.4
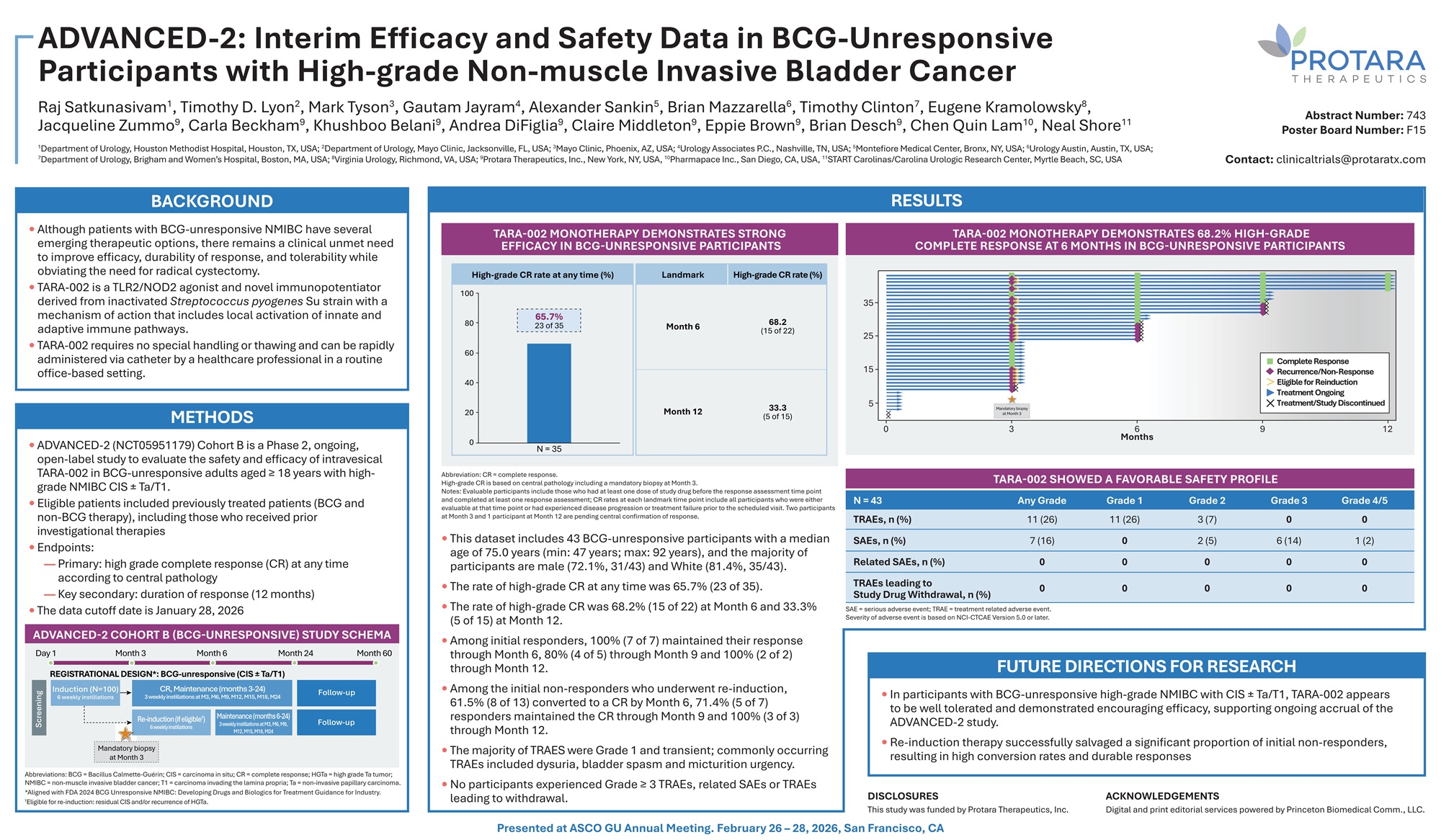
ADVANCED - 2: Interim Efficacy and Safety Data in BCG - Unresponsive Participants with High - grade Non - muscle Invasive Bladder Cancer Raj Satkunasivam 1 , Timothy D. Lyon 2 , Mark Tyson 3 , Gautam Jayram 4 , Alexander Sankin 5 , Brian Mazzarella 6 , Timothy Clinton 7 , Eugene Kramolowsky 8 , Jacqueline Zummo 9 , Carla Beckham 9 , Khushboo Belani 9 , Andrea DiFiglia 9 , Claire Middleton 9 , Eppie Brown 9 , Brian Desch 9 , Chen Ǫuin Lam 10 , Neal Shore 11 1 Department of Urology, Houston Methodist Hospital, Houston, TX, USA; 2 Department of Urology, Mayo Clinic, Jacksonville, FL, USA; 3 Mayo Clinic, Phoenix, AZ, USA; 4 Urology Associates P.C., Nashville, TN, USA; 5 Montefiore Medical Center, Bronx, NY, USA; 6 Urology Austin, Austin, TX, USA; 7 Department of Urology, Brigham and Women’s Hospital, Boston, MA, USA; 8 Virginia Urology, Richmond, VA, USA; 9 Protara Therapeutics, Inc., New York, NY, USA, 10 Pharmapace Inc., San Diego, CA, USA, 11 START Carolinas/Carolina Urologic Research Center, Myrtle Beach, SC, USA BACKGROUND • Although patients with BCG - unresponsive NMIBC have several emerging therapeutic options, there remains a clinical unmet need to improve efficacy, durability of response, and tolerability while obviating the need for radical cystectomy. • TARA - 002 is a TLR2/NOD2 agonist and novel immunopotentiator derived from inactivated Streptococcus pyogenes Su strain with a mechanism of action that includes local activation of innate and adaptive immune pathways. • TARA - 002 requires no special handling or thawing and can be rapidly administered via catheter by a healthcare professional in a routine office - based setting. METHODS • ADVANCED - 2 (NCT05951179) Cohort B is a Phase 2, ongoing, open - label study to evaluate the safety and efficacy of intravesical TARA - 002 in BCG - unresponsive adults aged ≥ 18 years with high - grade NMIBC CIS “ Ta/T1. • Eligible patients included previously treated patients (BCG and non - BCG therapy), including those who received prior investigational therapies • Endpoints: — Primary: high grade complete response (CR) at any time according to central pathology — Key secondary: duration of response (12 months) • The data cutoff date is January 28, 2026 ADVANCED - 2 COHORT B (BCG - UNRESPONSIVE) STUDY SCHEMA Abbreviations: BCG = Bacillus Calmette - Guérin; CIS = carcinoma in situ; CR = complete response; HGTa = high grade Ta tumor; NMIBC = non - muscle invasive bladder cancer; T1 = carcinoma invading the lamina propria; Ta = non - invasive papillary carcinoma. *Aligned with FDA 2024 BCG Unresponsive NMIBC: Developing Drugs and Biologics for Treatment Guidance for Industry. † Eligible for re - induction: residual CIS and/or recurrence of HGTa. RESULTS TARA - 002 MONOTHERAPY DEMONSTRATES STRONG EFFICACY IN BCG - UNRESPONSIVE PARTICIPANTS Abbreviation: CR = complete response. High - grade CR is based on central pathology including a mandatory biopsy at Month 3. Notes: Evaluable participants include those who had at least one dose of study drug before the response assessment time point and completed at least one response assessment; CR rates at each landmark time point include all participants who were either evaluable at that time point or had experienced disease progression or treatment failure prior to the scheduled visit. Two participants at Month 3 and 1 participant at Month 12 are pending central confirmation of response. • This dataset includes 43 BCG - unresponsive participants with a median age of 75.0 years (min: 47 years; max: 92 years), and the majority of participants are male (72.1%, 31/43) and White (81.4%, 35/43). • The rate of high - grade CR at any time was 65.7% (23 of 35). • The rate of high - grade CR was 68.2% (15 of 22) at Month 6 and 33.3% (5 of 15) at Month 12. • Among initial responders, 100% (7 of 7) maintained their response through Month 6, 80% (4 of 5) through Month 9 and 100% (2 of 2) through Month 12. • Among the initial non - responders who underwent re - induction, 61.5% (8 of 13) converted to a CR by Month 6, 71.4% (5 of 7) responders maintained the CR through Month 9 and 100% (3 of 3) through Month 12. • The majority of TRAES were Grade 1 and transient; commonly occurring TRAEs included dysuria, bladder spasm and micturition urgency. • No participants experienced Grade ≥ 3 TRAEs, related SAEs or TRAEs leading to withdrawal. FUTURE DIRECTIONS FOR RESEARCH • In participants w it h BCG - unresponsive high - grade NMIBC w it h CIS “ Ta/T 1 , TARA - 002 appears to be well tolerated and demonstrated encouraging efficacy, supporting ongoing accrual o f the ADVANCED - 2 study . • Re - induction therapy successfully salvaged a significant proportion o f initial non - responders, resulting in high conversion rates and durable responses TARA - 002 MONOTHERAPY DEMONSTRATES 68.2% HIGH - GRADE COMPLETE RESPONSE AT 6 MONTHS IN BCG - UNRESPONSIVE PARTICIPANTS TARA - 002 SHOWED A FAVORABLE SAFETY PROFILE Grade 4/5 Grade 3 Grade 2 Grade 1 Any Grade N = 43 0 0 3 (7) 11 (26) 11 (26) TRAEs, n (%) 1 (2) 6 (14) 2 (5) 0 7 (16) SAEs, n (%) 0 0 0 0 0 Related SAEs, n (%) 0 0 0 0 0 TRAEs leading to Study Drug Withdrawal, n (%) SAE = serious adverse event; TRAE = treatment related adverse event. Severity of adverse event is based on NCI - CTCAE Version 5.0 or later. Day 1 Month 3 Month 6 Month 24 Month 60 REGISTRATIONAL DESIGN*: BCG - unresponsive (CIS “ Ta/T1) Induction (N=100) 6 weekly instillations CR, Maintenance (months 3 - 24) 3 weekly instillations at M3, M6, M9, M12, M15, M18, M24 Follow - up Follow - up Re - induction (if eligible † ) 6 weekly instillations Maintenance (months 6 - 24) 3 weekly instillations at M3, M6, M9, M12, M15, M18, M24 Screenin g Mandatory biopsy at Month 3 0 3 6 Months 9 12 35 25 15 5 Complete Response Recurrence/Non - Response Eligible for Reinduction Treatment Ongoing Treatment/Study Discontinued Mandatory biopsy at Month 3 65.7% 23 of 35 Month 6 Month 12 68.2 (15 of 22) 33.3 (5 of 15) High - grade CR rate at any time (%) Landmark High - grade CR rate (%) 100 80 60 40 20 0 N = 35 Abstract Number: 743 Poster Board Number: F15 Contact: clinicaltrials@protaratx.com DISCLOSURES This study was funded by Protara Therapeutics, Inc. Presented at ASCO GU Annual Meeting. February 26 – 28, 2026, San Francisco, CA ACKNOWLEDGEMENTS Digital and print editorial services powered by Princeton Biomedical Comm., LLC.