July 16, 2026 12-Month Results from Ongoing Open-Label Extension Study of TPIP in
PAH Patients TPIP: treprostinil palmitil inhalation powder | PAH: pulmonary arterial hypertension
Forward Looking Statements The forward-looking statements in this presentation
are based upon the Company's current expectations and beliefs, and involve known and unknown risks, uncertainties and other factors, which may cause the Company's actual results, performance and achievements and the timing of certain events to
differ materially from the results, performance, achievements or timings discussed, projected, anticipated or indicated in any forward-looking statements. Such risks, uncertainties and other factors include, among others, the following: the
risk that the full data set from the OLE study of TPIP in PAH (the “Study”) or data generated in further clinical trials of TPIP will not be consistent with the interim results of the Study; the risk that data from the Study, which is conducted
in a single-arm, open-label design without a concurrent placebo control group, may not be predictive of, or may differ materially from, results obtained in the Phase 3 PALM-PAH randomized, double-blind, placebo-controlled trial; the risk that
the Study’s efficacy endpoints, which are secondary and exploratory in nature, may overestimate or otherwise not accurately reflect the true treatment effect of TPIP; failure to successfully conduct future clinical trials for TPIP, such as the
Company’s planned Phase 3 program for TPIP, including due to the Company's potential inability to enroll or retain sufficient patients to conduct and complete the trials or generate data necessary for regulatory approval, among other things;
development of unexpected safety or efficacy concerns related to TPIP; failure of third parties on which the Company is dependent to manufacture sufficient quantities of TPIP for clinical needs, to conduct the Company's clinical trials, or to
comply with the Company's agreements or laws and regulations that impact the Company's business or agreements with the Company; failure to obtain regulatory approval for TPIP; inaccuracies in the Company's estimates of the size of the potential
markets for TPIP or in data the Company has used to identify physicians; expected rates of patient uptake, duration of expected treatment, or expected patient adherence or discontinuation rates, if TPIP is approved; inability of the Company or
the Company's third-party manufacturers to comply with regulatory requirements related to TPIP; the Company's inability to obtain adequate reimbursement from government or third-party payors for TPIP or acceptable prices for TPIP, if approved;
restrictions or other obligations imposed on the Company by agreements related to TPIP and failure to comply with the Company’s obligations under such agreements; risks that the Company's clinical studies will be delayed or that serious side
effects will be identified during drug development; the strength and enforceability of the Company’s intellectual property rights or the rights of third parties; and the cost and potential reputational damage resulting from litigation to which
the Company may become a party, including product liability claims. Additional Disclaimers: Please be aware that TPIP is an investigational product that has not been approved for sale or found safe or effective by the FDA or any regulatory
authority. This presentation is not promotion or advertisement of TPIP. TPIP: treprostinil palmitil inhalation powder | FDA: Food & Drug Administration
Opening Remarks Study Results KOL Reflection Closing
Remarks 5-7 9-18 19 20-21 Will Lewis Chair & CEO Gene Sullivan Chief Product Strategy Officer KOL: key opinion leader Dr. Raymond Benza George M. and Linda H. Kaufman Academic Chair of Cardiology, Sentara Health

Opening Remarks Will Lewis | Chair & CEO
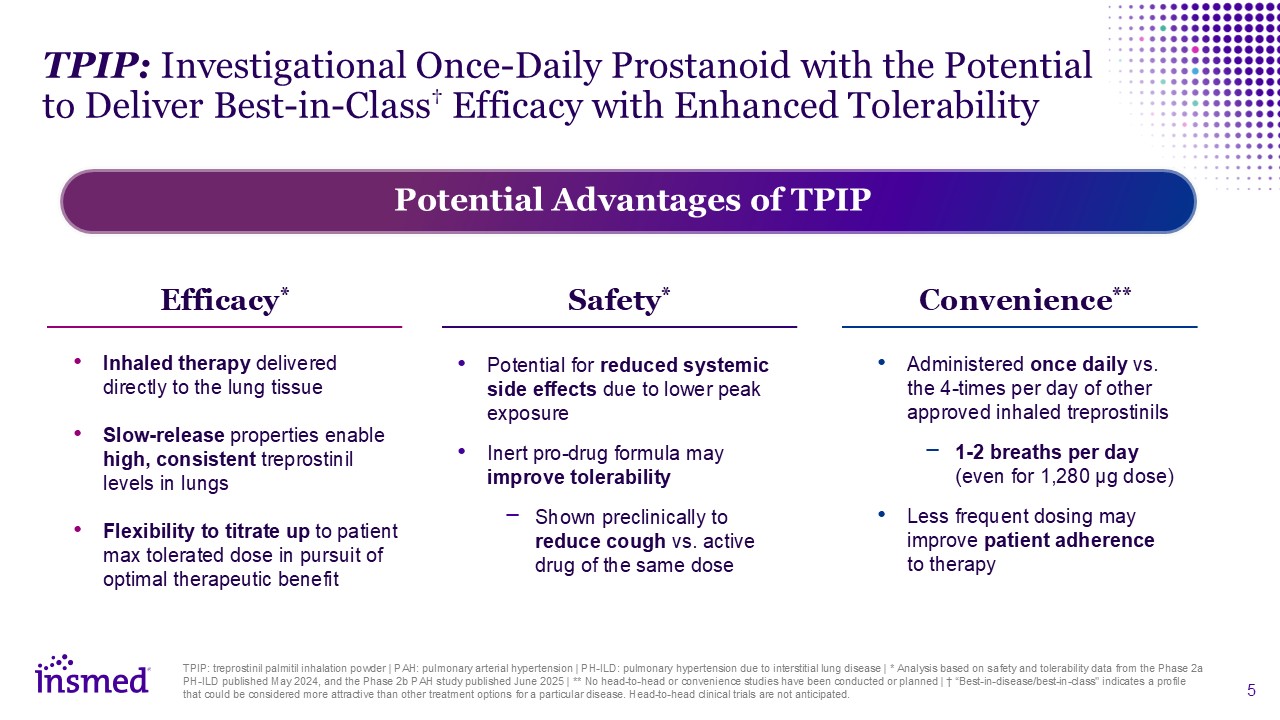
TPIP: Investigational Once-Daily Prostanoid with the Potential to Deliver
Best-in-Class† Efficacy with Enhanced Tolerability TPIP: treprostinil palmitil inhalation powder | PAH: pulmonary arterial hypertension | PH-ILD: pulmonary hypertension due to interstitial lung disease | * Analysis based on safety and
tolerability data from the Phase 2a PH-ILD published May 2024, and the Phase 2b PAH study published June 2025 | ** No head-to-head or convenience studies have been conducted or planned | † “Best-in-disease/best-in-class" indicates a profile
that could be considered more attractive than other treatment options for a particular disease. Head-to-head clinical trials are not anticipated. Potential Advantages of TPIP Efficacy* Inhaled therapy delivered directly to the lung
tissue Slow-release properties enable high, consistent treprostinil levels in lungs Flexibility to titrate up to patient max tolerated dose in pursuit of optimal therapeutic benefit Safety* Potential for reduced systemic side effects due to
lower peak exposure Inert pro-drug formula may improve tolerability Shown preclinically to reduce cough vs. active drug of the same dose Convenience** Administered once daily vs. the 4-times per day of other approved inhaled
treprostinils 1-2 breaths per day (even for 1,280 µg dose) Less frequent dosing may improve patient adherence to therapy
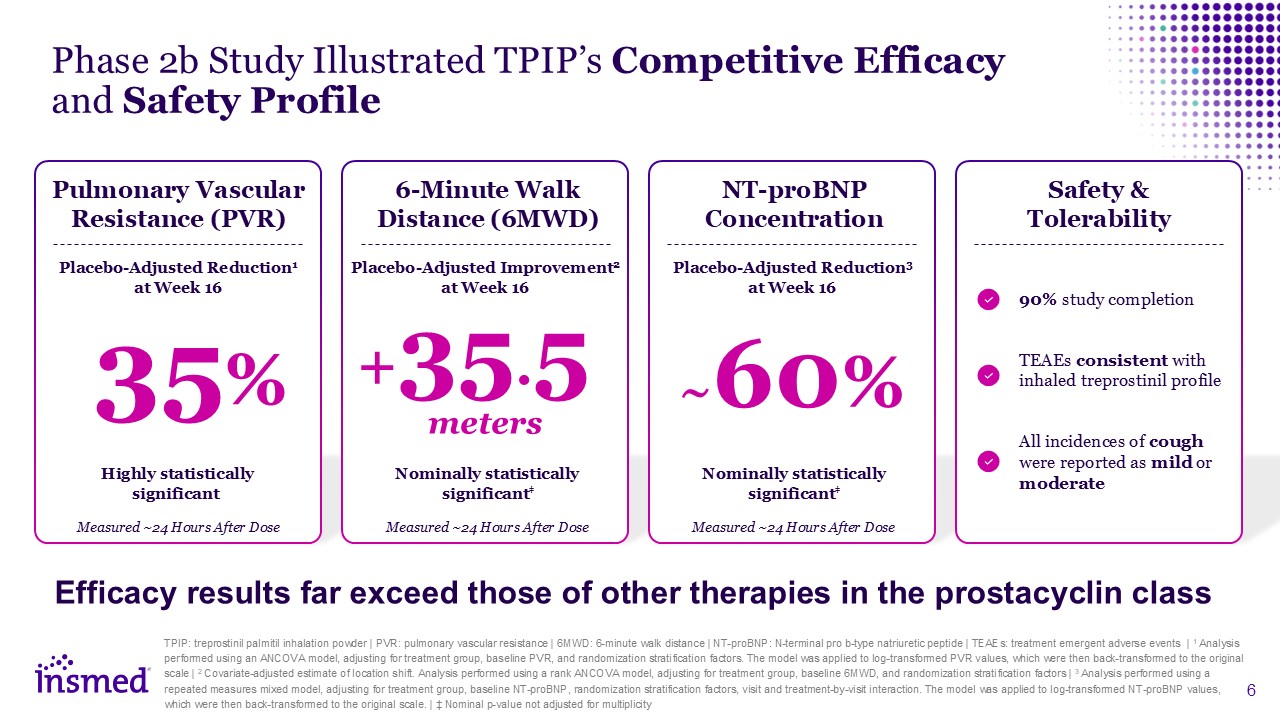
TPIP: treprostinil palmitil inhalation powder | PVR: pulmonary vascular resistance
| 6MWD: 6-minute walk distance | NT-proBNP: N-terminal pro b-type natriuretic peptide | TEAEs: treatment emergent adverse events | 1 Analysis performed using an ANCOVA model, adjusting for treatment group, baseline PVR, and randomization
stratification factors. The model was applied to log-transformed PVR values, which were then back-transformed to the original scale | 2 Covariate-adjusted estimate of location shift. Analysis performed using a rank ANCOVA model, adjusting for
treatment group, baseline 6MWD, and randomization stratification factors | 3 Analysis performed using a repeated measures mixed model, adjusting for treatment group, baseline NT-proBNP, randomization stratification factors, visit and
treatment-by-visit interaction. The model was applied to log-transformed NT-proBNP values, which were then back-transformed to the original scale. | ‡ Nominal p-value not adjusted for multiplicity Phase 2b Study Illustrated TPIP’s Competitive
Efficacy and Safety Profile 6-Minute Walk Distance (6MWD) Placebo-Adjusted Improvement2 at Week 16 Nominally statistically significant‡ +35.5 meters Safety & Tolerability 90% study completion TEAEs consistent with inhaled
treprostinil profile All incidences of cough were reported as mild or moderate Pulmonary Vascular Resistance (PVR) 35% Placebo-Adjusted Reduction1 at Week 16 Highly statistically significant Efficacy results far exceed those of other
therapies in the prostacyclin class Measured ~24 Hours After Dose Measured ~24 Hours After Dose NT-proBNP Concentration Placebo-Adjusted Reduction3 at Week 16 Nominally statistically significant‡ ~60% Measured ~24 Hours After Dose
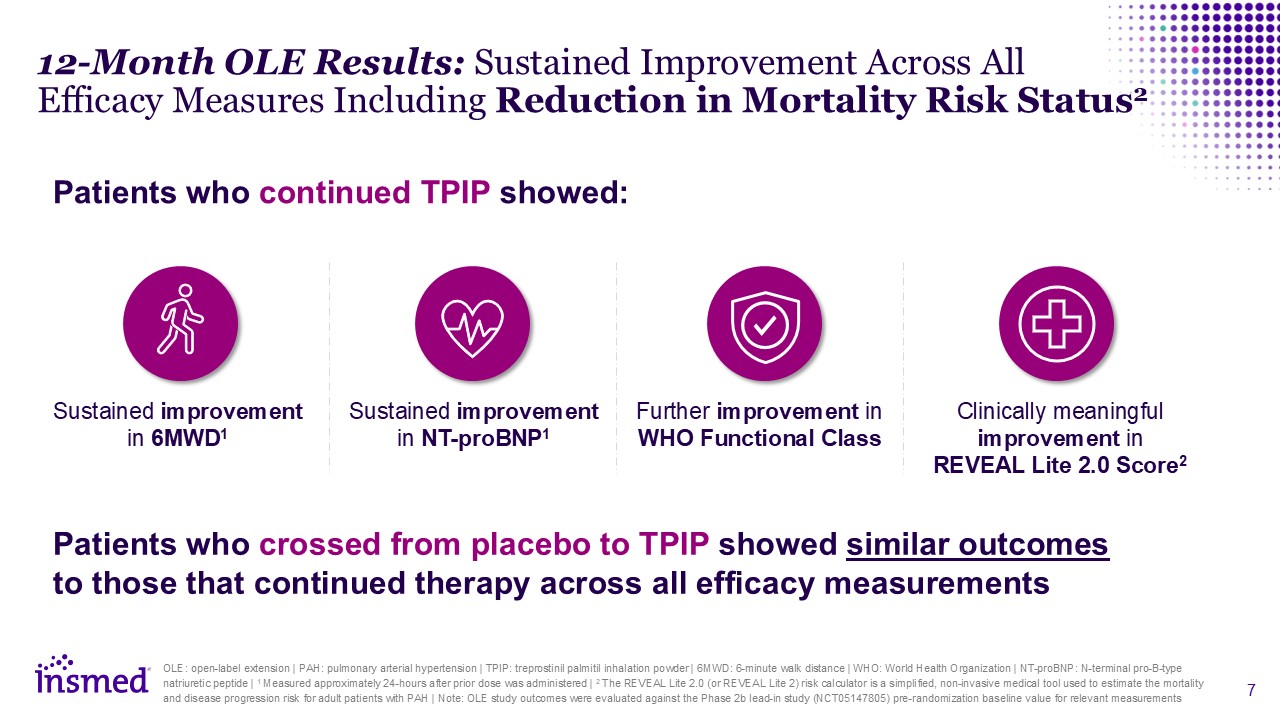
12-Month OLE Results: Sustained Improvement Across All Efficacy Measures Including
Reduction in Mortality Risk Status2 OLE: open-label extension | PAH: pulmonary arterial hypertension | TPIP: treprostinil palmitil inhalation powder | 6MWD: 6-minute walk distance | WHO: World Health Organization | NT-proBNP: N-terminal
pro-B-type natriuretic peptide | 1 Measured approximately 24-hours after prior dose was administered | 2 The REVEAL Lite 2.0 (or REVEAL Lite 2) risk calculator is a simplified, non-invasive medical tool used to estimate the mortality and
disease progression risk for adult patients with PAH | Note: OLE study outcomes were evaluated against the Phase 2b lead-in study (NCT05147805) pre-randomization baseline value for relevant measurements Patients who continued TPIP
showed: Sustained improvement in 6MWD1 Sustained improvement in NT-proBNP1 Further improvement in WHO Functional Class Clinically meaningful improvement in REVEAL Lite 2.0 Score2 Patients who crossed from placebo to TPIP showed
similar outcomes to those that continued therapy across all efficacy measurements
Study Results Gene Sullivan | Chief Product Strategy Officer
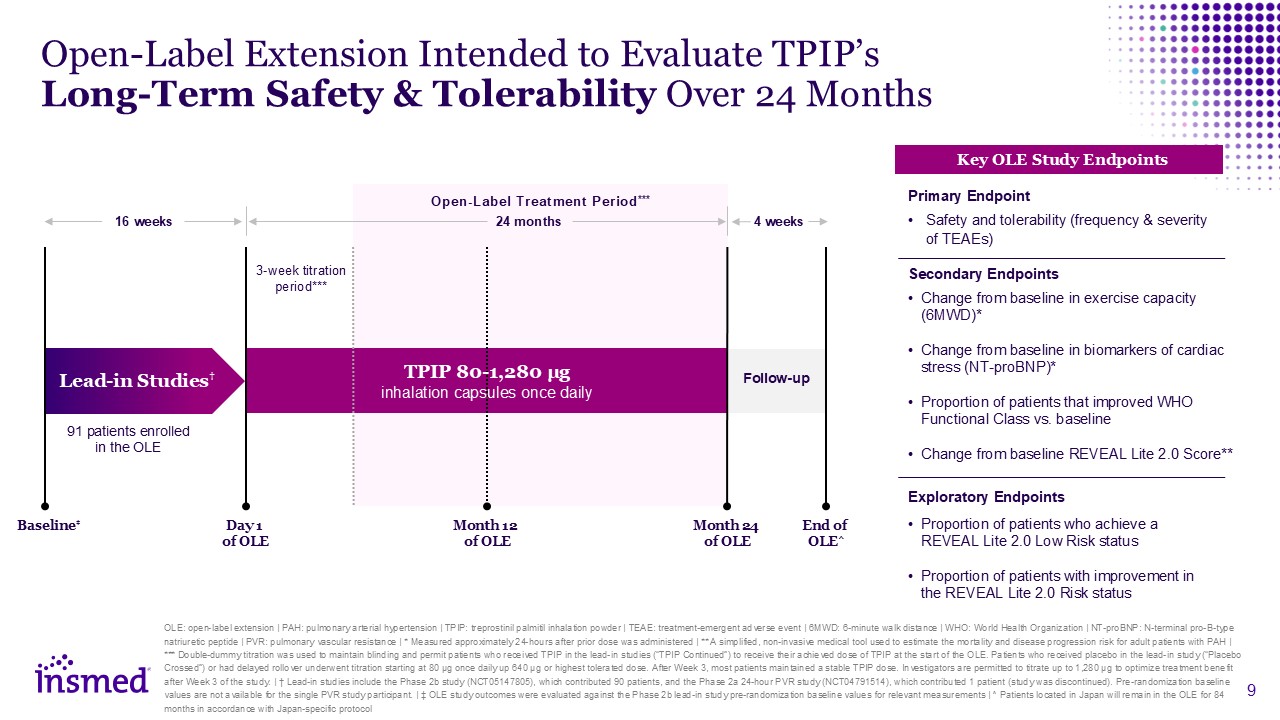
Open-Label Extension Intended to Evaluate TPIP’s Long-Term Safety &
Tolerability Over 24 Months Safety and tolerability (frequency & severity of TEAEs) Change from baseline in exercise capacity (6MWD)* Change from baseline in biomarkers of cardiac stress (NT-proBNP)* Proportion of patients that improved
WHO Functional Class vs. baseline Change from baseline REVEAL Lite 2.0 Score** Key OLE Study Endpoints Proportion of patients who achieve a REVEAL Lite 2.0 Low Risk status Proportion of patients with improvement in the REVEAL Lite 2.0 Risk
status Primary Endpoint Secondary Endpoints Exploratory Endpoints OLE: open-label extension | PAH: pulmonary arterial hypertension | TPIP: treprostinil palmitil inhalation powder | TEAE: treatment-emergent adverse event | 6MWD: 6-minute
walk distance | WHO: World Health Organization | NT-proBNP: N-terminal pro-B-type natriuretic peptide | PVR: pulmonary vascular resistance | * Measured approximately 24-hours after prior dose was administered | ** A simplified, non-invasive
medical tool used to estimate the mortality and disease progression risk for adult patients with PAH | *** Double-dummy titration was used to maintain blinding and permit patients who received TPIP in the lead-in studies (“TPIP Continued”) to
receive their achieved dose of TPIP at the start of the OLE. Patients who received placebo in the lead-in study (“Placebo Crossed”) or had delayed rollover underwent titration starting at 80 µg once daily up 640 µg or highest tolerated dose.
After Week 3, most patients maintained a stable TPIP dose. Investigators are permitted to titrate up to 1,280 µg to optimize treatment benefit after Week 3 of the study. | † Lead-in studies include the Phase 2b study (NCT05147805), which
contributed 90 patients, and the Phase 2a 24-hour PVR study (NCT04791514), which contributed 1 patient (study was discontinued). Pre-randomization baseline values are not available for the single PVR study participant. | ‡ OLE study outcomes
were evaluated against the Phase 2b lead-in study pre-randomization baseline values for relevant measurements | ^ Patients located in Japan will remain in the OLE for 84 months in accordance with Japan-specific protocol 4 weeks 24 months Day
1 of OLE End of OLE^ 16 weeks Follow-up Lead-in Studies† 3-week titration period*** Month 24 of OLE Baseline‡ Month 12 of OLE TPIP 80-1,280 µg inhalation capsules once daily Open-Label Treatment Period*** 91 patients
enrolled in the OLE
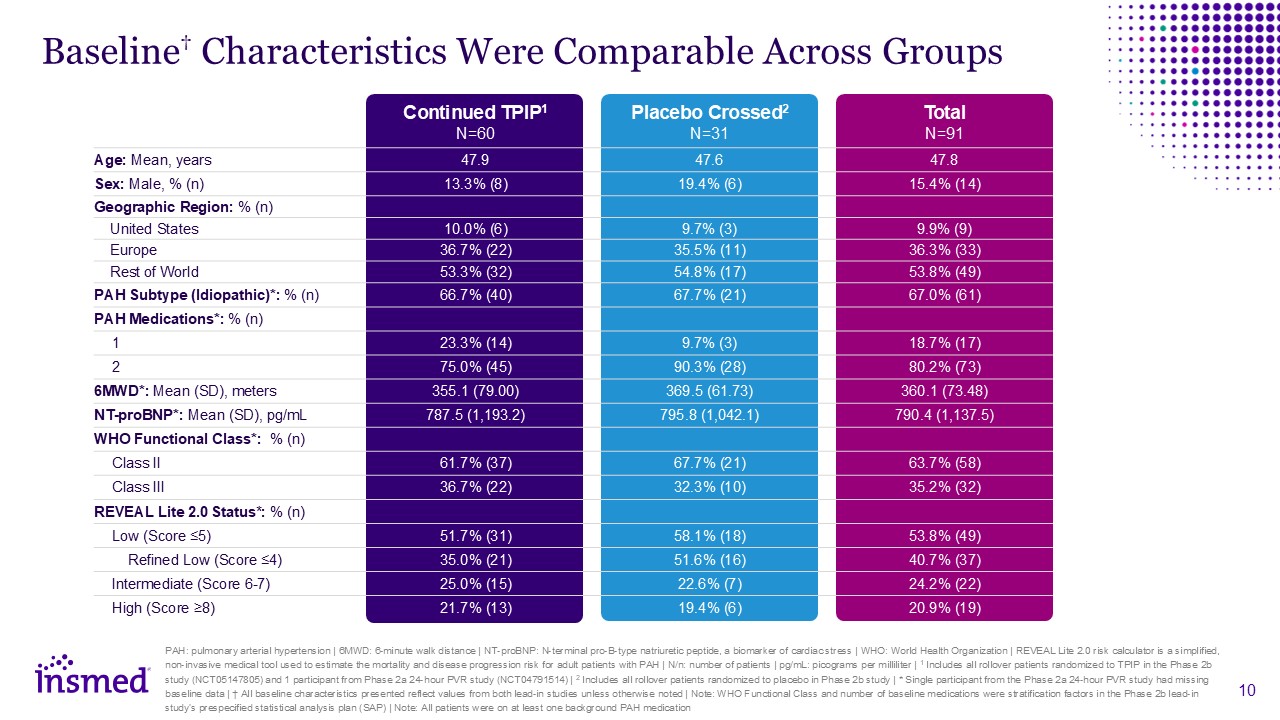
Baseline† Characteristics Were Comparable Across Groups Continued
TPIP1N=60 Placebo Crossed2N=31 Total N=91 Age: Mean, years 47.9 47.6 47.8 Sex: Male, % (n) 13.3% (8) 19.4% (6) 15.4% (14) Geographic Region: % (n) United States 10.0% (6) 9.7% (3) 9.9% (9) Europe 36.7% (22) 35.5%
(11) 36.3% (33) Rest of World 53.3% (32) 54.8% (17) 53.8% (49) PAH Subtype (Idiopathic)*: % (n) 66.7% (40) 67.7% (21) 67.0% (61) PAH Medications*: % (n) 1 23.3% (14) 9.7% (3) 18.7% (17) 2 75.0% (45) 90.3% (28) 80.2%
(73) 6MWD*: Mean (SD), meters 355.1 (79.00) 369.5 (61.73) 360.1 (73.48) NT-proBNP*: Mean (SD), pg/mL 787.5 (1,193.2) 795.8 (1,042.1) 790.4 (1,137.5) WHO Functional Class*: % (n) Class II 61.7% (37) 67.7% (21) 63.7% (58) Class
III 36.7% (22) 32.3% (10) 35.2% (32) REVEAL Lite 2.0 Status*: % (n) Low (Score ≤5) 51.7% (31) 58.1% (18) 53.8% (49) Refined Low (Score ≤4) 35.0% (21) 51.6% (16) 40.7% (37) Intermediate (Score 6-7) 25.0% (15) 22.6% (7) 24.2%
(22) High (Score ≥8) 21.7% (13) 19.4% (6) 20.9% (19) PAH: pulmonary arterial hypertension | 6MWD: 6-minute walk distance | NT-proBNP: N-terminal pro-B-type natriuretic peptide, a biomarker of cardiac stress | WHO: World Health Organization
| REVEAL Lite 2.0 risk calculator is a simplified, non-invasive medical tool used to estimate the mortality and disease progression risk for adult patients with PAH | N/n: number of patients | pg/mL: picograms per milliliter | 1 Includes all
rollover patients randomized to TPIP in the Phase 2b study (NCT05147805) and 1 participant from Phase 2a 24-hour PVR study (NCT04791514) | 2 Includes all rollover patients randomized to placebo in Phase 2b study | * Single participant from the
Phase 2a 24-hour PVR study had missing baseline data | † All baseline characteristics presented reflect values from both lead-in studies unless otherwise noted | Note: WHO Functional Class and number of baseline medications were stratification
factors in the Phase 2b lead-in study’s prespecified statistical analysis plan (SAP) | Note: All patients were on at least one background PAH medication
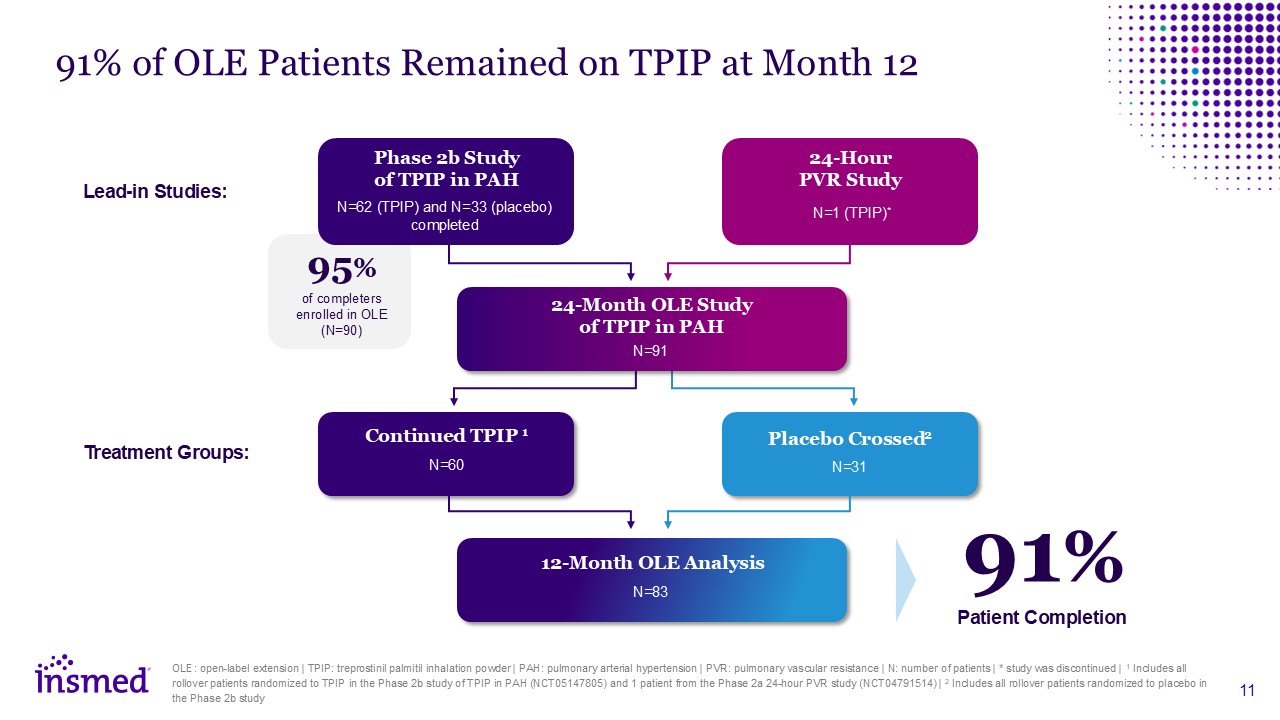
91% of OLE Patients Remained on TPIP at Month 12 OLE: open-label extension |
TPIP: treprostinil palmitil inhalation powder | PAH: pulmonary arterial hypertension | PVR: pulmonary vascular resistance | N: number of patients | * study was discontinued | 1 Includes all rollover patients randomized to TPIP in the Phase 2b
study of TPIP in PAH (NCT05147805) and 1 patient from the Phase 2a 24-hour PVR study (NCT04791514) | 2 Includes all rollover patients randomized to placebo in the Phase 2b study Phase 2b Study of TPIP in PAH N=62 (TPIP) and N=33 (placebo)
completed 24-Hour PVR Study N=1 (TPIP)* 24-Month OLE Study of TPIP in PAH N=91 Continued TPIP 1 N=60 Placebo Crossed2 N=31 12-Month OLE Analysis Lead-in Studies: N=83 95% of completers enrolled in OLE (N=90) 91% Patient
Completion Treatment Groups:
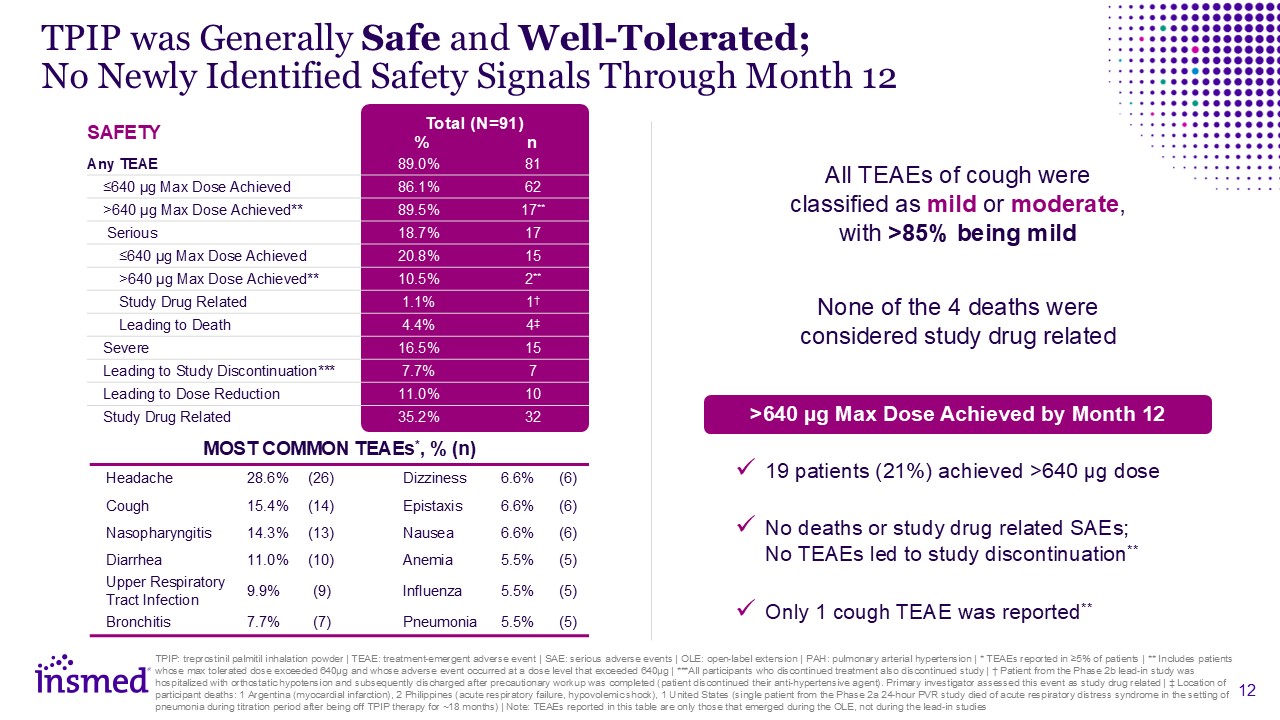
TPIP was Generally Safe and Well-Tolerated;No Newly Identified Safety Signals
Through Month 12 SAFETY Total (N=91) % n Any TEAE 89.0% 81 ≤640 µg Max Dose Achieved 86.1% 62 >640 µg Max Dose Achieved** 89.5% 17** Serious 18.7% 17 ≤640 µg Max Dose Achieved 20.8% 15 >640 µg Max Dose
Achieved** 10.5% 2** Study Drug Related 1.1% 1† Leading to Death 4.4% 4‡ Severe 16.5% 15 Leading to Study Discontinuation*** 7.7% 7 Leading to Dose Reduction 11.0% 10 Study Drug Related 35.2% 32 TPIP: treprostinil
palmitil inhalation powder | TEAE: treatment-emergent adverse event | SAE: serious adverse events | OLE: open-label extension | PAH: pulmonary arterial hypertension | * TEAEs reported in ≥5% of patients | ** Includes patients whose max
tolerated dose exceeded 640µg and whose adverse event occurred at a dose level that exceeded 640µg | ***All participants who discontinued treatment also discontinued study | † Patient from the Phase 2b lead-in study was hospitalized with
orthostatic hypotension and subsequently discharged after precautionary workup was completed (patient discontinued their anti-hypertensive agent). Primary investigator assessed this event as study drug related | ‡ Location of participant
deaths: 1 Argentina (myocardial infarction), 2 Philippines (acute respiratory failure, hypovolemic shock), 1 United States (single patient from the Phase 2a 24-hour PVR study died of acute respiratory distress syndrome in the setting of
pneumonia during titration period after being off TPIP therapy for ~18 months) | Note: TEAEs reported in this table are only those that emerged during the OLE, not during the lead-in studies MOST COMMON TEAEs*, % (n) Headache 28.6%
(26) Dizziness 6.6% (6) Cough 15.4% (14) Epistaxis 6.6% (6) Nasopharyngitis 14.3% (13) Nausea 6.6% (6) Diarrhea 11.0% (10) Anemia 5.5% (5) Upper Respiratory Tract Infection 9.9% (9) Influenza 5.5%
(5) Bronchitis 7.7% (7) Pneumonia 5.5% (5) 19 patients (21%) achieved >640 µg dose No deaths or study drug related SAEs; No TEAEs led to study discontinuation** Only 1 cough TEAE was reported** >640 µg Max Dose Achieved by
Month 12 None of the 4 deaths were considered study drug related All TEAEs of cough were classified as mild or moderate, with >85% being mild
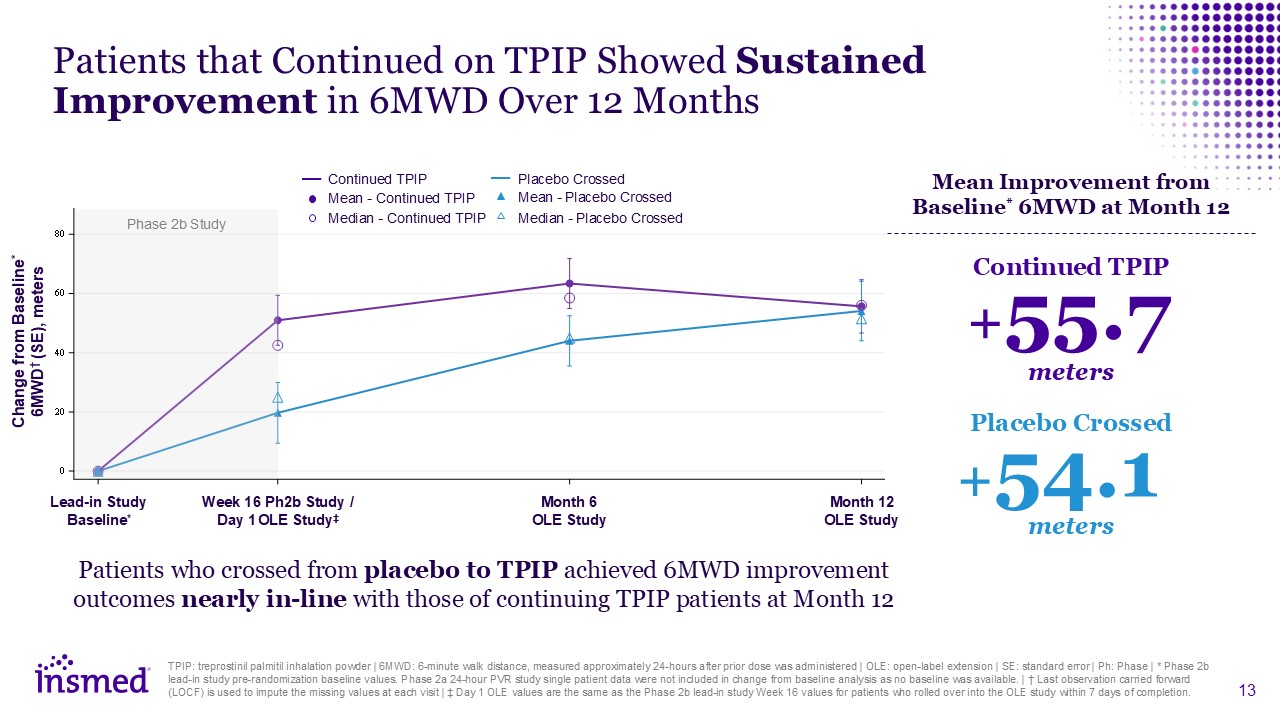
Patients that Continued on TPIP Showed Sustained Improvement in 6MWD Over 12
Months Change from Baseline* 6MWD† (SE), meters Lead-in Study Baseline* Week 16 Ph2b Study / Day 1 OLE Study‡ Month 6 OLE Study Month 12 OLE Study +55.7 Continued TPIP meters +54.1 Placebo Crossed meters Mean Improvement from
Baseline* 6MWD at Month 12 Patients who crossed from placebo to TPIP achieved 6MWD improvement outcomes nearly in-line with those of continuing TPIP patients at Month 12 TPIP: treprostinil palmitil inhalation powder | 6MWD: 6-minute walk
distance, measured approximately 24-hours after prior dose was administered | OLE: open-label extension | SE: standard error | Ph: Phase | * Phase 2b lead-in study pre-randomization baseline values. Phase 2a 24-hour PVR study single patient
data were not included in change from baseline analysis as no baseline was available. | † Last observation carried forward (LOCF) is used to impute the missing values at each visit | ‡ Day 1 OLE values are the same as the Phase 2b lead-in study
Week 16 values for patients who rolled over into the OLE study within 7 days of completion. Continued TPIP Placebo Crossed Median - Continued TPIP Median - Placebo Crossed Mean - Placebo Crossed Mean - Continued TPIP Phase 2b Study
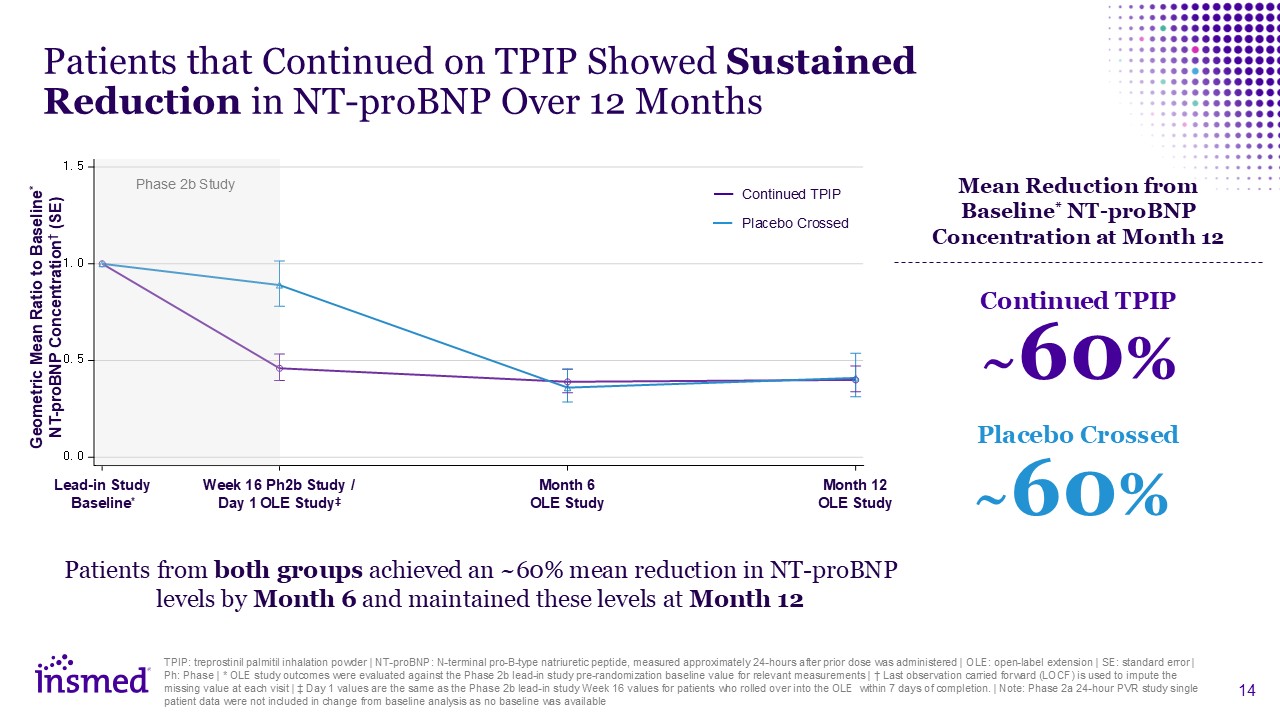
Patients that Continued on TPIP Showed Sustained Reduction in NT-proBNP Over 12
Months Geometric Mean Ratio to Baseline* NT-proBNP Concentration† (SE) Mean Reduction from Baseline* NT-proBNP Concentration at Month 12 TPIP: treprostinil palmitil inhalation powder | NT-proBNP: N-terminal pro-B-type natriuretic
peptide, measured approximately 24-hours after prior dose was administered | OLE: open-label extension | SE: standard error | Ph: Phase | * OLE study outcomes were evaluated against the Phase 2b lead-in study pre-randomization baseline value
for relevant measurements | † Last observation carried forward (LOCF) is used to impute the missing value at each visit | ‡ Day 1 values are the same as the Phase 2b lead-in study Week 16 values for patients who rolled over into the OLE within
7 days of completion. | Note: Phase 2a 24-hour PVR study single patient data were not included in change from baseline analysis as no baseline was available Patients from both groups achieved an ~60% mean reduction in NT-proBNP levels by Month
6 and maintained these levels at Month 12 Continued TPIP Placebo Crossed ~60% Continued TPIP ~60% Placebo Crossed Phase 2b Study Lead-in Study Baseline* Week 16 Ph2b Study / Day 1 OLE Study‡ Month 6 OLE Study Month 12 OLE Study
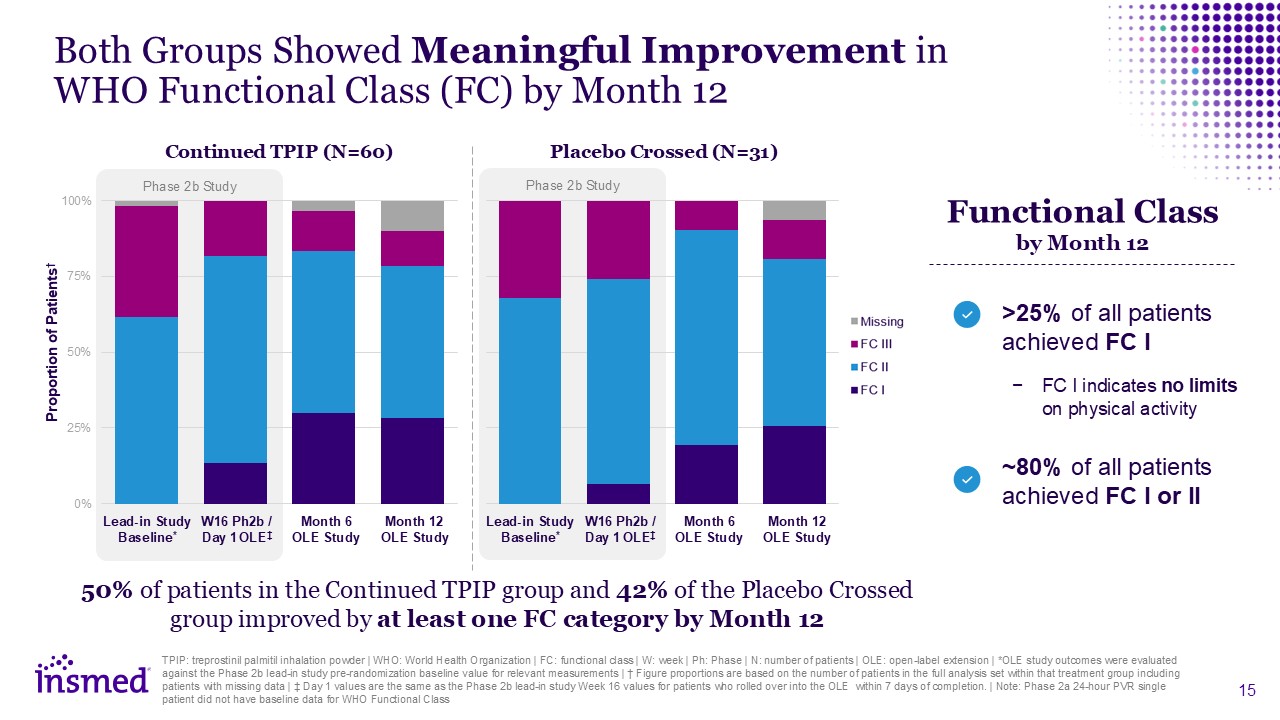
Lead-in Study Baseline* Month 6 OLE Study Month 12 OLE Study Both Groups
Showed Meaningful Improvement in WHO Functional Class (FC) by Month 12 Continued TPIP (N=60) Placebo Crossed (N=31) Proportion of Patients† ~80% of all patients achieved FC I or II Functional Class by Month 12 >25% of all patients
achieved FC I FC I indicates no limits on physical activity TPIP: treprostinil palmitil inhalation powder | WHO: World Health Organization | FC: functional class | W: week | Ph: Phase | N: number of patients | OLE: open-label extension |
*OLE study outcomes were evaluated against the Phase 2b lead-in study pre-randomization baseline value for relevant measurements | † Figure proportions are based on the number of patients in the full analysis set within that treatment group
including patients with missing data | ‡ Day 1 values are the same as the Phase 2b lead-in study Week 16 values for patients who rolled over into the OLE within 7 days of completion. | Note: Phase 2a 24-hour PVR single patient did not have
baseline data for WHO Functional Class Phase 2b Study Lead-in Study Baseline* Month 6 OLE Study Month 12 OLE Study Phase 2b Study W16 Ph2b / Day 1 OLE‡ W16 Ph2b / Day 1 OLE‡ 50% of patients in the Continued TPIP group and 42% of
the Placebo Crossed group improved by at least one FC category by Month 12
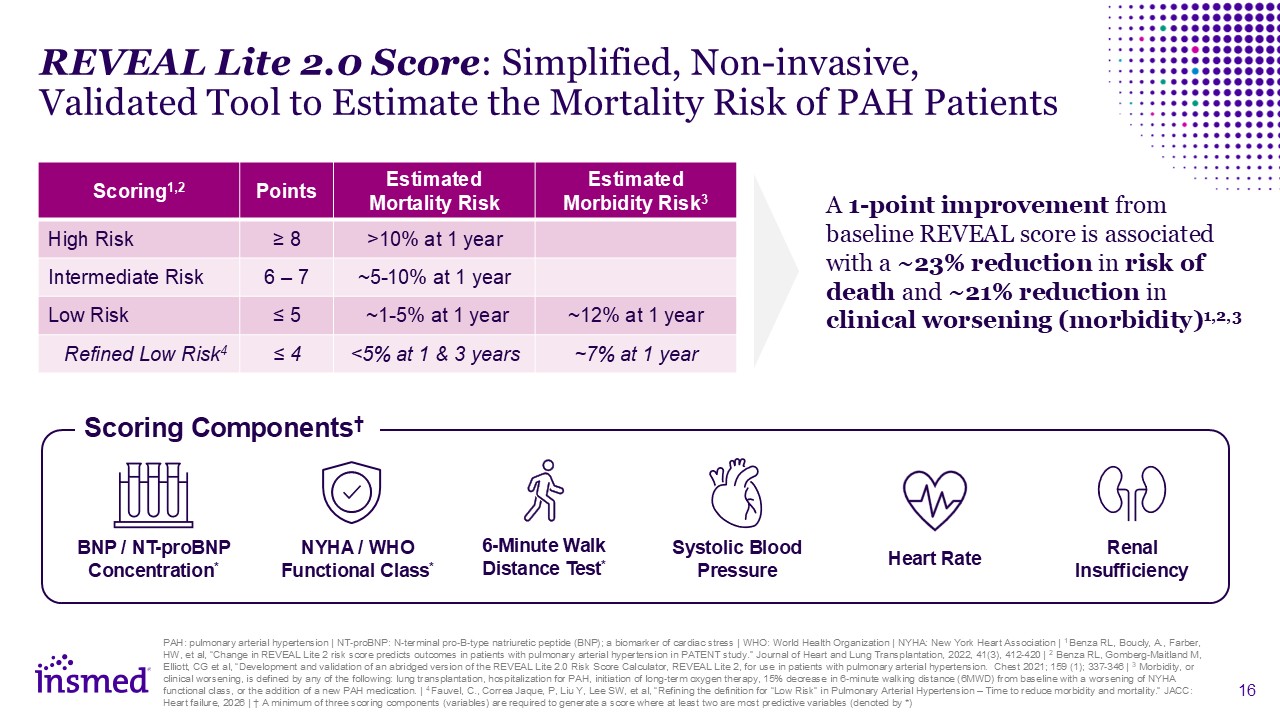
Scoring Components† REVEAL Lite 2.0 Score: Simplified, Non-invasive, Validated
Tool to Estimate the Mortality Risk of PAH Patients Scoring1,2 Points Estimated Mortality Risk Estimated Morbidity Risk3 High Risk ≥ 8 >10% at 1 year Intermediate Risk 6 – 7 ~5-10% at 1 year Low Risk ≤ 5 ~1-5% at 1 year ~12%
at 1 year Refined Low Risk4 ≤ 4 <5% at 1 & 3 years ~7% at 1 year A 1-point improvement from baseline REVEAL score is associated with a ~23% reduction in risk of death and ~21% reduction in clinical worsening (morbidity)1,2,3 PAH:
pulmonary arterial hypertension | NT-proBNP: N-terminal pro-B-type natriuretic peptide (BNP); a biomarker of cardiac stress | WHO: World Health Organization | NYHA: New York Heart Association | 1 Benza RL, Boucly, A., Farber, HW, et al, “Change
in REVEAL Lite 2 risk score predicts outcomes in patients with pulmonary arterial hypertension in PATENT study.” Journal of Heart and Lung Transplantation, 2022, 41(3), 412-420 | 2 Benza RL, Gomberg-Maitland M, Elliott, CG et al, “Development
and validation of an abridged version of the REVEAL Lite 2.0 Risk Score Calculator, REVEAL Lite 2, for use in patients with pulmonary arterial hypertension. Chest 2021; 159 (1); 337-346 | 3 Morbidity, or clinical worsening, is defined by any of
the following: lung transplantation, hospitalization for PAH, initiation of long-term oxygen therapy, 15% decrease in 6-minute walking distance (6MWD) from baseline with a worsening of NYHA functional class, or the addition of a new PAH
medication. | 4 Fauvel, C., Correa Jaque, P, Liu Y, Lee SW, et al, “Refining the definition for “Low Risk” in Pulmonary Arterial Hypertension – Time to reduce morbidity and mortality.” JACC: Heart failure, 2026 | † A minimum of three scoring
components (variables) are required to generate a score where at least two are most predictive variables (denoted by *) NYHA / WHO Functional Class* 6-Minute Walk Distance Test* Renal Insufficiency Heart Rate Systolic Blood Pressure BNP
/ NT-proBNP Concentration*
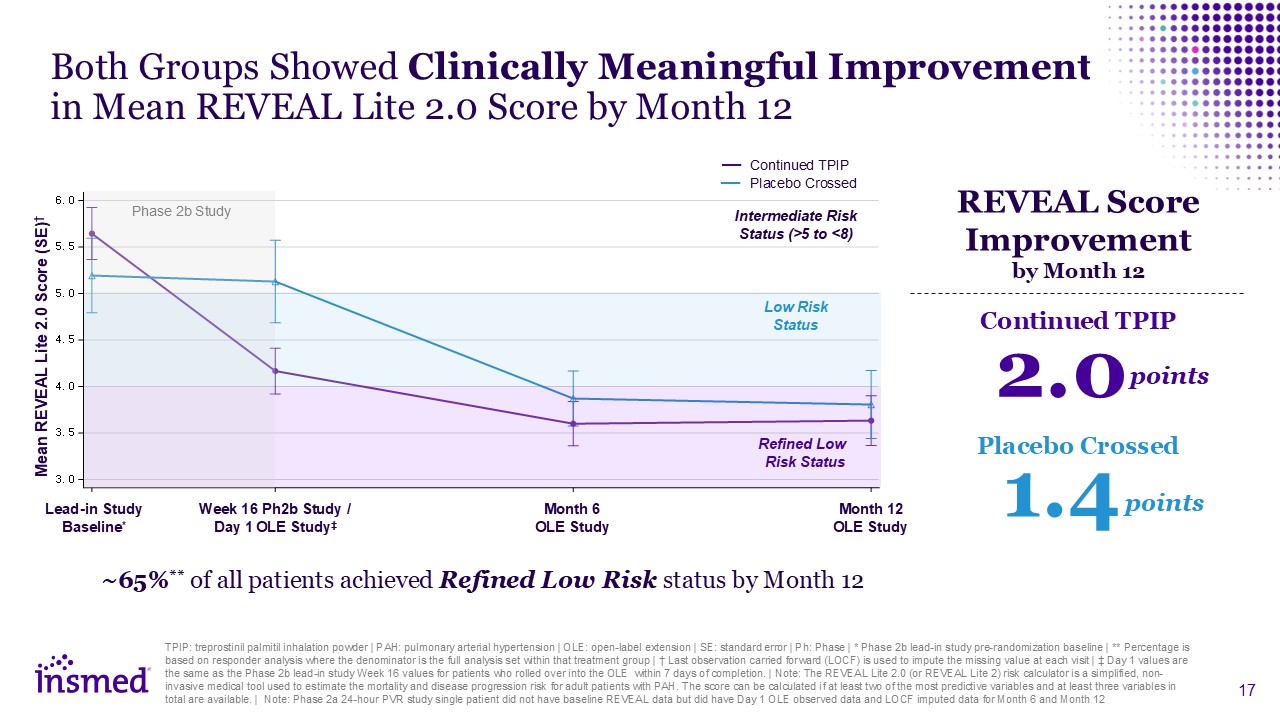
Both Groups Showed Clinically Meaningful Improvement in Mean REVEAL Lite 2.0 Score
by Month 12 Mean REVEAL Lite 2.0 Score (SE)† ~65%** of all patients achieved Refined Low Risk status by Month 12 REVEAL Score Improvement by Month 12 TPIP: treprostinil palmitil inhalation powder | PAH: pulmonary arterial hypertension |
OLE: open-label extension | SE: standard error | Ph: Phase | * Phase 2b lead-in study pre-randomization baseline | ** Percentage is based on responder analysis where the denominator is the full analysis set within that treatment group | † Last
observation carried forward (LOCF) is used to impute the missing value at each visit | ‡ Day 1 values are the same as the Phase 2b lead-in study Week 16 values for patients who rolled over into the OLE within 7 days of completion. | Note: The
REVEAL Lite 2.0 (or REVEAL Lite 2) risk calculator is a simplified, non-invasive medical tool used to estimate the mortality and disease progression risk for adult patients with PAH. The score can be calculated if at least two of the most
predictive variables and at least three variables in total are available. | Note: Phase 2a 24-hour PVR study single patient did not have baseline REVEAL data but did have Day 1 OLE observed data and LOCF imputed data for Month 6 and Month
12 Refined Low Risk Status Low Risk Status Intermediate Risk Status (>5 to <8) Phase 2b Study Continued TPIP Placebo Crossed Lead-in Study Baseline* Week 16 Ph2b Study / Day 1 OLE Study‡ Month 6 OLE Study Month 12 OLE
Study Continued TPIP Placebo Crossed 2.0 points 1.4 points
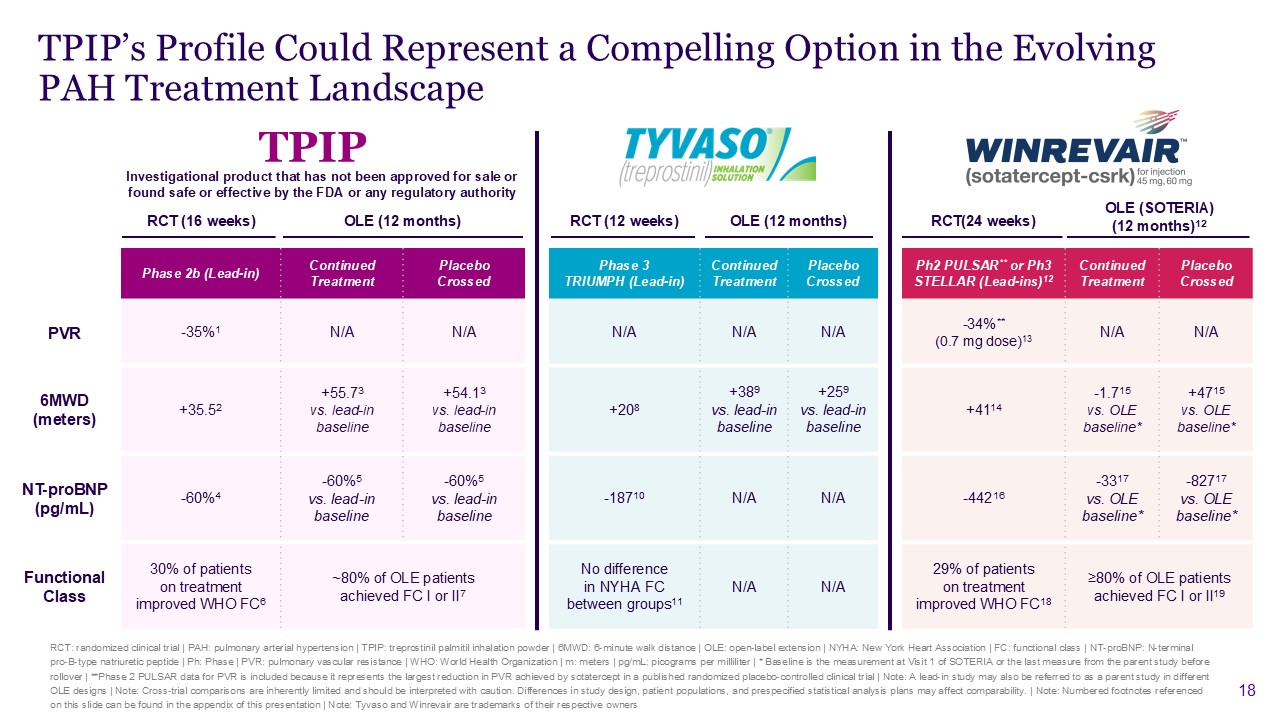
RCT: randomized clinical trial | PAH: pulmonary arterial hypertension | TPIP:
treprostinil palmitil inhalation powder | 6MWD: 6-minute walk distance | OLE: open-label extension | NYHA: New York Heart Association | FC: functional class | NT-proBNP: N-terminal pro-B-type natriuretic peptide | Ph: Phase | PVR: pulmonary
vascular resistance | WHO: World Health Organization | m: meters | pg/mL: picograms per milliliter | * Baseline is the measurement at Visit 1 of SOTERIA or the last measure from the parent study before rollover | **Phase 2 PULSAR data for PVR
is included because it represents the largest reduction in PVR achieved by sotatercept in a published randomized placebo-controlled clinical trial | Note: A lead-in study may also be referred to as a parent study in different OLE designs |
Note: Cross-trial comparisons are inherently limited and should be interpreted with caution. Differences in study design, patient populations, and prespecified statistical analysis plans may affect comparability. | Note: Numbered footnotes
referenced on this slide can be found in the appendix of this presentation | Note: Tyvaso and Winrevair are trademarks of their respective owners TPIP’s Profile Could Represent a Compelling Option in the Evolving PAH Treatment Landscape RCT
(16 weeks) OLE (12 months) RCT (12 weeks) OLE (12 months) RCT(24 weeks) OLE (SOTERIA) (12 months)12 Phase 2b (Lead-in) Continued Treatment Placebo Crossed X Phase 3 TRIUMPH (Lead-in) Continued Treatment Placebo Crossed X Ph2
PULSAR** or Ph3 STELLAR (Lead-ins)12 Continued Treatment Placebo Crossed PVR -35%1 N/A N/A X N/A N/A N/A X -34%** (0.7 mg dose)13 N/A N/A 6MWD (meters) +35.52 +55.73 vs. lead-in baseline +54.13 vs. lead-in
baseline X +208 +389 vs. lead-in baseline +259 vs. lead-in baseline X +4114 -1.715 vs. OLE baseline* +4715 vs. OLE baseline* NT-proBNP (pg/mL) -60%4 -60%5 vs. lead-in baseline -60%5 vs. lead-in
baseline X -18710 N/A N/A X -44216 -3317 vs. OLE baseline* -82717 vs. OLE baseline* Functional Class 30% of patients on treatment improved WHO FC6 ~80% of OLE patients achieved FC I or II7 X No difference in NYHA FC between
groups11 N/A N/A X 29% of patients on treatment improved WHO FC18 ≥80% of OLE patients achieved FC I or II19 TPIP Investigational product that has not been approved for sale or found safe or effective by the FDA or any regulatory
authority

KOL Reflection Dr. Raymond Benza MD, FACC, FAHA, FACP George M. and Linda H.
Kaufman Academic Chair of Cardiology, Sentara Health Phase 2b PAH study Steering Committee KOL: key opinion leader | MD: Doctor of Medicine | FACC: Fellow of the American College of Cardiology | FAHA: Fellow of the American Heart Association
| FACP: Fellow of the American College of Physicians | PAH: pulmonary arterial hypertension
These Results, Combined with Once-Daily Inhaled Profile, Reinforce TPIP’s
Potential to Become the Prostanoid of Choice Sustained improvements for patients remaining on TPIP and comparable benefits for patients who switched from placebo TPIP treatment led to meaningful reductions from baseline in REVEAL Lite 2.0
scores, a validated mortality risk assessment tool TPIP continued to demonstrate a favorable safety & tolerability profile with a low rate of cough (15%*, of which 85% was classified as mild) OLE: open-label extension | TPIP: treprostinil
palmitil inhalation powder | PAH: pulmonary arterial hypertension | The REVEAL Lite 2.0 (or REVEAL Lite 2) risk calculator is a simplified, non-invasive medical tool used to estimate the mortality and disease progression risk for adult patients
with PAH | TEAE: treatment-emergent adverse events | * Includes cough TEAEs that emerged after the first dose of the study drug was administered in the OLE (does not include TEAEs that emerged during the lead-in studies)
Next Steps: Design and Conduct an Expansive Registrational Program Across Four
Indications PAH: pulmonary arterial hypertension | PH-ILD: pulmonary hypertension due to interstitial lung disease | PPF: progressive pulmonary fibrosis | IPF: idiopathic pulmonary fibrosis | Q: quarter | H: half | TPIP: treprostinil palmitil
inhalation powder | Note: Initiation indicates that trial sites are open and ready to screen patients for enrollment PH-ILD IPF PPF PAH TPIP Phase 3 patient enrollment progressing Phase 3 first trial sites actively screening Phase 3
initiation expected 2H:26 Phase 3 initiation expected 1H:27

Q&A Session Will Lewis Chair & CEO Sara Bonstein Chief Financial
Officer Martina Flammer Chief Medical Officer Gene Sullivan Chief Product Strategy Officer Thank you to the patients and investigators participating in this study! Dr. Raymond Benza George M. and Linda H. Kaufman Academic Chair of
Cardiology, Sentara Health

Appendix
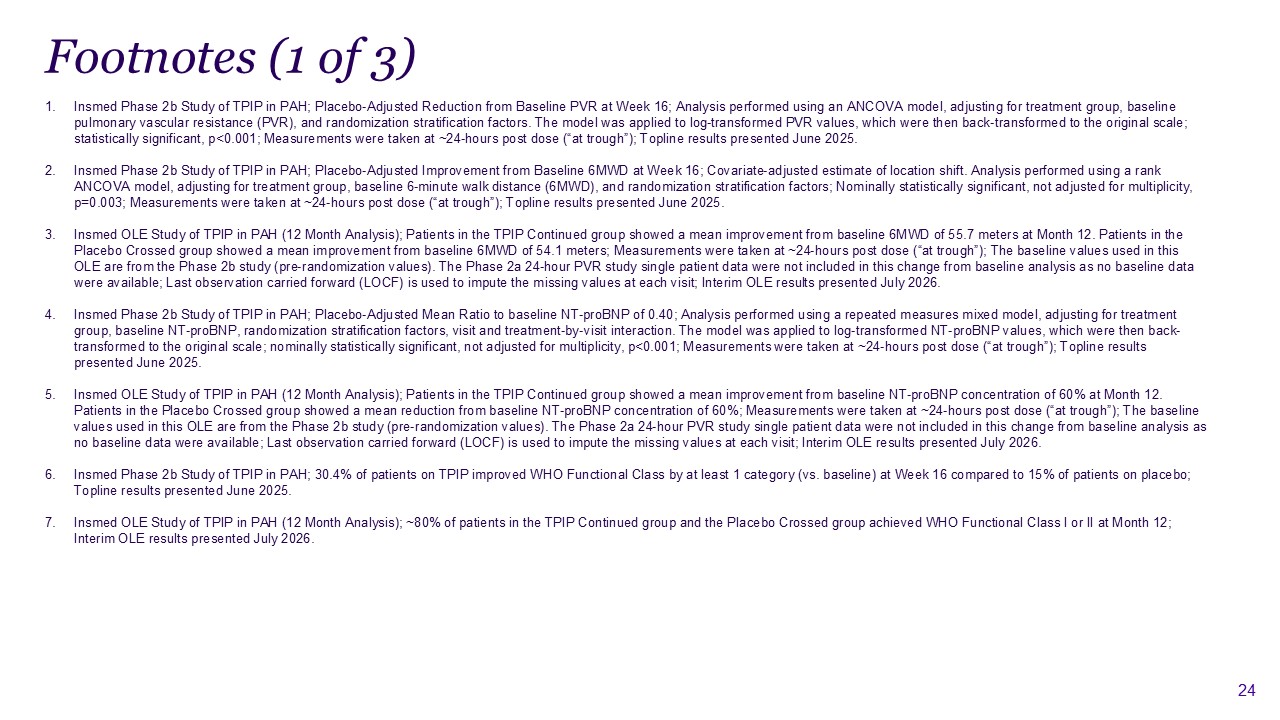
Footnotes (1 of 3) Insmed Phase 2b Study of TPIP in PAH; Placebo-Adjusted
Reduction from Baseline PVR at Week 16; Analysis performed using an ANCOVA model, adjusting for treatment group, baseline pulmonary vascular resistance (PVR), and randomization stratification factors. The model was applied to log-transformed
PVR values, which were then back-transformed to the original scale; statistically significant, p<0.001; Measurements were taken at ~24-hours post dose (“at trough”); Topline results presented June 2025. Insmed Phase 2b Study of TPIP in PAH;
Placebo-Adjusted Improvement from Baseline 6MWD at Week 16; Covariate-adjusted estimate of location shift. Analysis performed using a rank ANCOVA model, adjusting for treatment group, baseline 6-minute walk distance (6MWD), and randomization
stratification factors; Nominally statistically significant, not adjusted for multiplicity, p=0.003; Measurements were taken at ~24-hours post dose (“at trough”); Topline results presented June 2025. Insmed OLE Study of TPIP in PAH (12 Month
Analysis); Patients in the TPIP Continued group showed a mean improvement from baseline 6MWD of 55.7 meters at Month 12. Patients in the Placebo Crossed group showed a mean improvement from baseline 6MWD of 54.1 meters; Measurements were taken
at ~24-hours post dose (“at trough”); The baseline values used in this OLE are from the Phase 2b study (pre-randomization values). The Phase 2a 24-hour PVR study single patient data were not included in this change from baseline analysis as no
baseline data were available; Last observation carried forward (LOCF) is used to impute the missing values at each visit; Interim OLE results presented July 2026. Insmed Phase 2b Study of TPIP in PAH; Placebo-Adjusted Mean Ratio to baseline
NT-proBNP of 0.40; Analysis performed using a repeated measures mixed model, adjusting for treatment group, baseline NT-proBNP, randomization stratification factors, visit and treatment-by-visit interaction. The model was applied to
log-transformed NT-proBNP values, which were then back-transformed to the original scale; nominally statistically significant, not adjusted for multiplicity, p<0.001; Measurements were taken at ~24-hours post dose (“at trough”); Topline
results presented June 2025. Insmed OLE Study of TPIP in PAH (12 Month Analysis); Patients in the TPIP Continued group showed a mean improvement from baseline NT-proBNP concentration of 60% at Month 12. Patients in the Placebo Crossed group
showed a mean reduction from baseline NT-proBNP concentration of 60%; Measurements were taken at ~24-hours post dose (“at trough”); The baseline values used in this OLE are from the Phase 2b study (pre-randomization values). The Phase 2a
24-hour PVR study single patient data were not included in this change from baseline analysis as no baseline data were available; Last observation carried forward (LOCF) is used to impute the missing values at each visit; Interim OLE results
presented July 2026. Insmed Phase 2b Study of TPIP in PAH; 30.4% of patients on TPIP improved WHO Functional Class by at least 1 category (vs. baseline) at Week 16 compared to 15% of patients on placebo; Topline results presented June
2025. Insmed OLE Study of TPIP in PAH (12 Month Analysis); ~80% of patients in the TPIP Continued group and the Placebo Crossed group achieved WHO Functional Class I or II at Month 12; Interim OLE results presented July 2026.
Phase 3 TRIUMPH study; Hodges-Lehmann (H-L) median treatment difference in change
from baseline 6MWD at 12 weeks measured at peak drug exposure (p<0.001); McLaughlin, V, Benza, R, Rubin, L. et al. Addition of Inhaled Treprostinil to Oral Therapy for Pulmonary Arterial Hypertension: A Randomized Controlled Clinical Trial.
JACC. 2010 May | URL: https://doi.org/10.1016/j.jacc.2010.01.027 TRIUMPH OLE Study; Median changes in 6MWD at 6, 12, 18, and 24 months were 28, 31, 32, and 18 meters, respectively, for all participants, inclusive of the significant attrition
in median change in walk distance for those patients who initially received the placebo; Benza RL, Seeger W, McLaughlin VV, et al. Long-term effects of inhaled treprostinil in patients with pulmonary arterial hypertension: the Treprostinil
Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension (TRIUMPH) study open-label extension. J Heart Lung Transplant. 2011 | URL: https://www.tyvasohcp.com/pah/efficacy-safety/triumph-extension-study/ Phase 3 TRIUMPH
study; Hodges-Lehmann (H-L) between-treatment median difference in change from baseline NT-proBNP concentration measured at 12 weeks (p=0.0014) (ancillary endpoint); McLaughlin, V, Benza, R, Rubin, L. et al. Addition of Inhaled Treprostinil to
Oral Therapy for Pulmonary Arterial Hypertension: A Randomized Controlled Clinical Trial. JACC. 2010 May | URL: https://doi.org/10.1016/j.jacc.2010.01.027 Phase 3 TRIUMPH study; NYHA functional class was a prespecified secondary endpoint but
did not differ significantly between treatment and placebo at 12 weeks; McLaughlin, V, Benza, R, Rubin, L. et al. Addition of Inhaled Treprostinil to Oral Therapy for Pulmonary Arterial Hypertension: A Randomized Controlled Clinical Trial.
JACC. 2010 May | URL: https://doi.org/10.1016/j.jacc.2010.01.027 Footnotes (2 of 3)
SOTERIA OLE participants included eligible adults with PAH on stable background
therapy who completed a prior sotatercept study (Phase 2 or Phase 3) without early discontinuation were enrolled. Participants received subcutaneous sotatercept (≤0.7 mg dose once every 21 days). This differs from the design of the OLE studies
conducted for TYVASO and TPIP where OLE participants originated from the same lead-in (parent) study | Note on TPIP OLE: A single participant was enrolled in the OLE study from the Phase 2a 24-hour PVR study along with 90 participants from the
Phase 2b study Phase 2 PULSAR study; The greater degree of reduction in pulmonary vascular resistance as compared with placebo was seen at both dose levels of sotatercept, with the higher dose (0.7 mg dose) resulting in a 34% reduction from
baseline. Least-squares mean difference as compared with placebo -239.5 dyn.sec.cm-5 (baseline 755.9 dyn.sec.cm-5 for high dose); Humbert, M., McLaughlin, V., Gibbs, J. S. R., Gomberg-Maitland, M., Hoeper, M. M., Preston, I. R., Souza, R.,
Waxman, A., Escribano Subias, P., Feldman, J., Meyer, G., Montani, D., Olsson, K. M., Manimaran, S., Barnes, J., Linde, P. G., de Oliveira Pena, J., & Badesch, D. B. (2021). Sotatercept for the treatment of pulmonary arterial hypertension.
New England Journal of Medicine | URL: https://doi.org/10.1056/NEJMoa2024277 Phase 3 STELLAR study; Table 2. Change from Baseline at Week 24 in Primary and Secondary Efficacy End Points (Intention-to-Treat Population); The Hodges–Lehmann (H-L)
estimate of the difference between the sotatercept and placebo groups in the change from baseline at week 24 in the 6-minute walk distance was 40.8 m (p<0.001); Hoeper, M. M., Badesch, D. B., Ghofrani, H. A., et al. (2023). Phase 3 trial of
sotatercept for treatment of pulmonary arterial hypertension. New England Journal of Medicine 2023 | URL: https://doi.org/10.1056/NEJMoa2213558 SOTERIA OLE study; Supplementary Table 5. Change from Baseline at Week 24 and Year 1; Mean change
from baseline defined as measurement at Visit 1 of SOTERIA or the last measure from the parent study before rollover in 6MWD; Interim results of SOTERIA; Preston, I. R., Badesch, D. B., Ghofrani, H.-A., Hoeper, M. M., Channick, R. N., Chin, K.
M., Humbert, M., Jing, Z.-C., Lang, I. M., McLaughlin, V. V., Simonneau, G., Souza, R., Tapson, V. F., Torres, F., White, R. J., Beaufils, B., Kim, J. B., & Rubin, L. J. (2025). A long-term follow-up study of sotatercept for treatment of
pulmonary arterial hypertension: Interim results of SOTERIA. European Respiratory Journal, 2025 July | URL: https://doi.org/10.1183/13993003.01435-2024 Phase 3 STELLAR study; Table 2. Change from Baseline at Week 24 in Primary and Secondary
Efficacy End Points (Intention-to-Treat Population); The Hodges–Lehmann (H-L) estimate of the difference between the sotatercept and placebo groups in the change from baseline at week 24 in NT-proBNP concentration was -441.6 pg/mL; Hoeper, M.
M., Badesch, D. B., Ghofrani, H. A., et al. (2023). Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. New England Journal of Medicine 2023 | URL: https://doi.org/10.1056/NEJMoa2213558 SOTERIA OLE study;
Supplementary Table 5. Change from Baseline at Week 24 and Year 1; Mean change from baseline defined as measurement at Visit 1 of SOTERIA or the last measure from the parent study before rollover in NT-proBNP; Interim results of SOTERIA;
Preston, I. R., Badesch, D. B., Ghofrani, H.A., Hoeper, M. M., Channick, R. N., Chin, K. M., Humbert, M., Jing, Z.C., Lang, I. M., McLaughlin, V. V., Simonneau, G., Souza, R., Tapson, V. F., Torres, F., White, R. J., Beaufils, B., Kim, J. B.,
& Rubin, L. J. (2025). A long-term follow-up study of sotatercept for treatment of pulmonary arterial hypertension: Interim results of SOTERIA. European Respiratory Journal, 2025 July | URL:
https://doi.org/10.1183/13993003.01435-2024 Phase 3 STELLAR study; Table 2. Change from Baseline at Week 24 in Primary and Secondary Efficacy End Points (Intention-to-Treat Population); Percentage of patients with improvement from baseline WHO
functional class 29.4% for sotatercept arm and 13.8% for placebo arm; Hoeper, M. M., Badesch, D. B., Ghofrani, H. A., et al. (2023). Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. New England Journal of Medicine
2023 | URL: https://doi.org/10.1056/NEJMoa2213558 SOTERIA OLE study; Supplementary Table 5. Percent of patients in the Continued Sotatercept and Placebo-Crossed groups that achieved WHO-FC II/I by Year 1; Interim results of SOTERIA; Preston,
I. R., Badesch, D. B., Ghofrani, H.-A., Hoeper, M. M., Channick, R. N., Chin, K. M., Humbert, M., Jing, Z.-C., Lang, I. M., McLaughlin, V. V., Simonneau, G., Souza, R., Tapson, V. F., Torres, F., White, R. J., Beaufils, B., Kim, J. B., &
Rubin, L. J. (2025). A long-term follow-up study of sotatercept for treatment of pulmonary arterial hypertension: Interim results of SOTERIA. European Respiratory Journal, 2025 July | URL: https://doi.org/10.1183/13993003.01435-2024 Footnotes
(3 of 3)
