| Delivering Novel Therapies for RAS/MAPK Pathway-Driven Cancers C O R P O R A T E P R E S E N T A T I O N M A Y 2 0 2 6 |
| 2 FORWARD-LOOKING STATEMENTS This presentation includes forward-looking statements about, among other things, Verastem Oncology’s (the “Company”) programs and product candidates, strategy, future plans and prospects, including statements related to the approval and commercialization of AVMAPKI® FAKZYNJA® CO-PACK (avutometinib capsules; defactinib tablets) as a treatment for adult patients with Kirsten rat sarcoma viral oncogene homolog (KRAS) mutant-type (mt) recurrent Low-Grade Serous Ovarian Cancer (LGSOC), the expected outcome and benefits of collaborations, including with GenFleet Therapeutics (Shanghai), Inc. (GenFleet), including the conduct of a Phase 1/2a study and subsequent studies with respect to VS-7375, the potential of the results of the RAMP 301 Phase 3 trial to confirm the results of the RAMP 201 study specific to KRAS mutant patients and to expand the indication for AVMAPKI FAKZYNJA CO-PACK regardless of KRAS mutation status, the structure and potential clinical value of our completed, planned and pending clinical trials, the potential clinical value of various of the Company's clinical trials, including the RAMP 201, RAMP 201J, RAMP 205, RAMP 301 and VS-7375 trials, the timing of commencing and completing trials, including topline data reports, our interactions with regulators, the timeline and indications for clinical development, regulatory submissions and the potential for and timing of commercialization of our product candidates and potential for additional development programs involving the Company’s lead compound and the potential market opportunities thereof; and the estimated addressable markets for, and anticipated market opportunities of our drug candidates. The words "anticipate," "believe," "estimate," "expect," "may," "plan," "target," "potential," "would," "could," "should," "continue," “can” and similar expressions are intended to identify forward-looking statements, although not all forward-looking statements contain these identifying words. Each forward-looking statement is subject to risks and uncertainties that could cause actual results to differ materially from those expressed or implied in such statement. Forward-looking statements are subject to a number of risks and uncertainties including, but not limited to: the assumptions underlying the forward-looking statements; risks related to the development and successful commercialization of our product candidates; obtaining and maintaining regulatory approvals, including, but not limited to, potential regulatory delays or rejections; the challenges with the commercialization of a new product; our history of operating losses and the possibility that we may never achieve or maintain profitability; risks associated with meeting the objectives of Verastem's clinical trials, including, but not limited to Verastem's ability to achieve enrollment objectives concerning patient numbers (including an adequate safety database), outcomes objectives and/or timing objectives for Verastem's trials; any delays or failures enrollment and the occurrence of adverse safety events; our ability to successfully commercialize AVMAPKI FAKZYNJA CO-PACK in the U.S. including our ability to generate market demand for and acceptance of AVMAPKI FAKZYNJA CO-PACK; the potential inability to raise sufficient capital to fund ongoing operations as currently planned or to obtain financing on acceptable terms or to fund operations from revenues generated by the sales of AVMAPKI FAKZYNJA CO-PACK; actions or advice of regulatory agencies to maintain regulatory approval of AVMAPKI FAKZYNJA CO-PACK; the impact of current and future healthcare reforms, including those affecting the delivery of or payment for healthcare products and services; uncertainties related to the activities and initiatives of the current U.S. presidential administration, including regulatory and policy changes that may adversely affect our business; risks related to our ability to obtain, maintain and enforce patent and other intellectual property protection for our product candidates; decisions by regulatory authorities regarding trial design, labeling and other matters that could affect the timing, availability or commercial potential of our product candidates; whether preclinical testing of our product candidates and preliminary or interim data from clinical trials will be predictive of the results or success of ongoing or later clinical trials; that the timing, scope and rate of reimbursement for our product candidates is uncertain; that the market opportunities of our drug candidates are based on internal and third-party estimates which may prove to be incorrect; that third-party payors (including government agencies) may not reimburse; that there may be competitive developments affecting our product candidates; that data may not be available when expected; that enrollment of clinical trials may take longer than expected; the risks that we will not satisfy our post-marketing requirements and commitments established and agreed to as part of the FDA's approval of AVMAPKI FAKZYNJA CO-PACK; that our marketed product candidates may cause adverse safety events and/or unexpected concerns may arise from additional data or analysis, or result in unmanageable safety profiles as compared to their levels of efficacy; that we may not be able to confirm the results from the RAMP 201 study or expand the approved indication for AVMAPKI FAKZYNJA CO-PACK; that our product candidates may experience manufacturing or supply interruptions or failures; that any of our third-party contract research organizations, contract manufacturing organizations, clinical sites, or contractors, among others, who we rely on may fail to fully perform; that we face substantial competition, which may result in others developing or commercializing products before or more successfully than we do which could result in reduced market share or market potential for our product candidates; that we may be unable to successfully initiate or complete the clinical development and eventual commercialization of our product candidates; that the development and commercialization of our product candidates may take longer or cost more than planned, including as a result of conducting additional studies or our decisions regarding execution of such commercialization; that we may not attract and retain high quality personnel; that we or Pfizer, Inc. may fail to fully perform under the license agreement covering certain Pfizer FAK inhibitors, including defactinib; that we or Chugai Pharmaceutical Co., Ltd. may fail to fully perform under the avutometinib license agreement; that we or GenFleet may fail to fully perform under the collaboration and option agreement covering VS-7375 and other assets we may decide to option in; that our total addressable and target markets for our product candidates might be smaller than we are presently estimating; that we or Secura Bio, Inc. may fail to fully perform under the asset purchase agreement with Secura Bio, Inc., including in relation to milestone payments; that we may not be able to establish new or expand on existing collaborations or partnerships, including with respect to in-licensing of our product candidates, on favorable terms, or at all; that we may be unable to obtain adequate financing in the future through product licensing, co-promotional arrangements, public or private equity, debt financing or otherwise; that we may not pursue or submit regulatory filings for our product candidates; that, due to the current presidential administration's significant reduction in the FDA's workforce and potential reductions to the FDA's budget, we may experience a material impact to the FDA's ability to engage in a variety of activities that may affect our business, including routine regulatory and oversight activities; and that our product candidates may not receive regulatory approval, become commercially successful products, or result in new treatment options being offered to patients. Other risks and uncertainties include those identified under the heading “Risk Factors” in the Company’s Annual Report on Form 10-K for the year ended December 31, 2025, as filed with the Securities and Exchange Commission (SEC) on March 04, 2026, and in any subsequent filings with the SEC, which are available at www.sec.govand www.verastem.com.The forward-looking statements in this presentation speak only as of the original date of this presentation, and we undertake no obligation to update or revise any of these statements whether as a result of new information, future events or otherwise, except as required by law. Our business is subject to substantial risks and uncertainties, including those referenced above. Investors, potential investors, and others should give careful consideration to these risks and uncertainties. USE OF NON-GAAP FINANCIAL MEASURES This presentation contains references to our non-GAAP operating expense, a financial measure that is not calculated in accordance with generally accepted accounting principles in the US (GAAP). This non-GAAP financial measure excludes certain amounts or expenses from the corresponding financial measures determined in accordance with GAAP. Management believes this non-GAAP information is useful for investors, taken in conjunction with the Company’s GAAP financial statements, because it provides greater transparency and period-over-period comparability with respect to the Company’s operating performance and can enhance investors’ ability to identify operating trends in the Company’s business. Management uses this measure, among other factors, to assess and analyze operational results and trends and to make financial and operational decisions. Non-GAAP information is not prepared under a comprehensive set of accounting rules and should only be used to supplement an understanding of the Company’s operating results as reported under GAAP, not in isolation or as a substitute for, or superior to, financial information prepared and presented in accordance with GAAP. In addition, this non-GAAP financial measure is unlikely to be comparable with non-GAAP information provided by other companies. The determination of the amounts that are excluded from non-GAAP financial measures is a matter of management judgment and depends upon, among other factors, the nature of the underlying expense or income amounts. Reconciliations between this non-GAAP financial measure and the most comparable GAAP financial measure are included in the footnotes to the slides in this presentation on which such non-GAAP number appears. THIRD-PARTY SOURCES Certain information contained in this presentation, including industry and market data and other statistical information, relates to or is based on studies, publications, surveys and other data obtained from third-party sources and the Company’s own internal estimates and research. While the Company believes these third-party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Disclaimers |
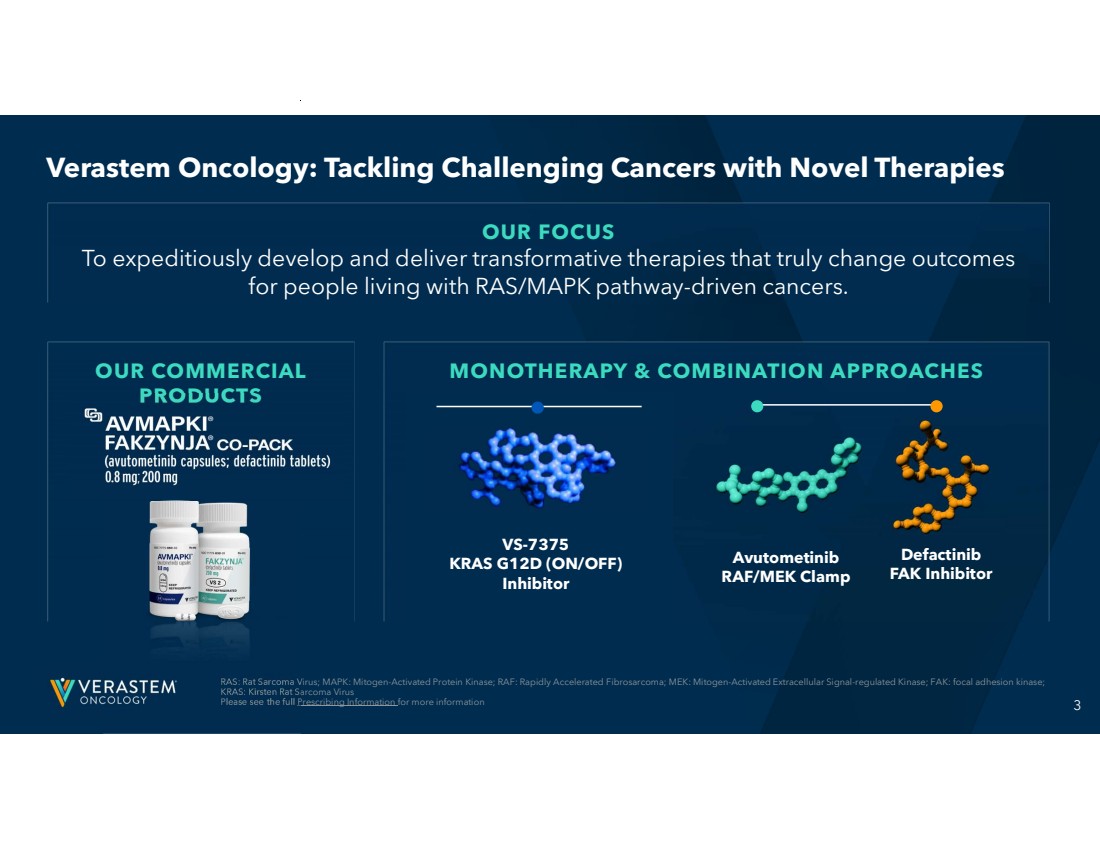
| 3 OUR COMMERCIAL PRODUCTS MONOTHERAPY & COMBINATION APPROACHES RAS: Rat Sarcoma Virus; MAPK: Mitogen-Activated Protein Kinase; RAF: Rapidly Accelerated Fibrosarcoma; MEK: Mitogen-Activated Extracellular Signal-regulated Kinase; FAK: focal adhesion kinase; KRAS: Kirsten Rat Sarcoma Virus Please see the full Prescribing Information for more information OUR FOCUS To expeditiously develop and deliver transformative therapies that truly change outcomes for people living with RAS/MAPK pathway-driven cancers. Avutometinib RAF/MEK Clamp Defactinib FAK Inhibitor VS-7375 KRAS G12D (ON/OFF) Inhibitor Verastem Oncology: Tackling Challenging Cancers with Novel Therapies |
| 4 FDA: Food and Drug Administration CLINICAL-TO-COMMERCIAL SUCCESS in bringing novel RAS/MAPK pathway-targeted therapies from development to FDA approval to commercialization INNOVATIVE PIPELINE with a potential best-in-class KRAS G12D asset targeting the most prevalent KRAS mutation in human cancers SCALABLE ORGANIZATION to maximize future oncology development programs and launches Well Positioned to Deliver Continued Commercial Success and a Potential Best-in-Class Treatment for Long-term Growth OUR ADVANTAGE: 4 |

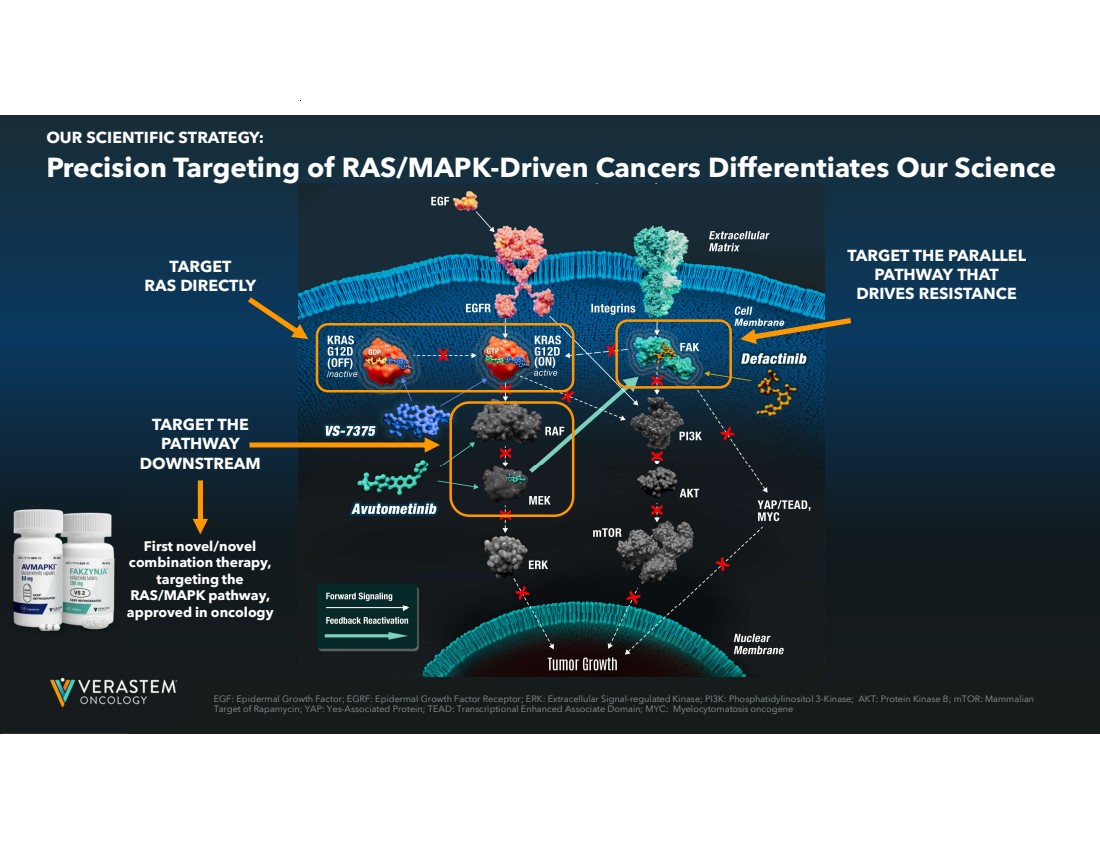
| 5 TARGET RAS DIRECTLY TARGET THE PATHWAY DOWNSTREAM TARGET THE PARALLEL PATHWAY THAT DRIVES RESISTANCE First novel/novel combination therapy, targeting the RAS/MAPK pathway, approved in oncology Precision Targeting of RAS/MAPK-Driven Cancers Differentiates Our Science OUR SCIENTIFIC STRATEGY: EGF: Epidermal Growth Factor; EGRF: Epidermal Growth Factor Receptor; ERK: Extracellular Signal-regulated Kinase; PI3K: Phosphatidylinositol 3-Kinase; AKT: Protein Kinase B; mTOR: Mammalian Target of Rapamycin; YAP: Yes-Associated Protein; TEAD: Transcriptional Enhanced Associate Domain; MYC: Myelocytomatosis oncogene |
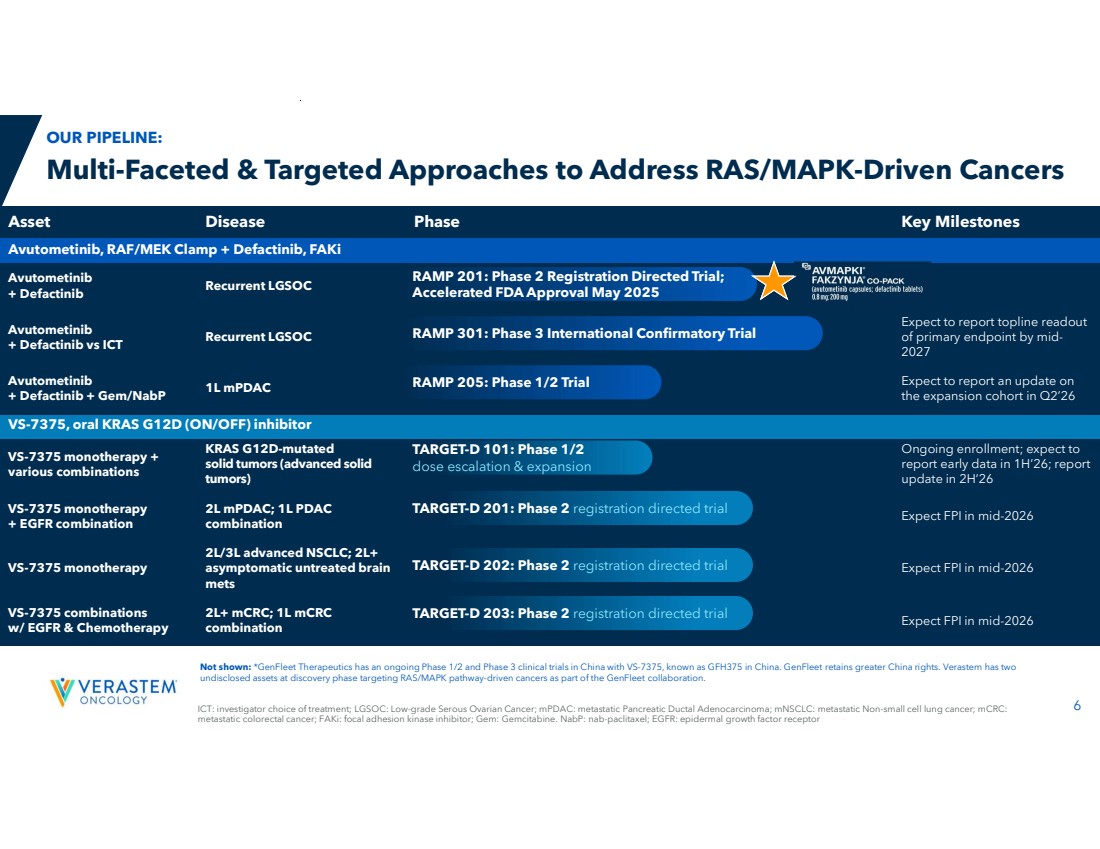
| ICT: investigator choice of treatment; LGSOC: Low-grade Serous Ovarian Cancer; mPDAC: metastatic Pancreatic Ductal Adenocarcinoma; mNSCLC: metastatic Non-small cell lung cancer; mCRC: 6 metastatic colorectal cancer; FAKi: focal adhesion kinase inhibitor; Gem: Gemcitabine. NabP: nab-paclitaxel; EGFR: epidermal growth factor receptor Not shown: *GenFleet Therapeutics has an ongoing Phase 1/2 and Phase 3 clinical trials in China with VS-7375, known as GFH375 in China. GenFleet retains greater China rights. Verastem has two undisclosed assets at discovery phase targeting RAS/MAPK pathway-driven cancers as part of the GenFleet collaboration. Asset Disease Phase Key Milestones Avutometinib, RAF/MEK Clamp + Defactinib, FAKi Recurrent LGSOC Avutometinib + Defactinib Expect to report topline readout of primary endpoint by mid-2027 Recurrent LGSOC Avutometinib + Defactinib vs ICT Expect to report an update on the expansion cohort in Q2’26 1L mPDAC Avutometinib + Defactinib + Gem/NabP VS-7375, oral KRAS G12D (ON/OFF) inhibitor Ongoing enrollment; expect to report early data in 1H’26; report update in 2H’26 KRAS G12D-mutated solid tumors (advanced solid tumors) VS-7375 monotherapy + various combinations Expect FPI in mid-2026 2L mPDAC; 1L PDAC combination VS-7375 monotherapy + EGFR combination Expect FPI in mid-2026 2L/3L advanced NSCLC; 2L+ asymptomatic untreated brain mets VS-7375 monotherapy Expect FPI in mid-2026 2L+ mCRC; 1L mCRC combination VS-7375 combinations w/ EGFR & Chemotherapy TARGET-D 101: Phase 1/2 dose escalation & expansion TARGET-D 202: Phase 2 registration directed trial TARGET-D 203: Phase 2 registration directed trial TARGET-D 201: Phase 2 registration directed trial RAMP 201: Phase 2 Registration Directed Trial; Accelerated FDA Approval May 2025 RAMP 301: Phase 3 International Confirmatory Trial RAMP 205: Phase 1/2 Trial Multi-Faceted & Targeted Approaches to Address RAS/MAPK-Driven Cancers OUR PIPELINE: |
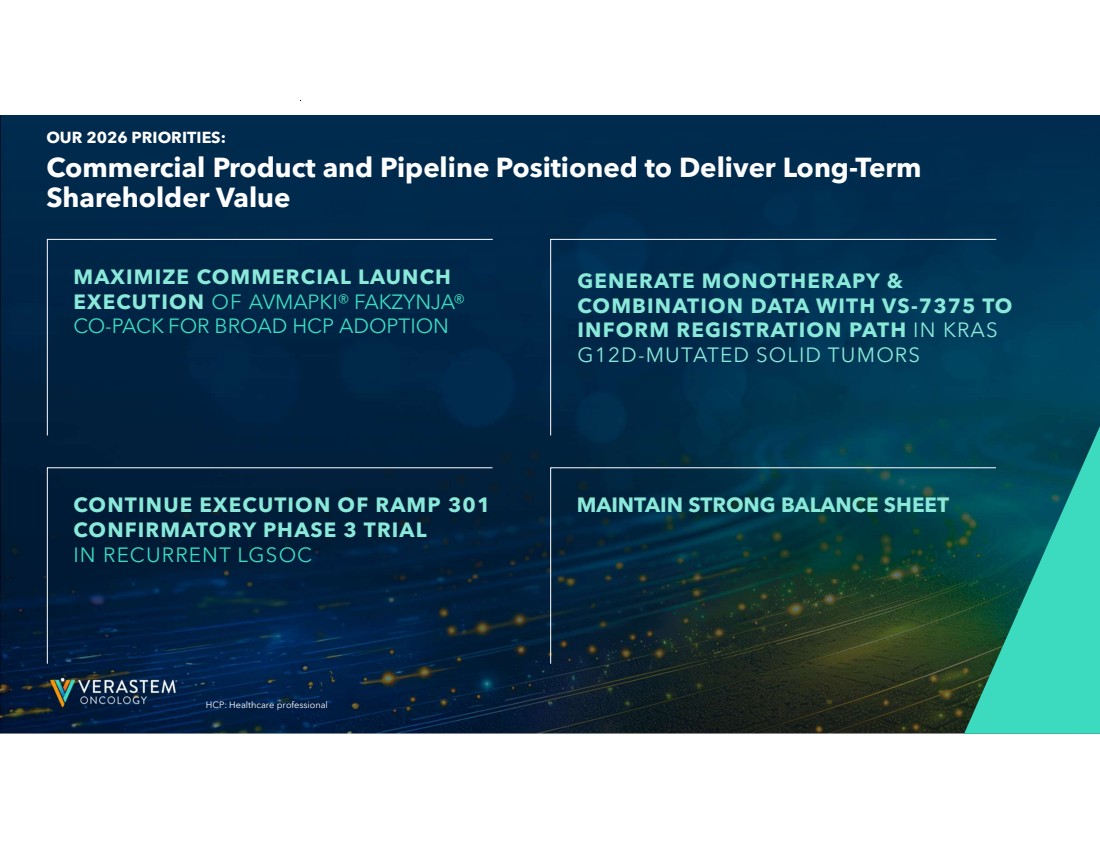
| 7 MAXIMIZE COMMERCIAL LAUNCH EXECUTION OF AVMAPKI® FAKZYNJA® CO-PACK FOR BROAD HCP ADOPTION Commercial Product and Pipeline Positioned to Deliver Long-Term Shareholder Value OUR 2026 PRIORITIES: CONTINUE EXECUTION OF RAMP 301 CONFIRMATORY PHASE 3 TRIAL IN RECURRENT LGSOC MAINTAIN STRONG BALANCE SHEET HCP: Healthcare professional GENERATE MONOTHERAPY & COMBINATION DATA WITH VS-7375 TO INFORM REGISTRATION PATH IN KRAS G12D-MUTATED SOLID TUMORS |
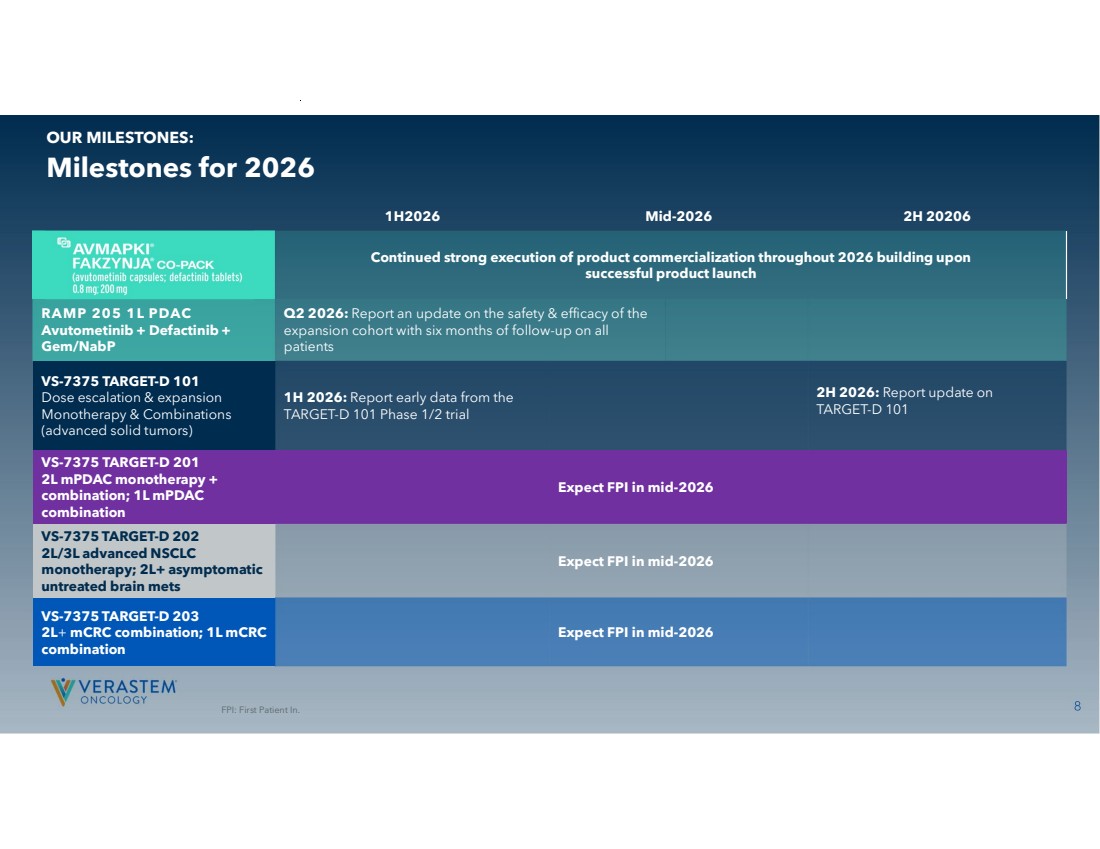
| 8 1H2026 Mid-2026 2H 20206 Continued strong execution of product commercialization throughout 2026 building upon successful product launch Q2 2026: Report an update on the safety & efficacy of the expansion cohort with six months of follow-up on all patients RAMP 205 1L PDAC Avutometinib + Defactinib + Gem/NabP 2H 2026: Report update on TARGET-D 101 1H 2026: Report early data from the TARGET-D 101 Phase 1/2 trial VS-7375 TARGET-D 101 Dose escalation & expansion Monotherapy & Combinations (advanced solid tumors) Expect FPI in mid-2026 VS-7375 TARGET-D 201 2L mPDAC monotherapy + combination; 1L mPDAC combination Expect FPI in mid-2026 VS-7375 TARGET-D 202 2L/3L advanced NSCLC monotherapy; 2L+ asymptomatic untreated brain mets Expect FPI in mid-2026 VS-7375 TARGET-D 203 2L+ mCRC combination; 1L mCRC combination Milestones for 2026 OUR MILESTONES: FPI: First Patient In. |
| 9 Commercially Launched in the U.S. for KRAS-mutated Recurrent LGSOC FDA APPROVAL DATE: MAY 8, 2025 |

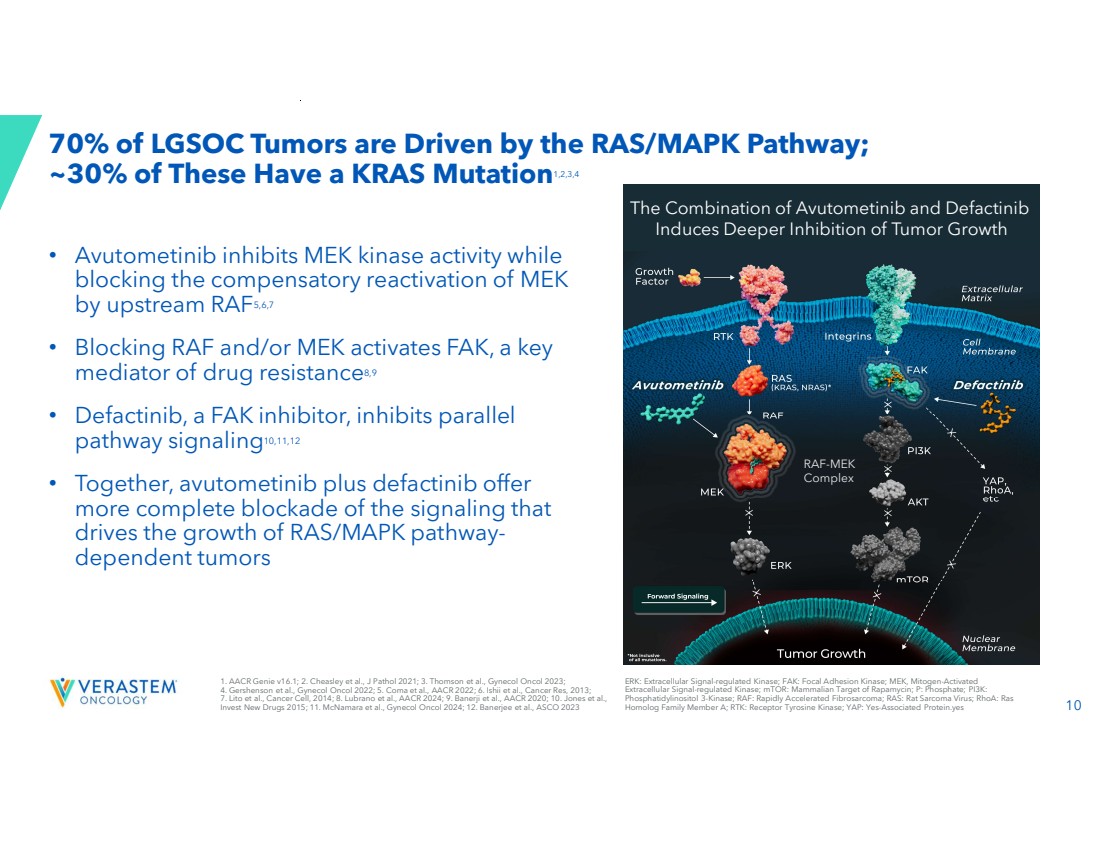
| 10 70% of LGSOC Tumors are Driven by the RAS/MAPK Pathway; ~30% of These Have a KRAS Mutation1,2,3,4 • Avutometinib inhibits MEK kinase activity while blocking the compensatory reactivation of MEK by upstream RAF5,6,7 • Blocking RAF and/or MEK activates FAK, a key mediator of drug resistance8,9 • Defactinib, a FAK inhibitor, inhibits parallel pathway signaling10,11,12 • Together, avutometinib plus defactinib offer more complete blockade of the signaling that drives the growth of RAS/MAPK pathway-dependent tumors RAF-MEK Complex The Combination of Avutometinib and Defactinib Induces Deeper Inhibition of Tumor Growth 1. AACR Genie v16.1; 2. Cheasley et al., J Pathol 2021; 3. Thomson et al., Gynecol Oncol 2023; 4. Gershenson et al., Gynecol Oncol 2022; 5. Coma et al., AACR 2022; 6. Ishii et al., Cancer Res, 2013; 7. Lito et al., Cancer Cell, 2014; 8. Lubrano et al., AACR 2024; 9. Banerji et al., AACR 2020; 10. Jones et al., Invest New Drugs 2015; 11. McNamara et al., Gynecol Oncol 2024; 12. Banerjee et al., ASCO 2023 ERK: Extracellular Signal-regulated Kinase; FAK: Focal Adhesion Kinase; MEK, Mitogen-Activated Extracellular Signal-regulated Kinase; mTOR: Mammalian Target of Rapamycin; P: Phosphate; PI3K: Phosphatidylinositol 3-Kinase; RAF: Rapidly Accelerated Fibrosarcoma; RAS: Rat Sarcoma Virus; RhoA: Ras Homolog Family Member A; RTK: Receptor Tyrosine Kinase; YAP: Yes-Associated Protein.yes |
| 11 High Unmet Need for an Effective and Tolerable Therapy in Recurrent LGSOC • U.S. annual incidence: ~1,000-2,0001 and prevalence: 6,000-8,0002 • Affects younger women with bimodal peaks of diagnosis between the ages of 20-30 and 50-60 – Disproportionately impacts health, fertility, and long-term quality of life3,4 • 80-90% of patients will experience a recurrence5 • Standard of care offers low to moderate response rates (6-13%)6,7,8 When you get told that you have a recurrence, the mental load is a lot. You’re thinking, okay, what did I have to do for treatment the first time? Now I have to repeat that. And will there even be something available for me to take for a second, or a third recurrence? - Amanda, real patient living with recurrent LGSOC; diagnosed at 26 with LGSOC 1.Verastem DOF; 2. US Cancer Statistics. Accessed 2024; 3. Slomovitz Gynecol Oncol 2020; 4. Manning-Geist B et al. Clin Cancer Res 2022;28(20):4456-4465; 5. Babaier 2022/p1/para1/ln6,7; 6. Gershenson Gynecol Oncol 2022; 7. Slomovitz Gynecol Oncol 2020; 8. Monk 2020/p3758/table2/footnote-b; 11 |
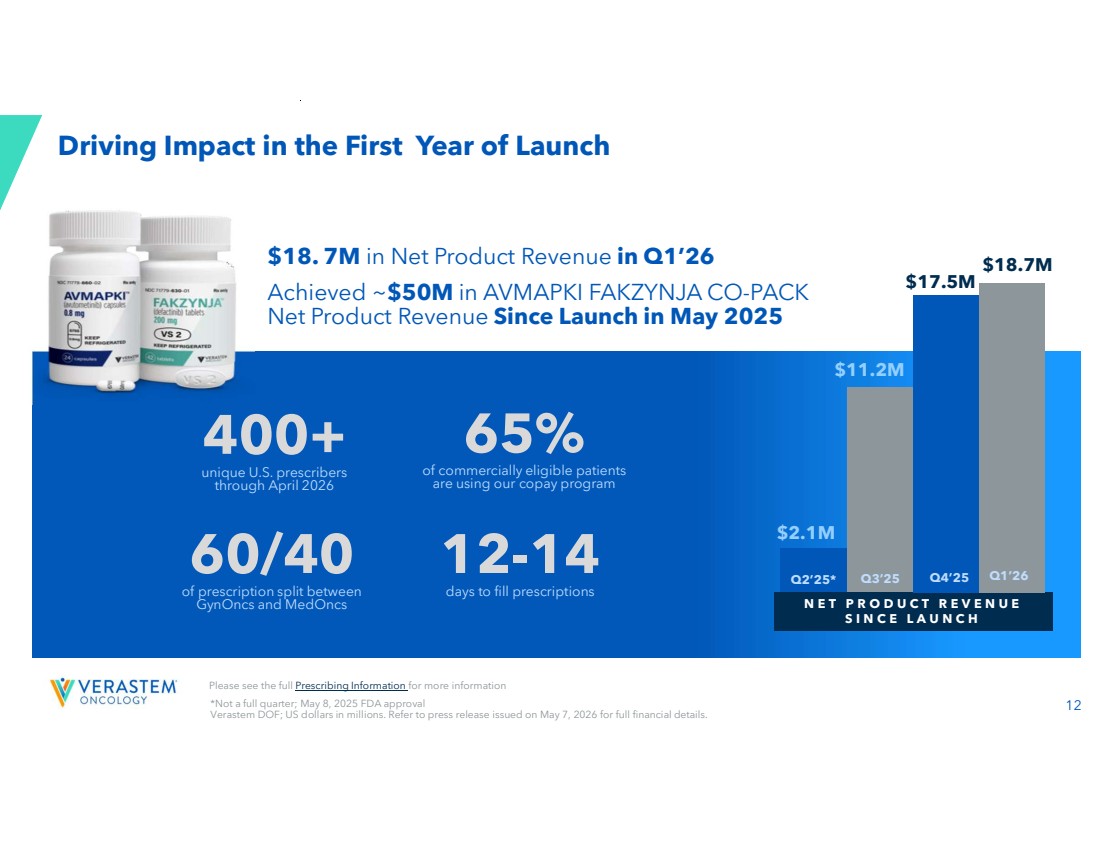
| 12 Driving Impact in the First Year of Launch N E T P R O D U C T R E V E N U E S I N C E L A U N C H $11.2M $17.5M $2.1M $30.9M FY25 $18.7M Q2’25* Q3’25 Q4’25 Q1’26 400+ unique U.S. prescribers through April 2026 60/40 of prescription split between GynOncs and MedOncs 65% of commercially eligible patients are using our copay program 12-14 days to fill prescriptions $18. 7M in Net Product Revenue in Q1’26 Achieved ~$50M in AVMAPKI FAKZYNJA CO-PACK Net Product Revenue Since Launch in May 2025 *Not a full quarter; May 8, 2025 FDA approval Verastem DOF; US dollars in millions. Refer to press release issued on May 7, 2026 for full financial details. Please see the full Prescribing Information for more information |
| 13 Three Key Drivers to Realize Full Benefits of AVMAPKI FAKZYNJA CO-PACK v New Patients Starts Use at First Recurrence Help Patients Stay on Therapy Please see the full Prescribing Information for more information |
| 14 Reach among prescribers who haven’t prescribed AVMAPKI FAKZYNJA CO-PACK Experience with AVMAPKI FAKZYNJA CO-PACK among current prescribers Entrenched prescribing behaviors Maximizing Benefit with AVMAPKI FAKZYNJA CO-PACK at First Recurrence Expand Shift Deepen Substantial Market Opportunity, Growth Potential Ahead Please see the full Prescribing Information for more information |

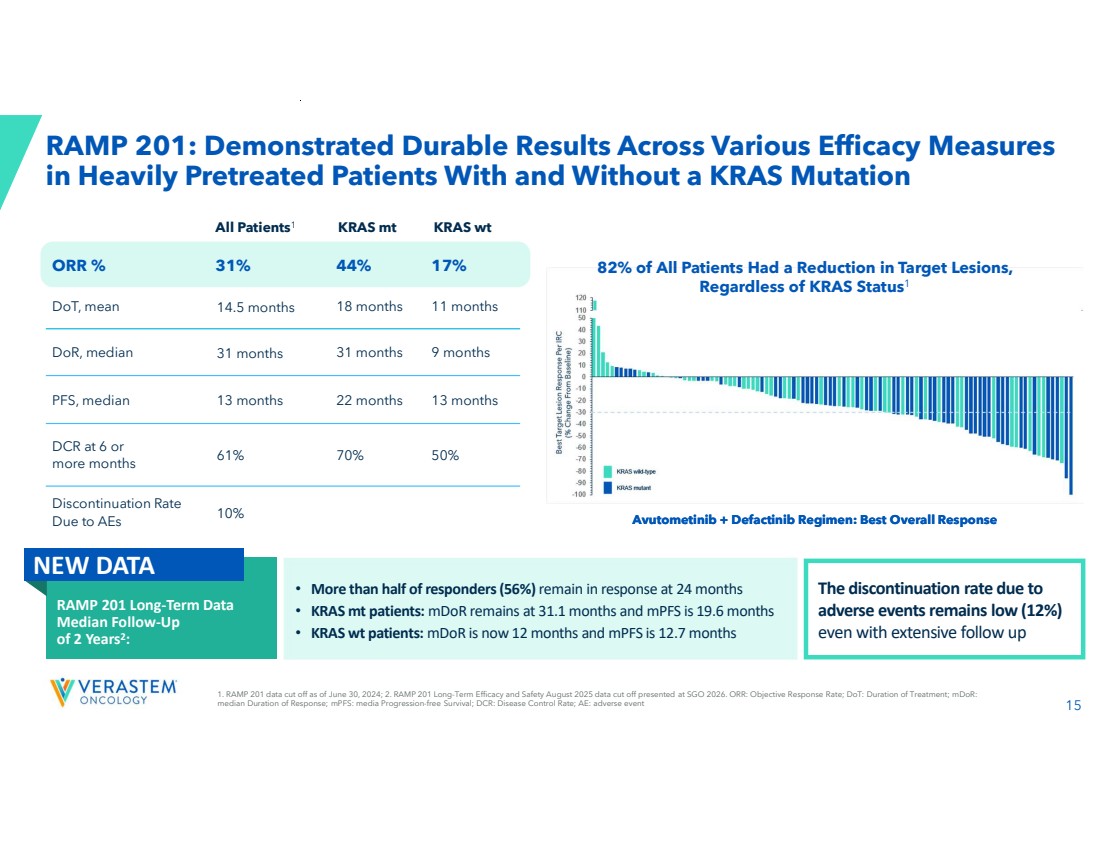
| 15 RAMP 201: Demonstrated Durable Results Across Various Efficacy Measures in Heavily Pretreated Patients With and Without a KRAS Mutation Avutometinib + Defactinib Regimen: Best Overall Response 82% of All Patients Had a Reduction in Target Lesions, Regardless of KRAS Status1 All Patients KRAS mt KRAS wt 1 ORR % 31% 44% 17% DoT, mean 14.5 months 18 months 11 months DoR, median 31 months 31 months 9 months PFS, median 13 months 22 months 13 months 61% 70% 50% DCR at 6 or more months 10% Discontinuation Rate Due to AEs 1. RAMP 201 data cut off as of June 30, 2024; 2. RAMP 201 Long-Term Efficacy and Safety August 2025 data cut off presented at SGO 2026. ORR: Objective Response Rate; DoT: Duration of Treatment; mDoR: median Duration of Response; mPFS: media Progression-free Survival; DCR: Disease Control Rate; AE: adverse event Avutometinib + Defactinib Regimen: Best Overall Response • More than half of responders (56%) remain in response at 24 months • KRAS mt patients: mDoR remains at 31.1 months and mPFS is 19.6 months • KRAS wt patients: mDoR is now 12 months and mPFS is 12.7 months The discontinuation rate due to adverse events remains low (12%) even with extensive follow up RAMP 201 Long-Term Data Median Follow-Up of 2 Years2 : NEW DATA |
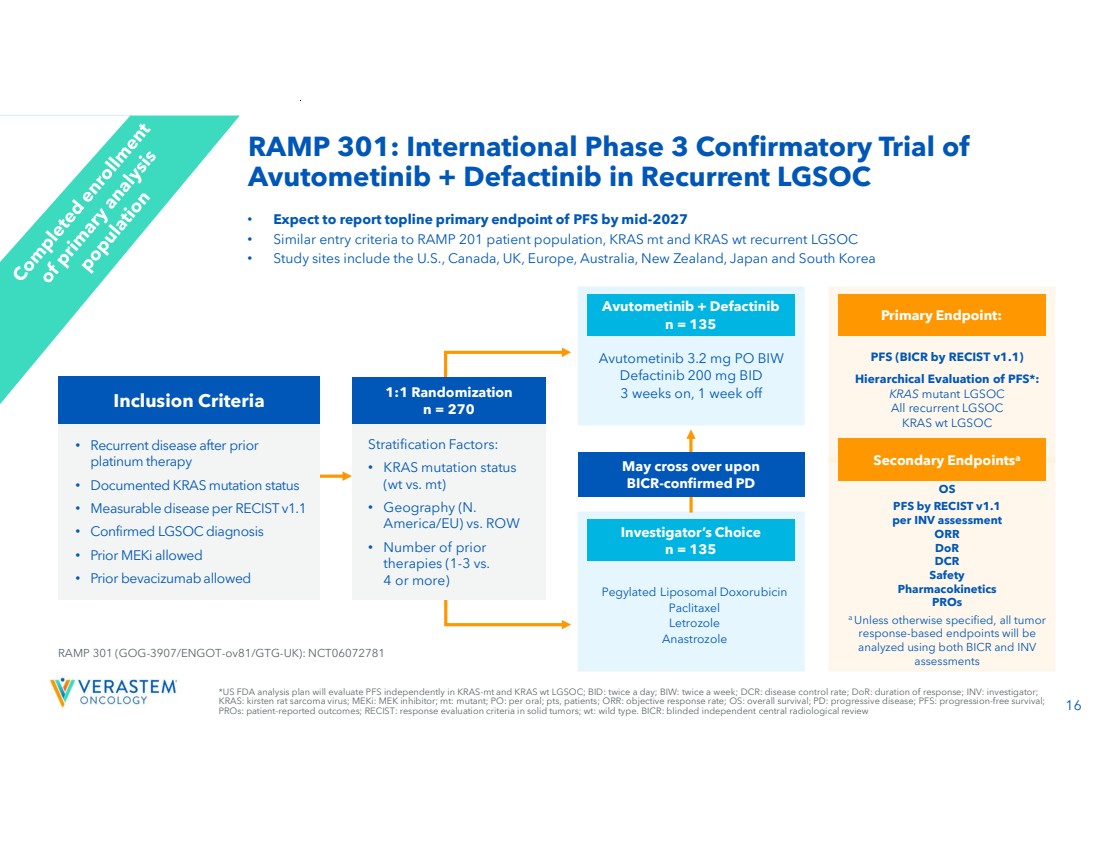
| 16 OS PFS by RECIST v1.1 per INV assessment ORR DoR DCR Safety Pharmacokinetics PROs a Unless otherwise specified, all tumor response-based endpoints will be analyzed using both BICR and INV assessments *US FDA analysis plan will evaluate PFS independently in KRAS-mt and KRAS wt LGSOC; BID: twice a day; BIW: twice a week; DCR: disease control rate; DoR: duration of response; INV: investigator; KRAS: kirsten rat sarcoma virus; MEKi: MEK inhibitor; mt: mutant; PO: per oral; pts, patients; ORR: objective response rate; OS: overall survival; PD: progressive disease; PFS: progression-free survival; PROs: patient-reported outcomes; RECIST: response evaluation criteria in solid tumors; wt: wild type. BICR: blinded independent central radiological review • Expect to report topline primary endpoint of PFS by mid-2027 • Similar entry criteria to RAMP 201 patient population, KRAS mt and KRAS wt recurrent LGSOC • Study sites include the U.S., Canada, UK, Europe, Australia, New Zealand, Japan and South Korea • Recurrent disease after prior platinum therapy • Documented KRAS mutation status • Measurable disease per RECIST v1.1 • Confirmed LGSOC diagnosis • Prior MEKi allowed • Prior bevacizumab allowed RAMP 301 (GOG-3907/ENGOT-ov81/GTG-UK): NCT06072781 Pegylated Liposomal Doxorubicin Paclitaxel Letrozole Anastrozole Investigator’s Choice n = 135 Avutometinib 3.2 mg PO BIW Defactinib 200 mg BID 3 weeks on, 1 week off Avutometinib + Defactinib n = 135 May cross over upon BICR-confirmed PD PFS (BICR by RECIST v1.1) Hierarchical Evaluation of PFS*: KRAS mutant LGSOC All recurrent LGSOC KRAS wt LGSOC Primary Endpoint: Secondary Endpointsa 1:1 Randomization n = 270 Stratification Factors: • KRAS mutation status (wt vs. mt) • Geography (N. America/EU) vs. ROW • Number of prior therapies (1-3 vs. 4 or more) Inclusion Criteria RAMP 301: International Phase 3 Confirmatory Trial of Avutometinib + Defactinib in Recurrent LGSOC |
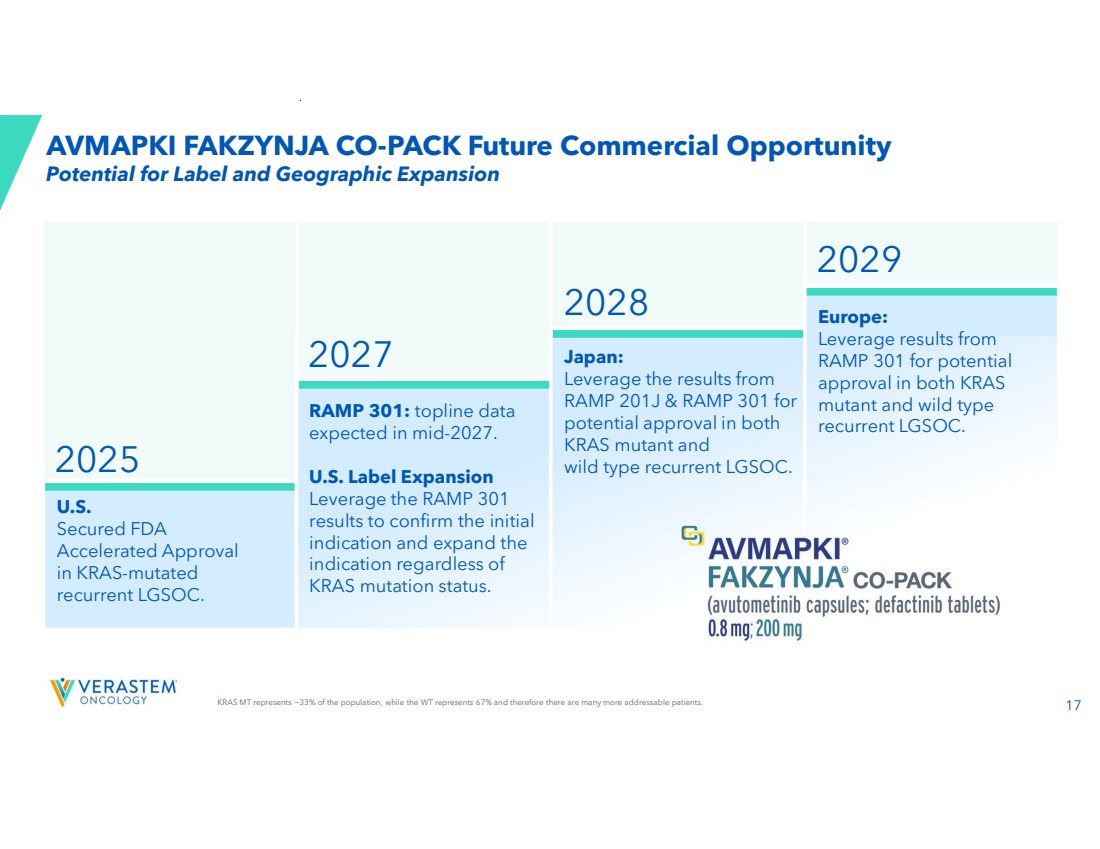
| 17 U.S. Secured FDA Accelerated Approval in KRAS-mutated recurrent LGSOC. 2029 2025 RAMP 301: topline data expected in mid-2027. U.S. Label Expansion Leverage the RAMP 301 results to confirm the initial indication and expand the indication regardless of KRAS mutation status. Japan: Leverage the results from RAMP 201J & RAMP 301 for potential approval in both KRAS mutant and wild type recurrent LGSOC. Europe: Leverage results from RAMP 301 for potential approval in both KRAS mutant and wild type recurrent LGSOC. 2028 2027 KRAS MT represents ~33% of the population, while the WT represents 67% and therefore there are many more addressable patients. Potential for Label and Geographic Expansion AVMAPKI FAKZYNJA CO-PACK Future Commercial Opportunity |
| 18 VS-7375, Oral KRAS G12D (ON/OFF) Inhibitor |
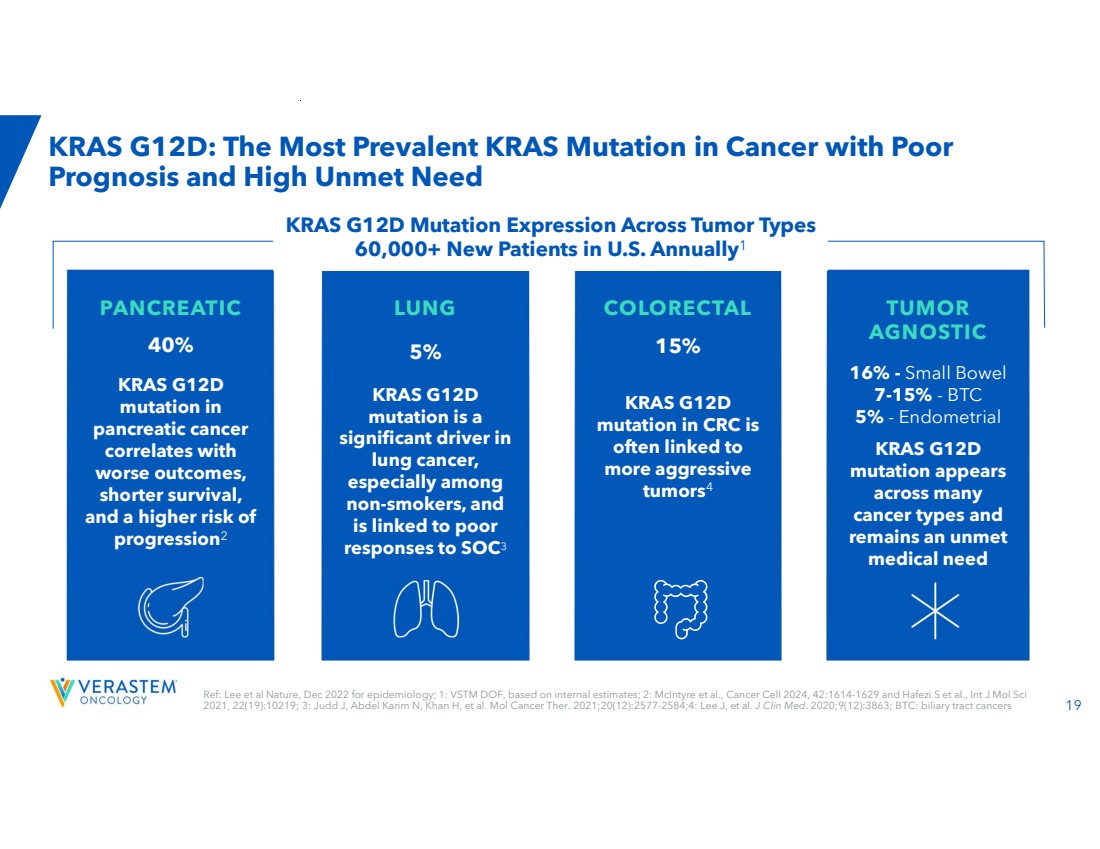
| 19 Ref: Lee et al Nature, Dec 2022 for epidemiology; 1: VSTM DOF, based on internal estimates; 2: McIntyre et al., Cancer Cell 2024, 42:1614-1629 and Hafezi S et al., Int J Mol Sci 2021, 22(19):10219; 3: Judd J, Abdel Karim N, Khan H, et al. Mol Cancer Ther. 2021;20(12):2577-2584;4: Lee J, et al. J Clin Med. 2020;9(12):3863; BTC: biliary tract cancers KRAS G12D: The Most Prevalent KRAS Mutation in Cancer with Poor Prognosis and High Unmet Need PANCREATIC 40% KRAS G12D mutation in pancreatic cancer correlates with worse outcomes, shorter survival, and a higher risk of progression2 LUNG 5% KRAS G12D mutation is a significant driver in lung cancer, especially among non-smokers, and is linked to poor responses to SOC3 COLORECTAL 15% KRAS G12D mutation in CRC is often linked to more aggressive tumors4 TUMOR AGNOSTIC 16% - Small Bowel 7-15% - BTC 5% - Endometrial KRAS G12D mutation appears across many cancer types and remains an unmet medical need KRAS G12D Mutation Expression Across Tumor Types 60,000+ New Patients in U.S. Annually1 |
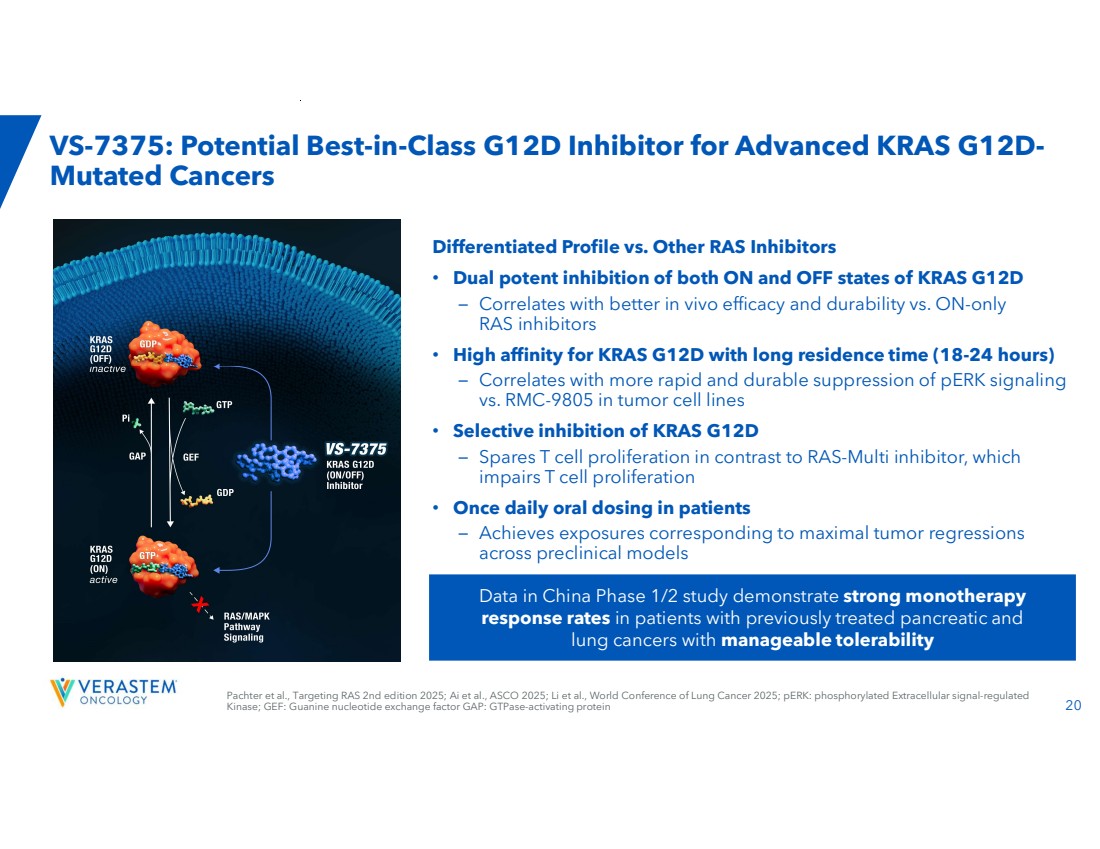
| 20 Data in China Phase 1/2 study demonstrate strong monotherapy response rates in patients with previously treated pancreatic and lung cancers with manageable tolerability Pachter et al., Targeting RAS 2nd edition 2025; Ai et al., ASCO 2025; Li et al., World Conference of Lung Cancer 2025; pERK: phosphorylated Extracellular signal-regulated Kinase; GEF: Guanine nucleotide exchange factor GAP: GTPase-activating protein VS-7375: Potential Best-in-Class G12D Inhibitor for Advanced KRAS G12D-Mutated Cancers Differentiated Profile vs. Other RAS Inhibitors • Dual potent inhibition of both ON and OFF states of KRAS G12D – Correlates with better in vivo efficacy and durability vs. ON-only RAS inhibitors • High affinity for KRAS G12D with long residence time (18-24 hours) – Correlates with more rapid and durable suppression of pERK signaling vs. RMC-9805 in tumor cell lines • Selective inhibition of KRAS G12D – Spares T cell proliferation in contrast to RAS-Multi inhibitor, which impairs T cell proliferation • Once daily oral dosing in patients – Achieves exposures corresponding to maximal tumor regressions across preclinical models |
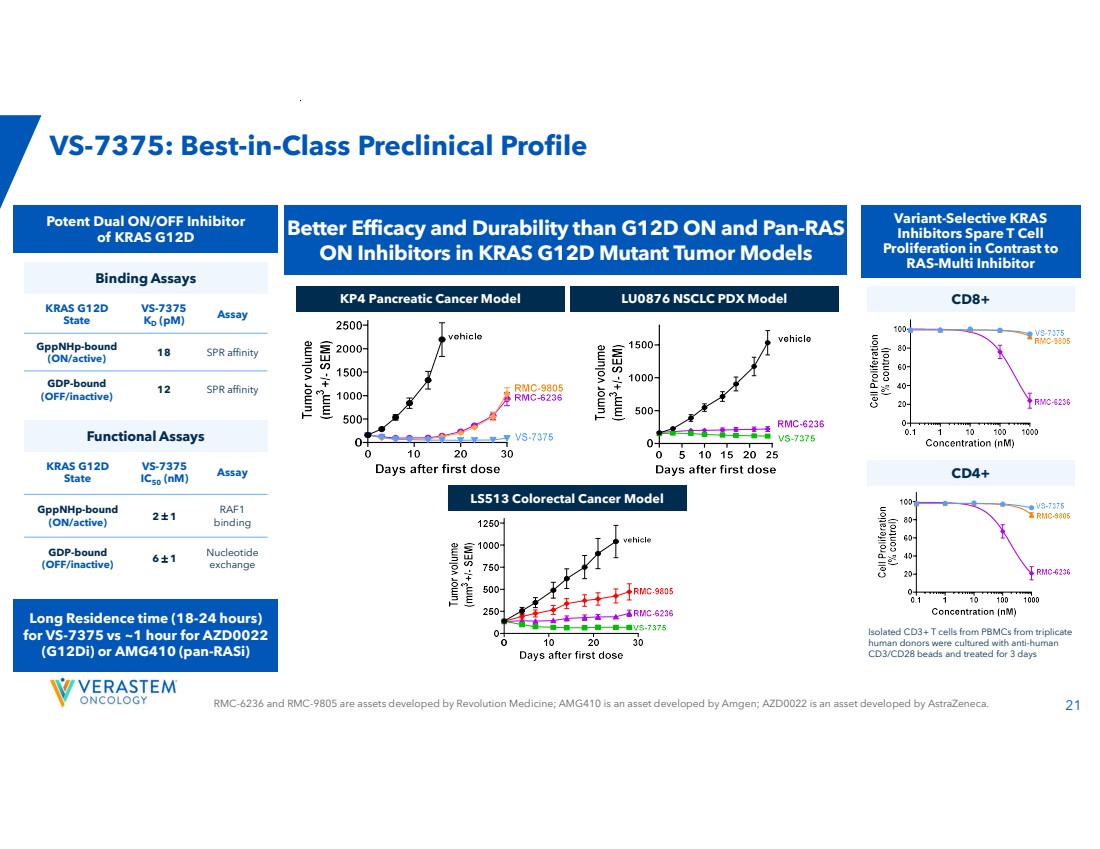
| RMC-6236 and RMC-9805 are assets developed by Revolution Medicine; AMG410 is an asset developed by Amgen; AZD0022 is an asset developed by AstraZeneca. 21 VS-7375: Best-in-Class Preclinical Profile LS513 Colorectal Cancer Model Better Efficacy and Durability than G12D ON and Pan-RAS ON Inhibitors in KRAS G12D Mutant Tumor Models Isolated CD3+ T cells from PBMCs from triplicate human donors were cultured with anti-human CD3/CD28 beads and treated for 3 days Variant-Selective KRAS Inhibitors Spare T Cell Proliferation in Contrast to RAS-Multi Inhibitor Assay VS-7375 IC50 (nM) KRAS G12D State RAF1 binding 2 1 GppNHp-bound (ON/active) Nucleotide exchange 6 1 GDP-bound (OFF/inactive) Assay VS-7375 KD (pM) KRAS G12D State 18 SPR affinity GppNHp-bound (ON/active) 12 SPR affinity GDP-bound (OFF/inactive) Functional Assays Potent Dual ON/OFF Inhibitor of KRAS G12D Long Residence time (18-24 hours) for VS-7375 vs ~1 hour for AZD0022 (G12Di) or AMG410 (pan-RASi) KP4 Pancreatic Cancer Model LU0876 NSCLC PDX Model Binding Assays CD8+ CD4+ |
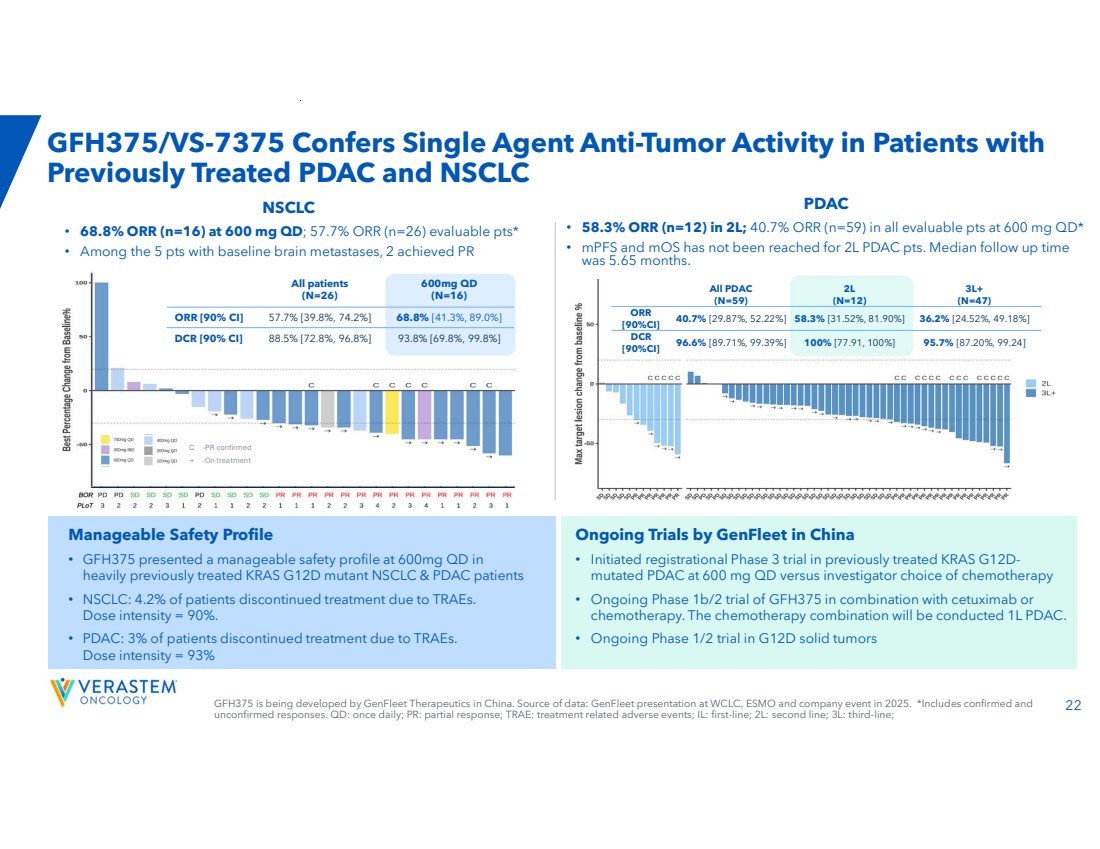
| 22 GFH375/VS-7375 Confers Single Agent Anti-Tumor Activity in Patients with Previously Treated PDAC and NSCLC PDAC • 58.3% ORR (n=12) in 2L; 40.7% ORR (n=59) in all evaluable pts at 600 mg QD* • mPFS and mOS has not been reached for 2L PDAC pts. Median follow up time was 5.65 months. C -PR confirmed → -On treatment NSCLC • 68.8% ORR (n=16) at 600 mg QD; 57.7% ORR (n=26) evaluable pts* • Among the 5 pts with baseline brain metastases, 2 achieved PR Ongoing Trials by GenFleet in China • Initiated registrational Phase 3 trial in previously treated KRAS G12D-mutated PDAC at 600 mg QD versus investigator choice of chemotherapy • Ongoing Phase 1b/2 trial of GFH375 in combination with cetuximab or chemotherapy. The chemotherapy combination will be conducted 1L PDAC. • Ongoing Phase 1/2 trial in G12D solid tumors Manageable Safety Profile • GFH375 presented a manageable safety profile at 600mg QD in heavily previously treated KRAS G12D mutant NSCLC & PDAC patients • NSCLC: 4.2% of patients discontinued treatment due to TRAEs. Dose intensity = 90%. • PDAC: 3% of patients discontinued treatment due to TRAEs. Dose intensity = 93% 600mg QD (N=16) All patients (N=26) ORR [90% CI] 57.7% [39.8%, 74.2%] 68.8% [41.3%, 89.0%] DCR [90% CI] 88.5% [72.8%, 96.8%] 93.8% [69.8%, 99.8%] 3L+ (N=47) 2L (N=12) All PDAC (N=59) 40.7% [29.87%, 52.22%] 58.3% [31.52%, 81.90%] 36.2% [24.52%, 49.18%] ORR [90%CI] 96.6% [89.71%, 99.39%] 100% [77.91, 100%] 95.7% [87.20%, 99.24] DCR [90%CI] GFH375 is being developed by GenFleet Therapeutics in China. Source of data: GenFleet presentation at WCLC, ESMO and company event in 2025. *Includes confirmed and unconfirmed responses. QD: once daily; PR: partial response; TRAE: treatment related adverse events; IL: first-line; 2L: second line; 3L: third-line; |
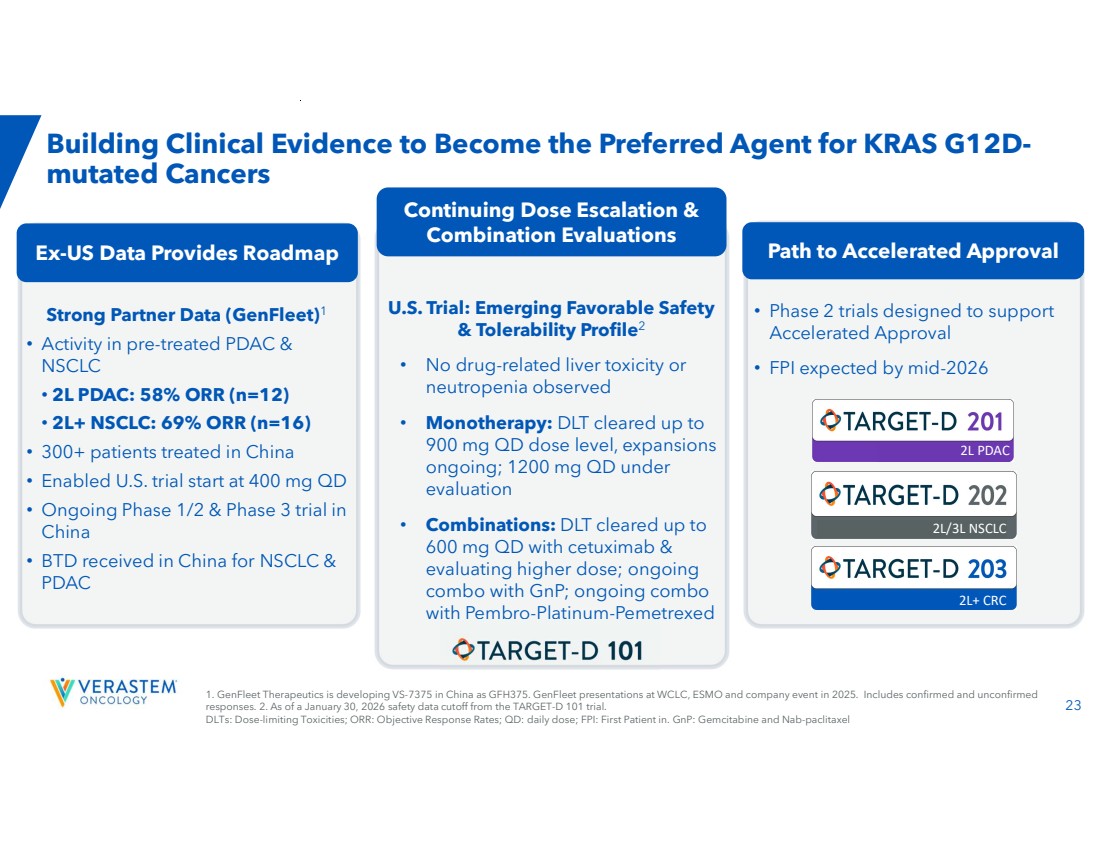
| 23 Strong Partner Data (GenFleet)1 • Activity in pre-treated PDAC & NSCLC • 2L PDAC: 58% ORR (n=12) • 2L+ NSCLC: 69% ORR (n=16) • 300+ patients treated in China • Enabled U.S. trial start at 400 mg QD • Ongoing Phase 1/2 & Phase 3 trial in China • BTD received in China for NSCLC & PDAC Ex-US Data Provides Roadmap U.S. Trial: Emerging Favorable Safety & Tolerability Profile2 • No drug-related liver toxicity or neutropenia observed • Monotherapy: DLT cleared up to 900 mg QD dose level, expansions ongoing; 1200 mg QD under evaluation • Combinations: DLT cleared up to 600 mg QD with cetuximab & evaluating higher dose; ongoing combo with GnP; ongoing combo with Pembro-Platinum-Pemetrexed Building Clinical Evidence to Become the Preferred Agent for KRAS G12D-mutated Cancers Path to Accelerated Approval Continuing Dose Escalation & Combination Evaluations • Phase 2 trials designed to support Accelerated Approval • FPI expected by mid-2026 2L PDAC 2L/3L NSCLC 2L+ CRC 1. GenFleet Therapeutics is developing VS-7375 in China as GFH375. GenFleet presentations at WCLC, ESMO and company event in 2025. Includes confirmed and unconfirmed responses. 2. As of a January 30, 2026 safety data cutoff from the TARGET-D 101 trial. DLTs: Dose-limiting Toxicities; ORR: Objective Response Rates; QD: daily dose; FPI: First Patient in. GnP: Gemcitabine and Nab-paclitaxel |
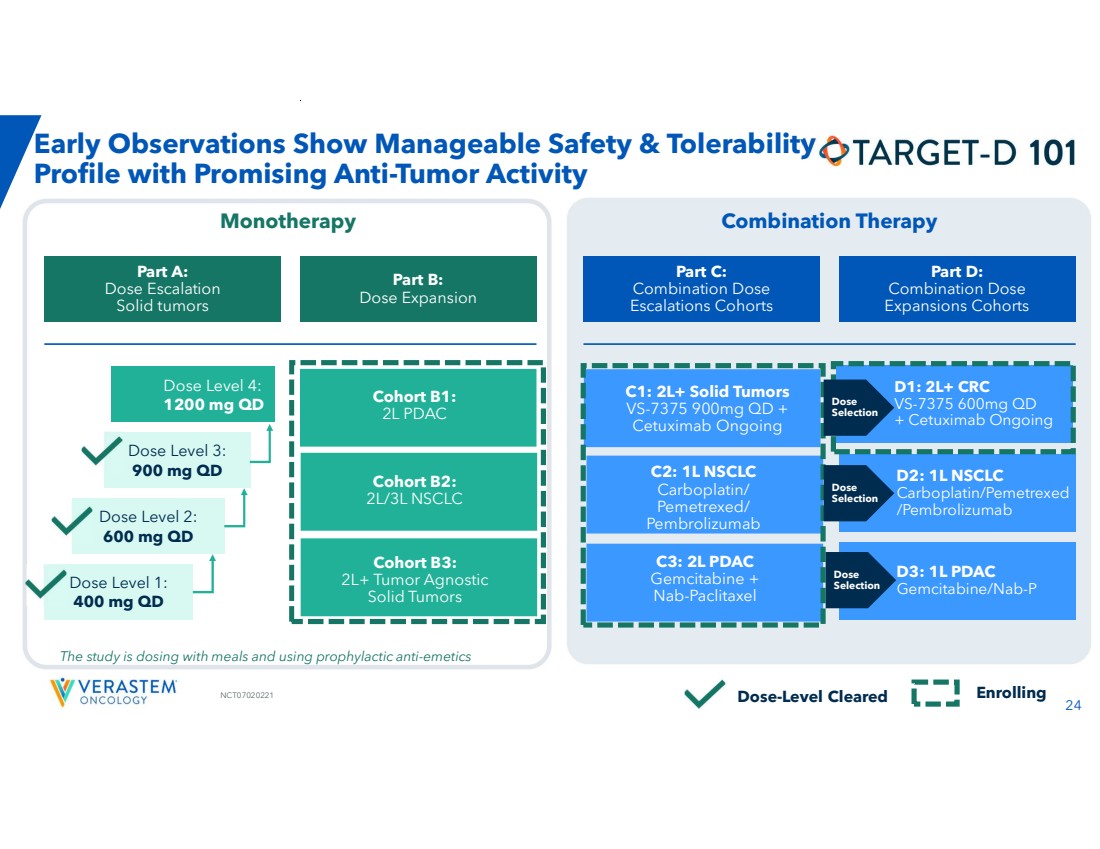
| 24 NCT07020221 D1: 2L+ CRC VS-7375 600mg QD + Cetuximab Ongoing D2: 1L NSCLC Carboplatin/Pemetrexed /Pembrolizumab D3: 1L PDAC Gemcitabine/Nab-P Early Observations Show Manageable Safety & Tolerability Profile with Promising Anti-Tumor Activity Enrolling Monotherapy Combination Therapy Part B: Dose Expansion Part C: Combination Dose Escalations Cohorts Part D: Combination Dose Expansions Cohorts Part A: Dose Escalation Solid tumors Dose Level 2: 600 mg QD Dose Level 3: 900 mg QD Dose Level 1: 400 mg QD Dose Level 4: 1200 mg QD Dose-Level Cleared The study is dosing with meals and using prophylactic anti-emetics Dose Selection Dose Selection Dose Selection C1: 2L+ Solid Tumors VS-7375 900mg QD + Cetuximab Ongoing C2: 1L NSCLC Carboplatin/ Pemetrexed/ Pembrolizumab C3: 2L PDAC Gemcitabine + Nab-Paclitaxel Cohort B3: 2L+ Tumor Agnostic Solid Tumors Cohort B2: 2L/3L NSCLC Cohort B1: 2L PDAC |
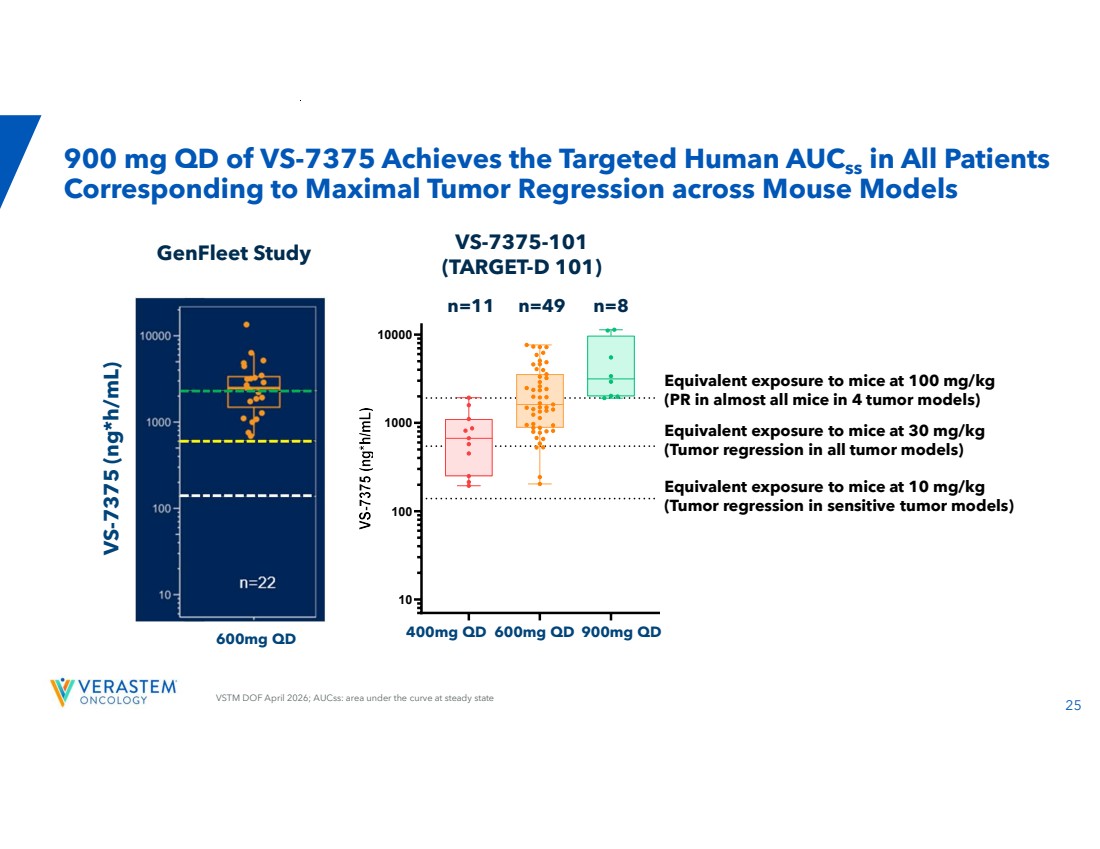
| 25 VSTM DOF April 2026; AUCss: area under the curve at steady state 400 mg 600 mg 900 mg 10 100 1000 10000 900 mg QD of VS-7375 Achieves the Targeted Human AUCss in All Patients Corresponding to Maximal Tumor Regression across Mouse Models VS-7375 (ng*h/mL) 600mg QD VS-7375-101 (TARGET-D 101) n=11 n=49 n=8 GenFleet Study 400mg QD 600mg QD 900mg QD Equivalent exposure to mice at 100 mg/kg (PR in almost all mice in 4 tumor models) Equivalent exposure to mice at 10 mg/kg (Tumor regression in sensitive tumor models) Equivalent exposure to mice at 30 mg/kg (Tumor regression in all tumor models) |
| 26 Monotherapy Dose Escalation Cohorts (All dose levels) N=231 ; mDoT, median (range): 1.6 (0.7-5.6) months (TRAEs) Gr. 1, n (%) Gr. 2, n (%) Gr. 3, n (%) Gr. ≥4, n (%) All Gr., n (%) System Organ Class Preferred Term Gastrointestinal Nausea 11 (48) 1 (4) 0 (0) 0 (0) 12 (52) Diarrhea 7 (30) 1 (4) 1 (4) 0 (0) 9 (39) Vomiting 6 (26) 0 (0) 0 (0) 0 (0) 6 (26) Abdominal pain 0 (0) 1 (4) 0 (0) 0 (0) 1 (4) Abdominal distention 2 (9) 0 (0) 0 (0) 0 (0) 2 (9) Flatulence 2 (9) 0 (0) 0 (0) 0 (0) 2 (9) General Fatigue 6 (26) 1 (4) 0 (0) 0 (0) 7 (30) Edema peripheral 1 (4) 0 (0) 0 (0) 0 (0) 1 (4) Investigations AST increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) ALT increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) Blood bilirubin increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) GGT increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) ALP increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) Amylase increased 1 (4) 1 (4) 1 (4) 0 (0) 3 (13) Lipase increased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) Blood & lymphatic/ investigations Anemia 1 (4) 1 (4) 0 (0) 0 (0) 2 (9) Neutropenia 1 (4) 1 (4) 0 (0) 0 (0) 2 (9) 2 WBC decreased 0 (0) 1 (4) 0 (0) 0 (0) 1 (4) Platelet decreased 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) Metabolism and nutrition Decreased appetite 2 (9) 1 (4) 0 (0) 0 (0) 3 (13) Nervous system Dizziness 1 (4) 0 (0) 0 (0) 0 (0) 1 (4) Headache 1 (4) 0 (0) 0 (0) 0 (0) 1 (4) Skin & subcutaneous tissue Rash maculo-papular 1 (4) 0 (0) 0 (0) 0 (0) 1 (4) VSTM DOF, Jan. 30. 2026 cutoff; mDOT: median Duration of Treatment; AST: AspartateAminotransferase; ALT: Alanine Aminotransferase;GGT: Gammaglutamyl transferase; ALP: AlkalinePhosphatase; WBC: White Blood Count; Gr: Grade 1. 9 patients at 400mg, 9 patients at 600mg, 5 patients at 900mg 2. Included neutropenia and neutrophil count decreased • No drug-related liver function test abnormalities were reported in any patient across any of the dose levels evaluated • No neutropenia >Grade 2 was reported • Rates of nausea, vomiting and diarrhea, using standard prophylactic anti-nausea agents and rapid institution of over-the-counter anti-diarrheals, are lower than those reported by our partner in China VS-7375 Safety/ Tolerability Profile |

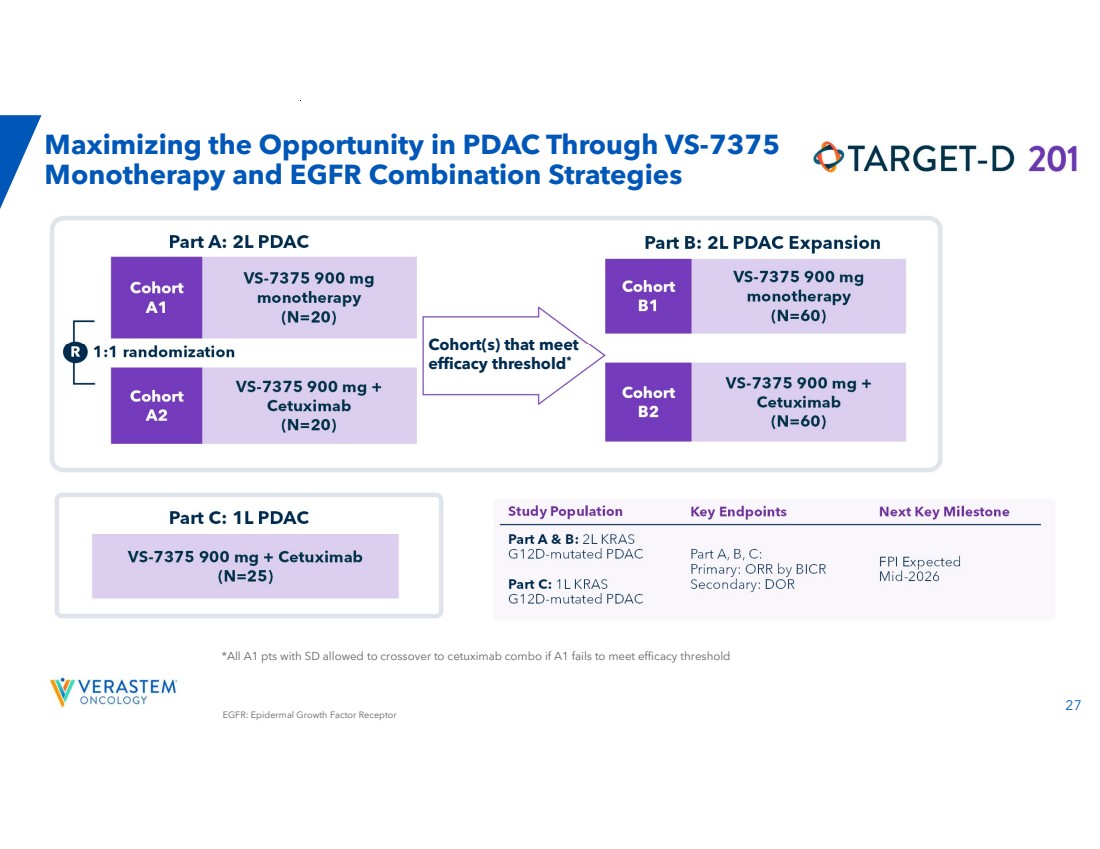
| 27 *All A1 pts with SD allowed to crossover to cetuximab combo if A1 fails to meet efficacy threshold Maximizing the Opportunity in PDAC Through VS-7375 Monotherapy and EGFR Combination Strategies R 1:1 randomization Part A: 2L PDAC Cohort A1 Cohort A2 VS-7375 900 mg monotherapy (N=20) VS-7375 900 mg + Cetuximab (N=20) Cohort B1 Cohort B2 VS-7375 900 mg monotherapy (N=60) VS-7375 900 mg + Cetuximab (N=60) Part B: 2L PDAC Expansion Cohort(s) that meet efficacy threshold* Part C: 1L PDAC VS-7375 900 mg + Cetuximab (N=25) Study Population Key Endpoints Next Key Milestone FPI Expected Mid-2026 Part A, B, C: Primary: ORR by BICR Secondary: DOR Part A & B: 2L KRAS G12D-mutated PDAC Part C: 1L KRAS G12D-mutated PDAC EGFR: Epidermal Growth Factor Receptor |
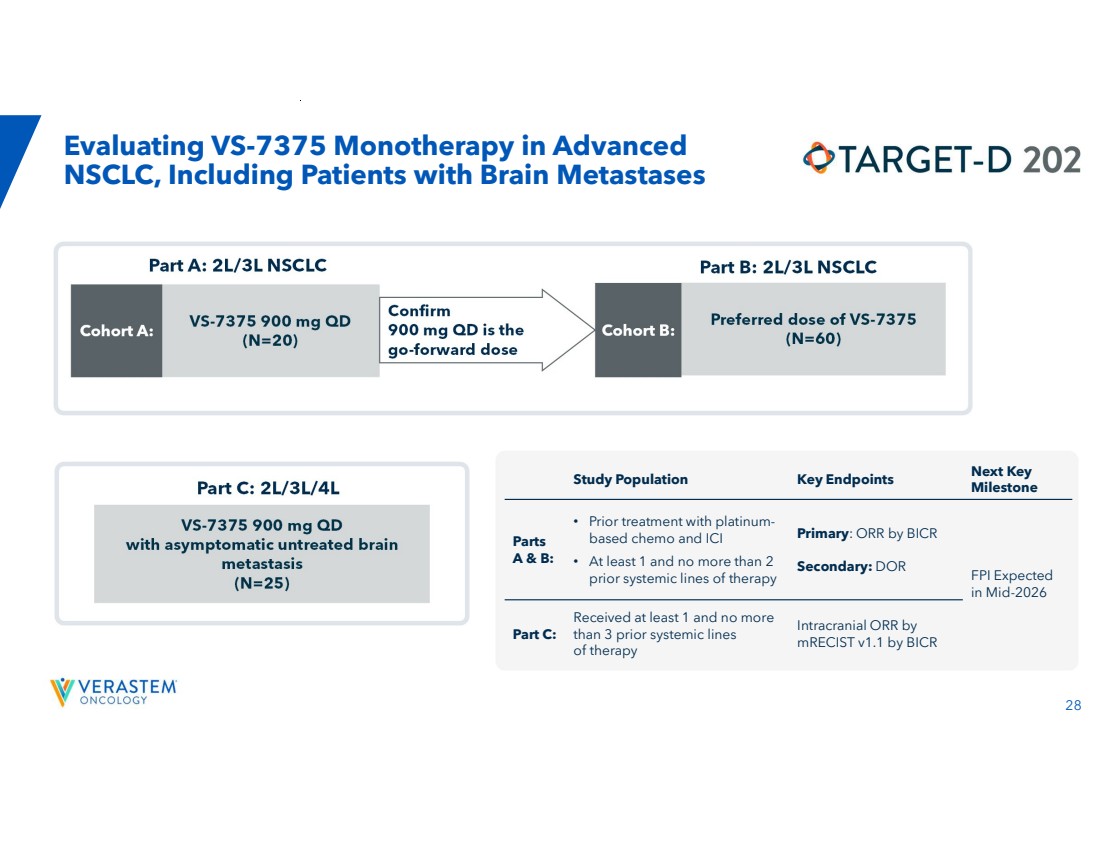
| 28 Evaluating VS-7375 Monotherapy in Advanced NSCLC, Including Patients with Brain Metastases Cohort A: Confirm 900 mg QD is the go-forward dose Part A: 2L/3L NSCLC VS-7375 900 mg QD (N=20) Cohort B: Preferred dose of VS-7375 (N=60) Part B: 2L/3L NSCLC Part C: 2L/3L/4L VS-7375 900 mg QD with asymptomatic untreated brain metastasis (N=25) Next Key Milestone Study Population Key Endpoints FPI Expected in Mid-2026 Primary: ORR by BICR Secondary: DOR • Prior treatment with platinum-based chemo and ICI • At least 1 and no more than 2 prior systemic lines of therapy Parts A & B: Intracranial ORR by mRECIST v1.1 by BICR Received at least 1 and no more than 3 prior systemic lines of therapy Part C: |
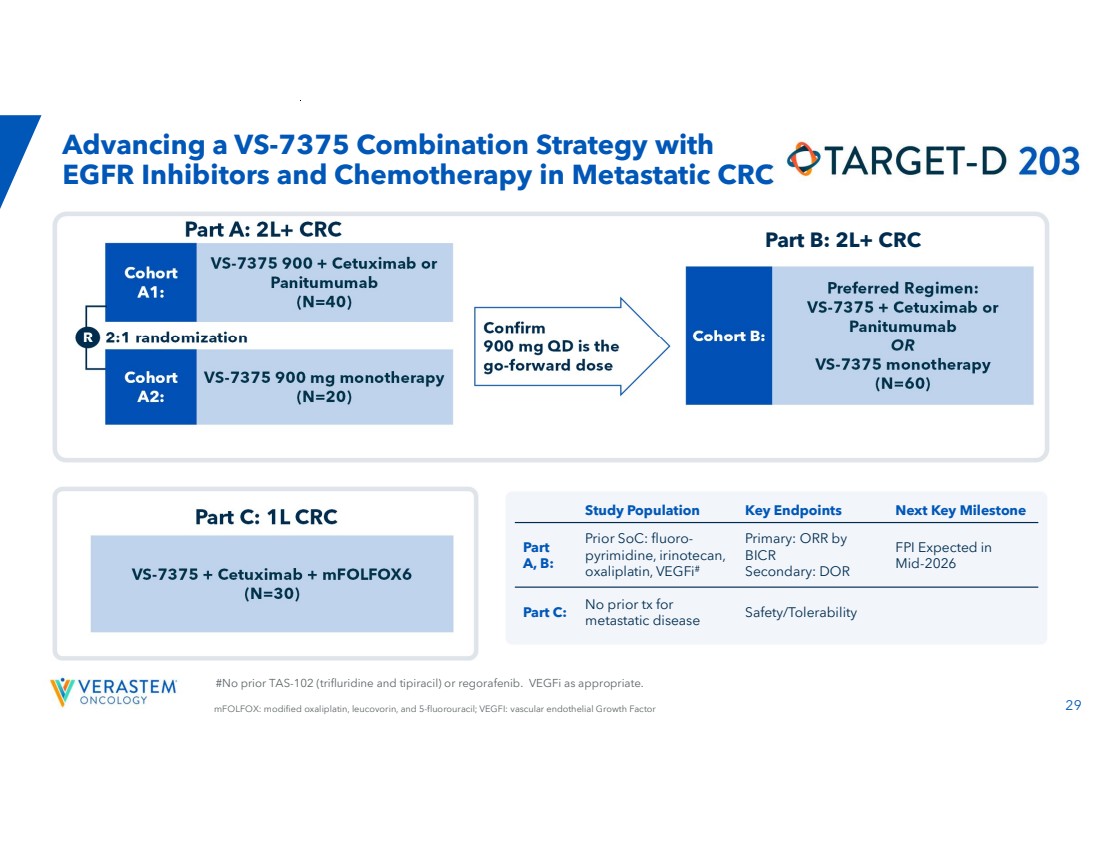
| 29 #No prior TAS-102 (trifluridine and tipiracil) or regorafenib. VEGFi as appropriate. Advancing a VS-7375 Combination Strategy with EGFR Inhibitors and Chemotherapy in Metastatic CRC Cohort A1: R Confirm 900 mg QD is the go-forward dose 2:1 randomization Cohort A2: Part A: 2L+ CRC VS-7375 900 + Cetuximab or Panitumumab (N=40) VS-7375 900 mg monotherapy (N=20) Cohort B: Preferred Regimen: VS-7375 + Cetuximab or Panitumumab OR VS-7375 monotherapy (N=60) Part C: 1L CRC VS-7375 + Cetuximab + mFOLFOX6 (N=30) Part B: 2L+ CRC mFOLFOX: modified oxaliplatin, leucovorin, and 5-fluorouracil; VEGFI: vascular endothelial Growth Factor Study Population Key Endpoints Next Key Milestone FPI Expected in Mid-2026 Primary: ORR by BICR Secondary: DOR Prior SoC: fluoro-pyrimidine, irinotecan, oxaliplatin, VEGFi# Part A, B: Safety/Tolerability No prior tx for metastatic disease Part C: |
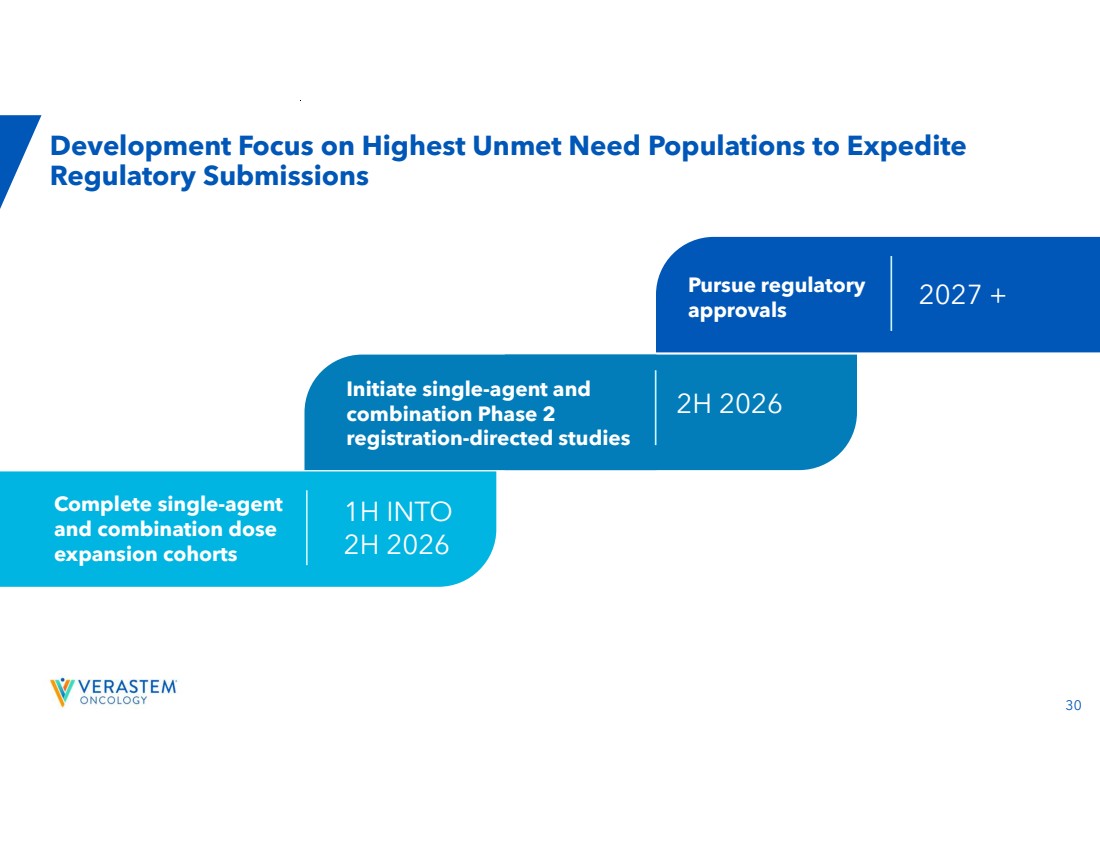
| 30 Development Focus on Highest Unmet Need Populations to Expedite Regulatory Submissions Complete single-agent and combination dose expansion cohorts 1H INTO 2H 2026 Initiate single-agent and combination Phase 2 registration-directed studies 2H 2026 Pursue regulatory approvals 2027 + |
| Topline Data from RAMP 205: Avutometinib + Defactinib + Standard of Care in First-Line Metastatic Pancreatic Cancer |

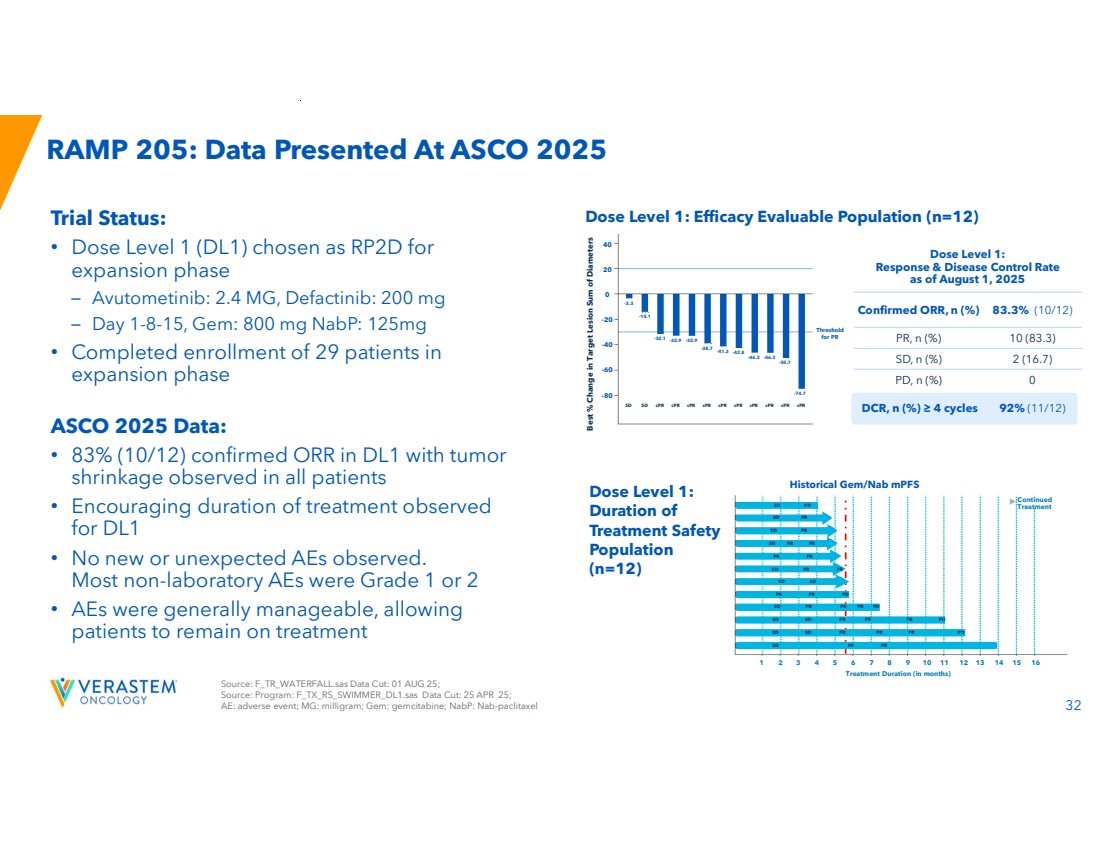
| 32 Historical Gem/Nab mPFS RAMP 205: Data Presented At ASCO 2025 Trial Status: • Dose Level 1 (DL1) chosen as RP2D for expansion phase – Avutometinib: 2.4 MG, Defactinib: 200 mg – Day 1-8-15, Gem: 800 mg NabP: 125mg • Completed enrollment of 29 patients in expansion phase ASCO 2025 Data: • 83% (10/12) confirmed ORR in DL1 with tumor shrinkage observed in all patients • Encouraging duration of treatment observed for DL1 • No new or unexpected AEs observed. Most non-laboratory AEs were Grade 1 or 2 • AEs were generally manageable, allowing patients to remain on treatment Dose Level 1: Efficacy Evaluable Population (n=12) Dose Level 1: Duration of Treatment Safety Population (n=12) Historical Gem/Nab mPFS Source: F_TR_WATERFALL.sas Data Cut: 01 AUG 25; Source: Program: F_TX_RS_SWIMMER_DL1.sas Data Cut: 25 APR 25; AE: adverse event; MG: milligram; Gem: gemcitabine; NabP: Nab-paclitaxel Threshold for PR Dose Level 1: Response & Disease Control Rate as of August 1, 2025 Confirmed ORR, n (%) 83.3% (10/12) PR, n (%) 10 (83.3) SD, n (%) 2 (16.7) PD, n (%) 0 DCR, n (%) ≥ 4 cycles 92% (11/12) Best % Change in Target Lesion Sum of Diameters 40 20 0 -20 -40 -60 -80 -3.3 -14.1 -32.1 -32.9 -32.9 -38.7 -41.3 -42.8 -46.3 -46.3 -50.7 -74.7 SD SD cPR cPR cPR cPR cPR cPR cPR cPR cPR cPR SD PD SD PR SD PR SD PR PR PR PR SD PR PR SD SD PR PR SD PR PR PR SD SD PR PR SD SD PR SD PR PR PR PR PD PR PD PD PD 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Treatment Duration (in months) Continued Treatment |
| Financials 33 |

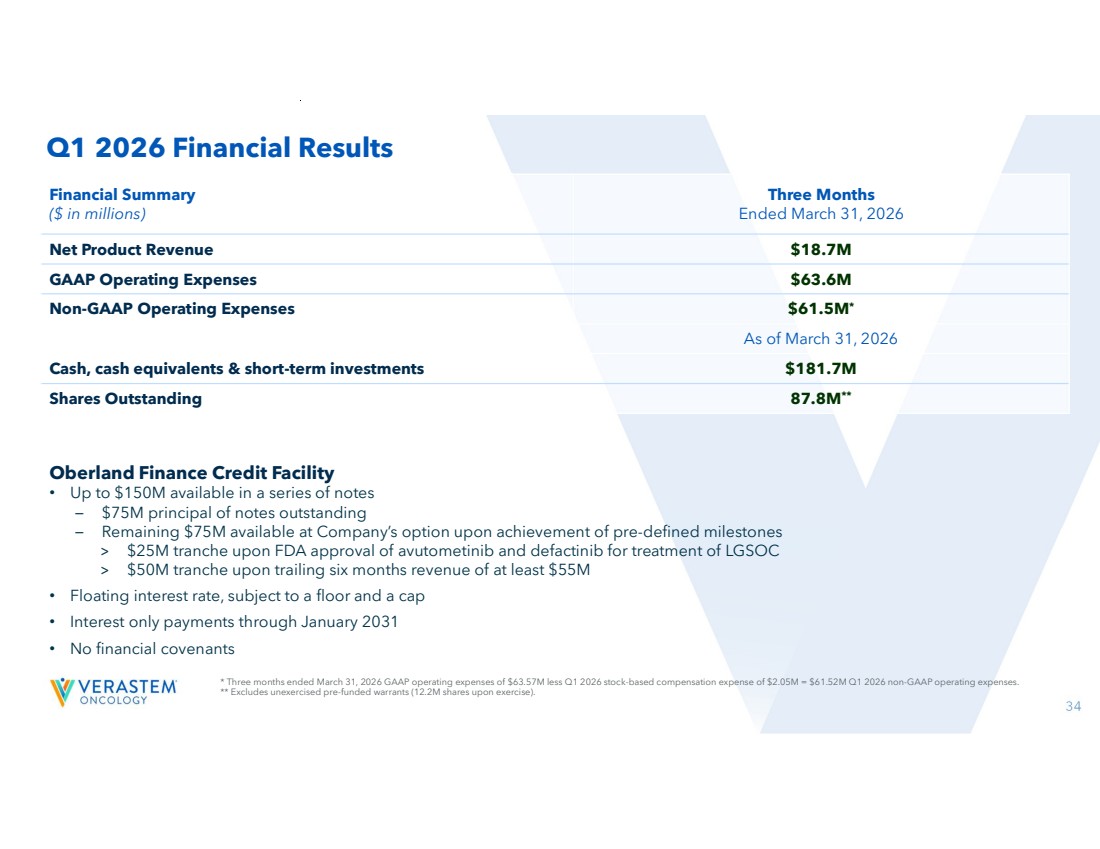
| 34 Oberland Finance Credit Facility • Up to $150M available in a series of notes – $75M principal of notes outstanding – Remaining $75M available at Company’s option upon achievement of pre-defined milestones > $25M tranche upon FDA approval of avutometinib and defactinib for treatment of LGSOC > $50M tranche upon trailing six months revenue of at least $55M • Floating interest rate, subject to a floor and a cap • Interest only payments through January 2031 • No financial covenants Three Months Ended March 31, 2026 Financial Summary ($ in millions) Net Product Revenue $18.7M GAAP Operating Expenses $63.6M Non-GAAP Operating Expenses $61.5M* As of March 31, 2026 Cash, cash equivalents & short-term investments $181.7M 87.8M** Shares Outstanding Q1 2026 Financial Results * Three months ended March 31, 2026 GAAP operating expenses of $63.57M less Q1 2026 stock-based compensation expense of $2.05M = $61.52M Q1 2026 non-GAAP operating expenses. ** Excludes unexercised pre-funded warrants (12.2M shares upon exercise). |
| 35 EU: European Union Delivering for Long-term Growth • Established commercial presence with AVMAPKI FAKZYNJA CO-PACK – RAMP 301: Fully-enrolled Phase 3 confirmatory trial has the potential to expand U.S. label and can be leveraged for EU/Japan approvals in recurrent LGSOC regardless of KRAS mutation • VS-7375 addresses significant opportunity in multiple KRAS G12D solid tumors with a differentiated profile and best-in-class anti-tumor activity – Active clinical development program advancing VS-7375 toward registration-directed studies in monotherapy and various combination approaches across multiple KRAS G12D solid tumors; expect to report early data update in 1H 2026 • Cash runway into 2027 to see key data inflection points – AVMAPKI FAKZYNJA CO-PACK franchise will be self-sustaining in 2H 2026, funding both commercial operations and avutometinib plus defactinib clinical trials |

| THANK YOU! |

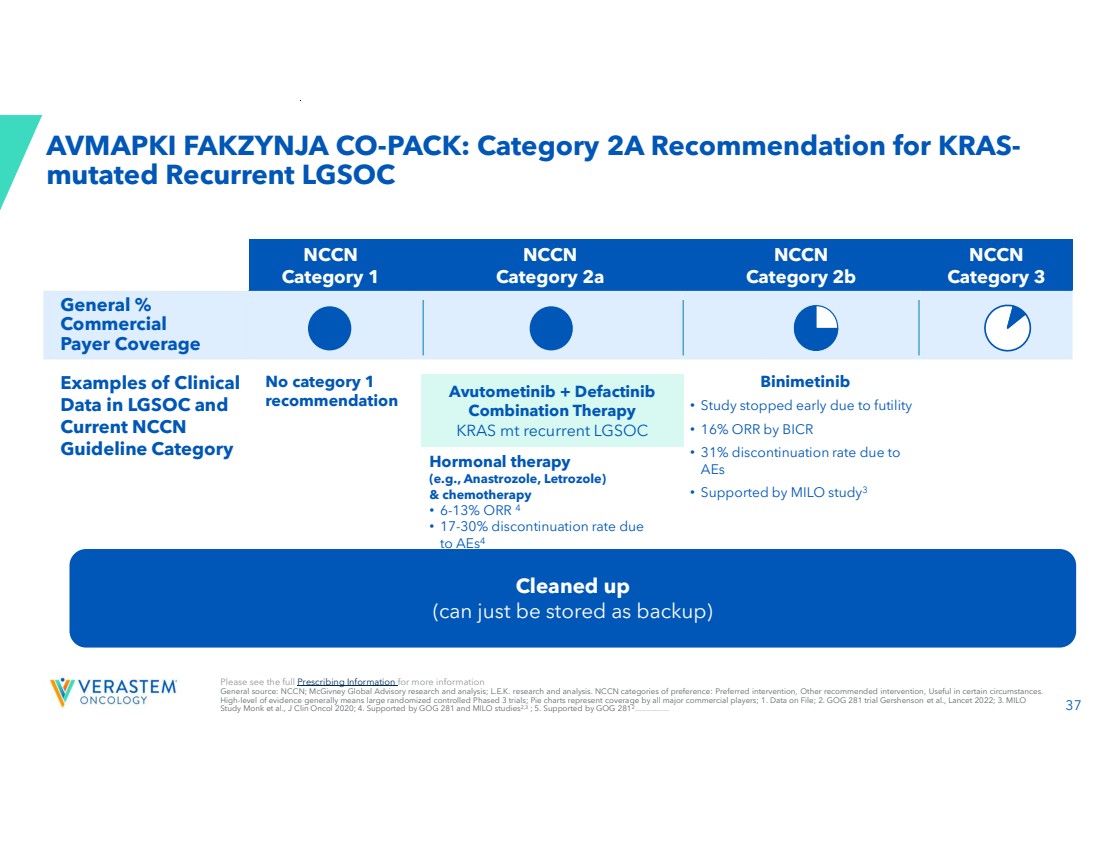
| 37 AVMAPKI FAKZYNJA CO-PACK: Category 2A Recommendation for KRAS-mutated Recurrent LGSOC NCCN Category 3 NCCN Category 2b NCCN Category 2a NCCN Category 1 General % Commercial Payer Coverage Binimetinib • Study stopped early due to futility • 16% ORR by BICR • 31% discontinuation rate due to AEs • Supported by MILO study3 Hormonal therapy (e.g., Anastrozole, Letrozole) & chemotherapy • 6-13% ORR 4 • 17-30% discontinuation rate due to AEs4 Trametinib (2-4% US utilization rate1 ) • 26% ORR by INV assessment, no BICR5 • 36% discontinuation rate due to AEs5 No category 1 recommendation Examples of Clinical Data in LGSOC and Current NCCN Guideline Category Avutometinib + Defactinib Combination Therapy KRAS mt recurrent LGSOC Please see the full Prescribing Information for more information General source: NCCN; McGivney Global Advisory research and analysis; L.E.K. research and analysis. NCCN categories of preference: Preferred intervention, Other recommended intervention, Useful in certain circumstances. High-level of evidence generally means large randomized controlled Phased 3 trials; Pie charts represent coverage by all major commercial players; 1. Data on File; 2. GOG 281 trial Gershenson et al., Lancet 2022; 3. MILO Study Monk et al., J Clin Oncol 2020; 4. Supported by GOG 281 and MILO studies2,3 ; 5. Supported by GOG 2812 ;AEs: adverse events; BICR: Blinded Independent Central Review Cleaned up (can just be stored as backup) |
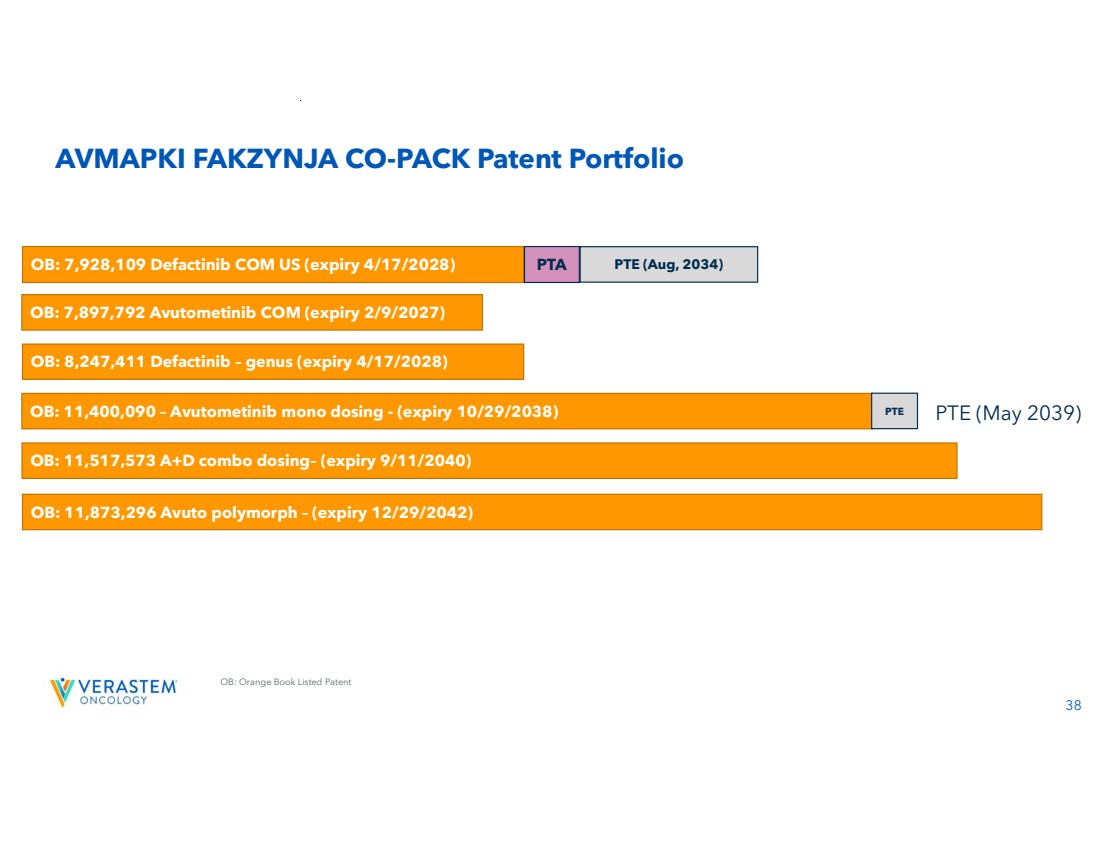
| 38 OB: Orange Book Listed Patent AVMAPKI FAKZYNJA CO-PACK Patent Portfolio OB: 7,897,792 Avutometinib COM (expiry 2/9/2027) OB: 11,400,090 – Avutometinib mono dosing - (expiry 10/29/2038) PTE OB: 7,928,109 Defactinib COM US (expiry 4/17/2028) PTA PTE (Aug, 2034) OB: 8,247,411 Defactinib – genus (expiry 4/17/2028) OB: 11,517,573 A+D combo dosing– (expiry 9/11/2040) OB: 11,873,296 Avuto polymorph – (expiry 12/29/2042) PTE (May 2039) |