.5
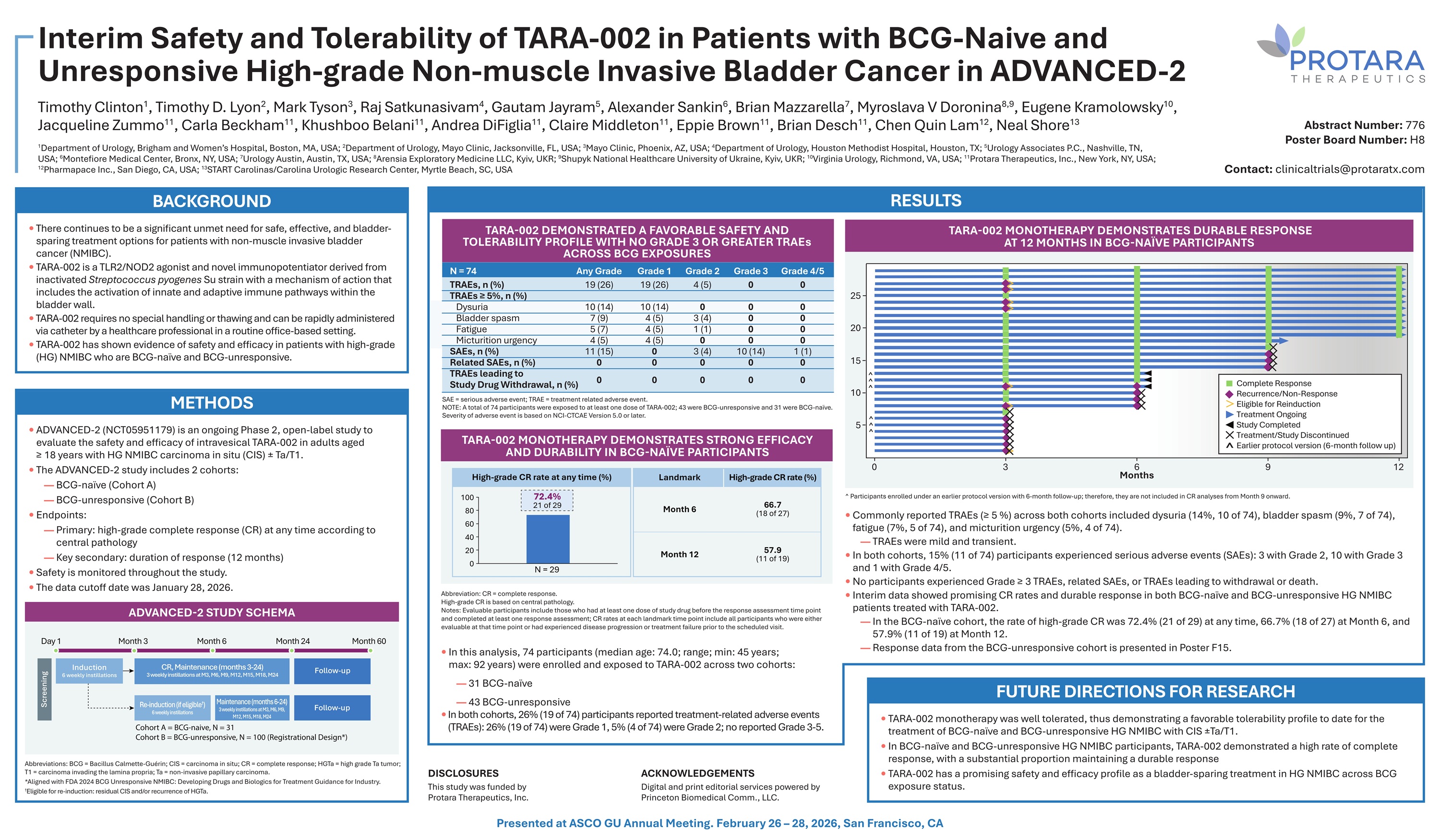
Interim Safety and Tolerability of TARA - 002 in Patients with BCG - Naive and Unresponsive High - grade Non - muscle Invasive Bladder Cancer in ADVANCED - 2 Timothy Clinton 1 , Timothy D. Lyon 2 , Mark Tyson 3 , Raj Satkunasivam 4 , Gautam Jayram 5 , Alexander Sankin 6 , Brian Mazzarella 7 , Myroslava V Doronina 8,9 , Eugene Kramolowsky 10 , Jacqueline Zummo 11 , Carla Beckham 11 , Khushboo Belani 11 , Andrea DiFiglia 11 , Claire Middleton 11 , Eppie Brown 11 , Brian Desch 11 , Chen Ǫuin Lam 12 , Neal Shore 13 1 Department of Urology, Brigham and Women’s Hospital, Boston, MA, USA; 2 Department of Urology, Mayo Clinic, Jacksonville, FL, USA; 3 Mayo Clinic, Phoenix, AZ, USA; 4 Department of Urology, Houston Methodist Hospital, Houston, TX; 5 Urology Associates P.C., Nashville, TN, USA; 6 Montefiore Medical Center, Bronx, NY, USA; 7 Urology Austin, Austin, TX, USA; 8 Arensia Exploratory Medicine LLC, Kyiv, UKR; 9 Shupyk National Healthcare University of Ukraine, Kyiv, UKR; 10 Virginia Urology, Richmond, VA, USA; 11 Protara Therapeutics, Inc., New York, NY, USA; 12 Pharmapace Inc., San Diego, CA, USA; 13 START Carolinas/Carolina Urologic Research Center, Myrtle Beach, SC, USA BACKGROUND • There continues to be a significant unmet need for safe, effective, and bladder - sparing treatment options for patients with non - muscle invasive bladder cancer (NMIBC). • TARA - 002 is a TLR2/NOD2 agonist and novel immunopotentiator derived from inactivated Streptococcus pyogenes Su strain with a mechanism of action that includes the activation of innate and adaptive immune pathways within the bladder wall. • TARA - 002 requires no special handling or thawing and can be rapidly administered via catheter by a healthcare professional in a routine office - based setting. • TARA - 002 has shown evidence of safety and efficacy in patients with high - grade (HG) NMIBC who are BCG - naïve and BCG - unresponsive. METHODS • ADVANCED - 2 (NCT05951179) is an ongoing Phase 2, open - label study to evaluate the safety and efficacy of intravesical TARA - 002 in adults aged ≥ 18 years with HG NMIBC carcinoma in situ (CIS) “ Ta/T1. • The ADVANCED - 2 study includes 2 cohorts: — BCG - naïve (Cohort A) — BCG - unresponsive (Cohort B) • Endpoints: — Primary: high - grade complete response (CR) at any time according to central pathology — Key secondary: duration of response (12 months) • Safety is monitored throughout the study. • The data cutoff date was January 28, 2026. Abbreviations: BCG = Bacillus Calmette - Guérin; CIS = carcinoma in situ; CR = complete response; HGTa = high grade Ta tumor; T1 = carcinoma invading the lamina propria; Ta = non - invasive papillary carcinoma. *Aligned with FDA 2024 BCG Unresponsive NMIBC: Developing Drugs and Biologics for Treatment Guidance for Industry. † Eligible for re - induction: residual CIS and/or recurrence of HGTa. ADVANCED - 2 STUDY SCHEMA Day 1 Month 3 Month 6 Month 24 RESULTS TARA - 002 DEMONSTRATED A FAVORABLE SAFETY AND TOLERABILITY PROFILE WITH NO GRADE 3 OR GREATER TRAEs ACROSS BCG EXPOSURES N = 74 Any Grade Grade 1 Grade 2 Grade 3 Grade 4/5 TRAEs, n (%) 19 (26) 19 (26) 4 (5) 0 0 TRAEs ≥ 5%, n (%) Dysuria 10 (14) 10 (14) 0 0 0 Bladder spasm 7 (9) 4 (5) 3 (4) 0 0 Fatigue Micturition urgency 5 (7) 4 (5) 4 (5) 4 (5) 1 (1) 0 0 0 0 0 1 (1) 10 (14) 3 (4) 0 11 (15) SAEs, n (%) 0 0 0 0 0 Related SAEs, n (%) TRAEs leading to Study Drug Withdrawal, n (%) 0 0 0 0 0 SAE = serious adverse event; TRAE = treatment related adverse event. NOTE: A total of 74 participants were exposed to at least one dose of TARA - 002; 43 were BCG - unresponsive and 31 were BCG - naïve. Severity of adverse event is based on NCI - CTCAE Version 5.0 or later. Abbreviation : CR = complete response . High - grade CR is based on central pathology . Notes : Evaluable participants include those who had at least one dose of study drug before the response assessment time point and completed at least one response assessment ; CR rates at each landmark time point include all participants who were either evaluable at that time point or had experienced disease progression or treatment failure prior to the scheduled visit . • In this analysis, 74 participants (median age: 74.0; range; min: 45 years; max: 92 years) were enrolled and exposed to TARA - 002 across two cohorts: — 31 BCG - naïve — 43 BCG - unresponsive • In both cohorts, 26% (19 of 74) participants reported treatment - related adverse events (TRAEs): 26% (19 of 74) were Grade 1, 5% (4 of 74) were Grade 2; no reported Grade 3 - 5. FUTURE DIRECTIONS FOR RESEARCH • TARA - 002 monotherapy was well tolerated, thus demonstrating a favorable tolerability profile to date for the treatment of BCG - naïve and BCG - unresponsive HG NMIBC with CIS “ Ta/T1. • In BCG - naïve and BCG - unresponsive HG NMIBC participants, TARA - 002 demonstrated a high rate of complete response, with a substantial proportion maintaining a durable response • TARA - 002 has a promising safety and efficacy profile as a bladder - sparing treatment in HG NMIBC across BCG exposure status. TARA - 002 MONOTHERAPY DEMONSTRATES DURABLE RESPONSE AT 12 MONTHS IN BCG - NAÏVE PARTICIPANTS ^ Participants enrolled under an earlier protocol version with 6 - month follow - up; therefore, they are not included in CR analyses from Month 9 onward. • Commonly reported TRAEs (≥ 5 %) across both cohorts included dysuria (14%, 10 of 74), bladder spasm (9%, 7 of 74), fatigue (7%, 5 of 74), and micturition urgency (5%, 4 of 74). — TRAEs were mild and transient. • In both cohorts, 15% (11 of 74) participants experienced serious adverse events (SAEs): 3 with Grade 2, 10 with Grade 3 and 1 with Grade 4/5. • No participants experienced Grade ≥ 3 TRAEs, related SAEs, or TRAEs leading to withdrawal or death. • Interim data showed promising CR rates and durable response in both BCG - naïve and BCG - unresponsive HG NMIBC patients treated with TARA - 002. — In the BCG - naïve cohort, the rate of high - grade CR was 72.4% (21 of 29) at any time, 66.7% (18 of 27) at Month 6, and 57.9% (11 of 19) at Month 12. — Response data from the BCG - unresponsive cohort is presented in Poster F15. Month 60 Induction 6 weekly instillations CR, Maintenance (months 3 - 24) 3 weekly instillations at M3, M6, M9, M12, M15, M18, M24 Follow - up Follow - up Re - induction (if eligible † ) 6 weekly instillations Maintenance (months 6 - 24) 3 weekly instillations at M3, M6, M9, M12, M15, M18, M24 Screening Cohort A = BCG - naive, N = 31 Cohort B = BCG - unresponsive, N = 100 (Registrational Design*) 0 3 6 Months 9 12 25 20 15 5 Complete Response Recurrence/Non - Response Eligible for Reinduction Treatment Ongoing Study Completed Treatment/Study Discontinued Earlier protocol version (6 - month follow up) ^ 10 ^ ^ ^ ^ 72.4% 21 of 29 Month 6 Month 12 TARA - 002 MONOTHERAPY DEMONSTRATES STRONG EFFICACY AND DURABILITY IN BCG - NAÏVE PARTICIPANTS High - grade CR rate at any time (%) Landmark High - grade CR rate (%) 66.7 (18 of 27) 57.9 (11 of 19) 100 80 60 40 20 0 N = 29 Abstract Number: 776 Poster Board Number: H8 Contact: clinicaltrials@protaratx.com DISCLOSURES This study was funded by Protara Therapeutics, Inc. ACKNOWLEDGEMENTS Digital and print editorial services powered by Princeton Biomedical Comm., LLC. Presented at ASCO GU Annual Meeting. February 26 – 28, 2026, San Francisco, CA