brensocatib remains under
review by regulatory authorities in the UK and Japan (approved in the U.S. and EU) | ** moderate-to-severe asthma | Bronchiectasis: non-cystic fibrosis bronchiectasis | Initiation indicates that trial sites are open and ready to screen
participants for enrollment | MAC: Mycobacterium avium complex lung disease | TPIP: Treprostinil Palmitil Inhalation Powder | PH-ILD: pulmonary hypertension due to interstitial lung disease | PAH: pulmonary arterial hypertension | PPF:
progressive pulmonary fibrosis | IPF: idiopathic pulmonary fibrosis | ILD: interstitial lung disease | DPP1: dipeptidyl peptidase 1 inhibitor | Next-Gen: next-generation | U.S.: United States | UK: United Kingdom | EU: European Union | H: Half
| Ph: Phase Anticipated Catalysts | ENCORE Ph3 readout | PALM-PAH Ph3 trial initiation 1H:26 | BRINSUPRI EU launch* 2H:26 | PALM-PPF Ph3 trial initiation 2H:26 | PALM-IPF Ph3 trial initiation 2H:26 | BRINSUPRI UK & Japan
launch* ’26/’27 | ILD & Asthma Ph2 trial initiations Mar/Apr 2026 BRINSUPRI® (brensocatib) Bronchiectasis* Pre-Clinical Ph1 Ph2 Ph 3 Commercial DPP1 Inhibitors Other Indications TPIP
PH-ILD PAH PPF IPF INS1148 ILD Asthma** ARIKAYCE® Refractory MAC All MAC Lung Disease Early 2026

Immunology & Inflammation T H E R A P E U T I C A R E A
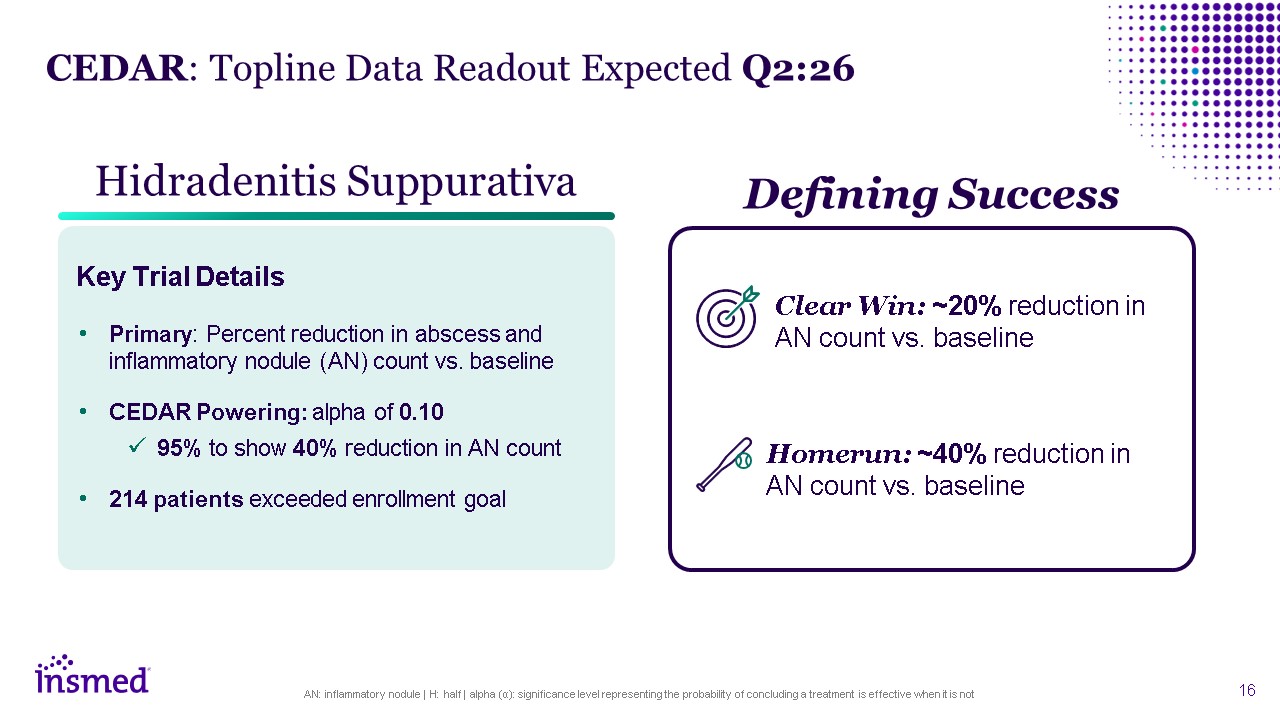
AN: inflammatory nodule | H: half | alpha (α): significance level representing the
probability of concluding a treatment is effective when it is not Hidradenitis Suppurativa Primary: Percent reduction in abscess and inflammatory nodule (AN) count vs. baseline CEDAR Powering: alpha of 0.10 95% to show 40% reduction in AN
count 214 patients exceeded enrollment goal CEDAR: Topline Data Readout Expected Q2:26 Defining Success Clear Win: ~20% reduction in AN count vs. baseline Key Trial Details Homerun: ~40% reduction in AN count vs. baseline
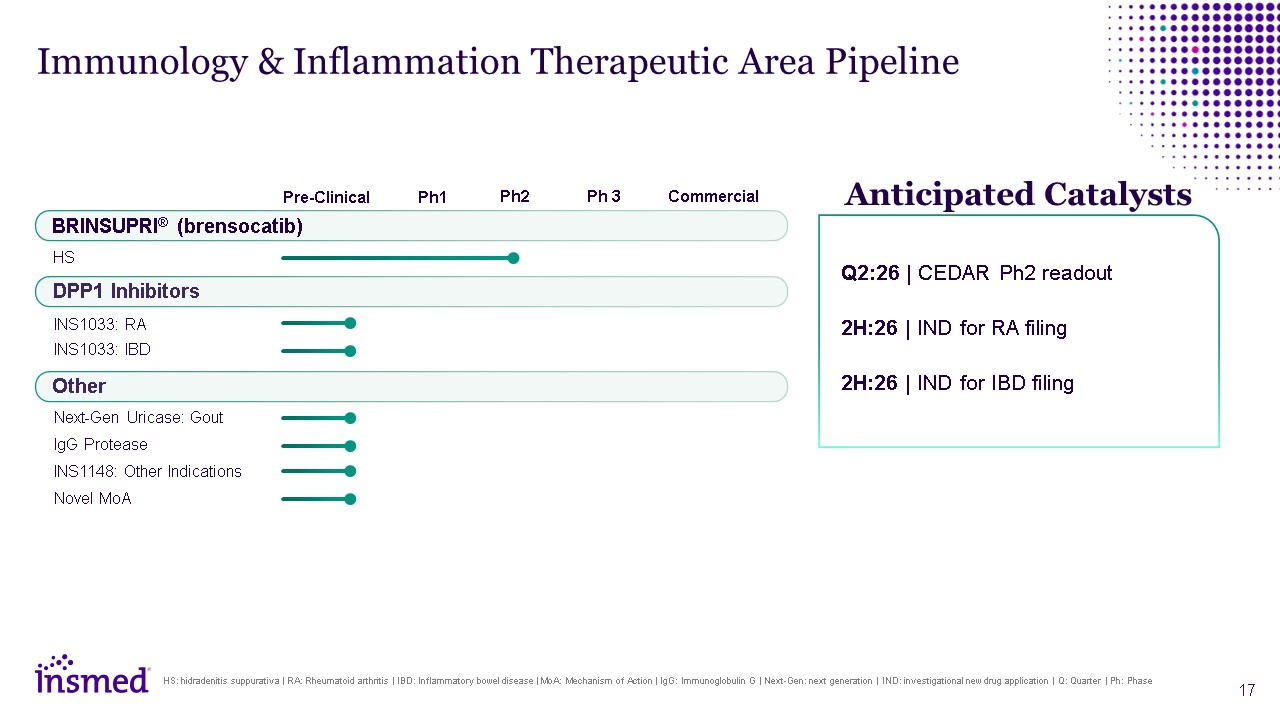
Immunology & Inflammation Therapeutic Area Pipeline BRINSUPRI®
(brensocatib) HS Pre-Clinical Ph1 Ph2 Ph 3 Commercial Other Next-Gen Uricase: Gout IgG Protease INS1148: Other Indications Novel MoA DPP1 Inhibitors INS1033: RA INS1033: IBD Anticipated Catalysts Q2:26 | CEDAR Ph2 readout
2H:26 | IND for RA filing 2H:26 | IND for IBD filing HS: hidradenitis suppurativa | RA: Rheumatoid arthritis | IBD: Inflammatory bowel disease | MoA: Mechanism of Action | IgG: Immunoglobulin G | Next-Gen: next generation | IND:
investigational new drug application | Q: Quarter | Ph: Phase

Neuro & Other Rare T H E R A P E U T I C A R E A
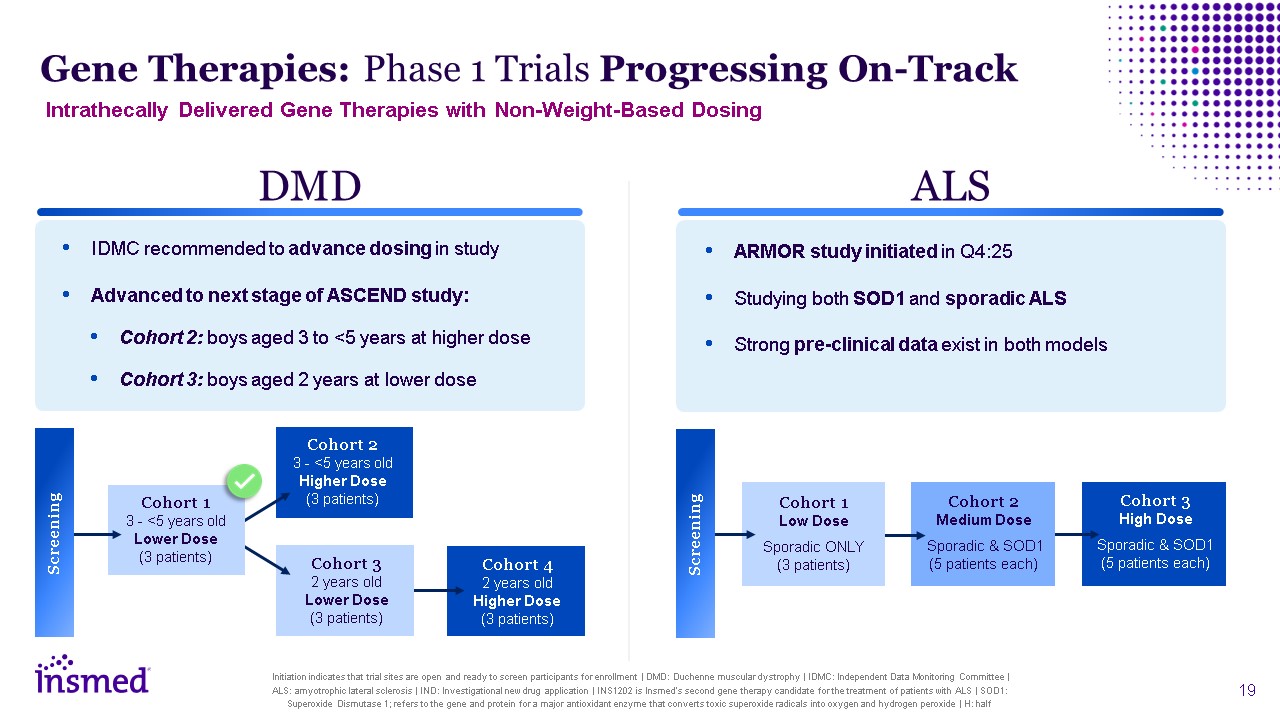
Gene Therapies: Phase 1 Trials Progressing On-Track Initiation indicates that
trial sites are open and ready to screen participants for enrollment | DMD: Duchenne muscular dystrophy | IDMC: Independent Data Monitoring Committee | ALS: amyotrophic lateral sclerosis | IND: Investigational new drug application | INS1202 is
Insmed’s second gene therapy candidate for the treatment of patients with ALS | SOD1: Superoxide Dismutase 1; refers to the gene and protein for a major antioxidant enzyme that converts toxic superoxide radicals into oxygen and hydrogen
peroxide | H: half DMD IDMC recommended to advance dosing in study Advanced to next stage of ASCEND study: Cohort 2: boys aged 3 to <5 years at higher dose Cohort 3: boys aged 2 years at lower dose ALS ARMOR study initiated in
Q4:25 Studying both SOD1 and sporadic ALS Strong pre-clinical data exist in both models Cohort 4 2 years old Higher Dose (3 patients) Cohort 2 3 - <5 years old Higher Dose (3 patients) Cohort 3 2 years old Lower Dose (3
patients) Cohort 1 3 - <5 years old Lower Dose (3 patients) Screening Cohort 3 High Dose Sporadic & SOD1 (5 patients each) Cohort 2 Medium Dose Sporadic & SOD1 (5 patients each) Cohort 1 Low Dose Sporadic ONLY (3
patients) Screening Intrathecally Delivered Gene Therapies with Non-Weight-Based Dosing
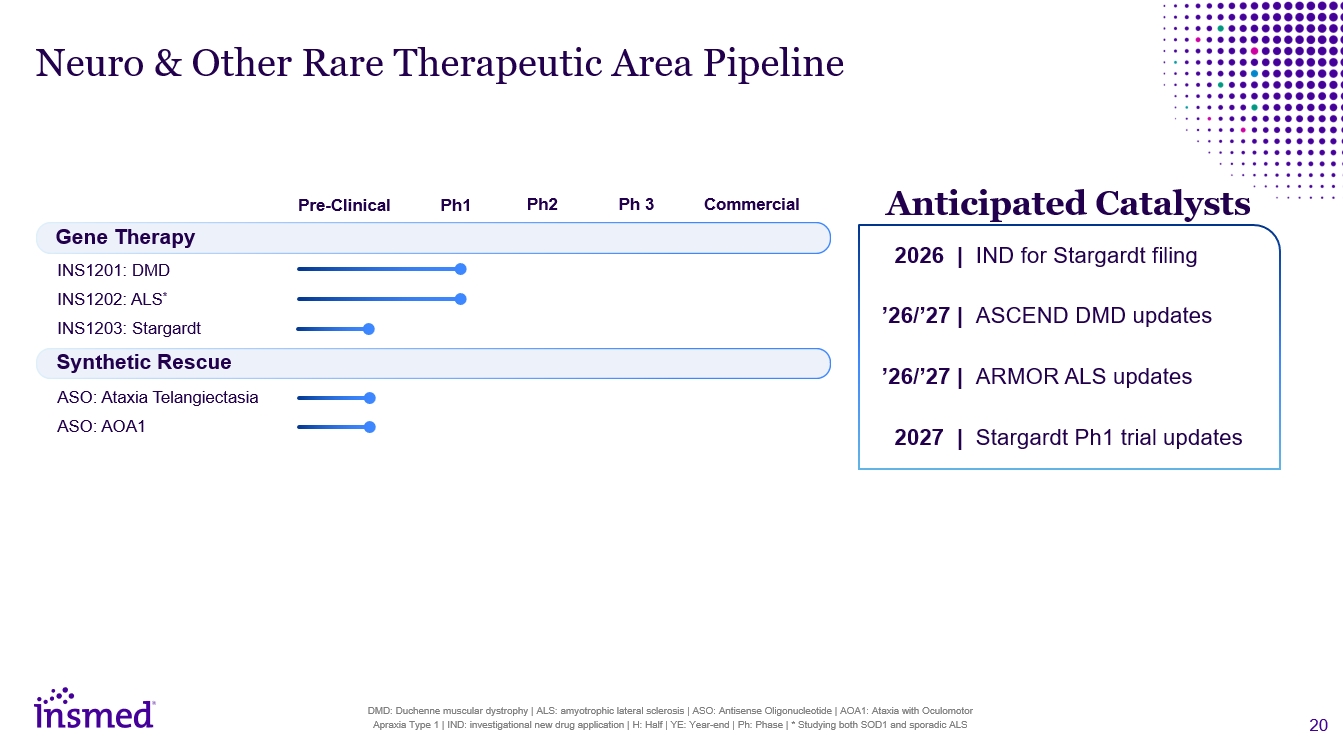
Anticipated Catalysts 2026 | IND for Stargardt filing ’26/’27 | ASCEND DMD
updates ’26/’27 | ARMOR ALS updates 2027 | Stargardt Ph1 trial updates Neuro & Other Rare Therapeutic Area Pipeline Gene Therapy INS1201: DMD INS1202: ALS* INS1203: Stargardt Pre-Clinical Ph1 Ph2 Ph 3 Commercial Synthetic
Rescue DMD: Duchenne muscular dystrophy | ALS: amyotrophic lateral sclerosis | ASO: Antisense Oligonucleotide | AOA1: Ataxia with Oculomotor Apraxia Type 1 | IND: investigational new drug application | H: Half | YE: Year-end | Ph: Phase | *
Studying both SOD1 and sporadic ALS ASO: Ataxia Telangiectasia ASO: AoA1

Financial Strength Allows Us to Pursue Our Ambitious Goals 1 Unaudited revenue
results and/or cash, cash equivalents, and marketable securities | 2 year-over-year growth vs. unaudited 2025 revenue results | 3 Revenue guidance for current label; does not include revenues from potential label expansion | BD: business
development | U.S.: United States Capital Allocation Deploy capital to maximize opportunities for patients Prioritize BD opportunities with promising science $1.7B as of 9/30/20251 Cash Position 2025 $433.8M 2026 Guidance $450M to
$470M $28.1M U.S. Only1 Q3:25 (Partial) $144.6M U.S. Only1 Q4:25 (Full) 1 Preliminary unaudited revenue results are subject to adjustment. The Company will report its final and complete fourth-quarter and full-year 2025 financial
results in February 2026. The actual results could be materially different from these preliminary unaudited financial results | U.S.: United States | M: Million | BD: Business development Worldwide1 Worldwide
Our Culture is Our Greatest Strength In a recent survey* >90% of
employees who responded said they felt: Proud to work at Insmed Inspired by what we do Confident in Insmed’s future Driven to do their best work * The 2025 annual Insmed Pulse Survey included 92% participation across the
organization Certified as a U.S. Great Place to Work No. 1 on Science’s Top BioPharma Employers List Five Years in a Row

2026: Building On Our Momentum Next 18+ Months: Potential future value creation
driven by commercial execution and clinical progress Three Therapeutic Areas: New structure supports the evolution of our commercial portfolio & clinical pipeline BRINSUPRI: Strong start to U.S. launch; multiple international launches
expected in 2026* U.S.: United States | * Pending regulatory approval in the United Kingdom (UK) and Japan
Thank You