UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the
Securities Exchange Act of 1934
Date of Report (Date of earliest event reported):
(Exact name of registrant as specified in its charter)
|
(State or Other Jurisdiction of Incorporation) |
(Commission File Number) |
(I.R.S. Employer Identification No.) |
|
|
|
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code:
Former name or former address, if changed since last report: Not applicable
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading symbol(s) | Name of each exchange on which registered |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule
405 of the Securities Act of 1933 (17 CFR §230.405) or Rule 12b-2 of the Securities Exchange Act of 1934 (17 CFR §240.12b-2). Emerging
growth company
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01. | Regulation FD Disclosure. |
On May 14, 2026, Corvus Pharmaceuticals, Inc. presented final data from its randomized, blinded, placebo-controlled Phase 1 clinical trial evaluating soquelitinib in patients with moderate-to-severe atopic dermatitis. A copy of the press release is furnished as Exhibit 99.1 to this Current Report on Form 8-K.
The information set forth in this Item 7.01 and in the press release attached hereto as Exhibit 99.1 are deemed to be “furnished” and shall not be deemed to be “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that Section. The information set forth in this Item 7.01, including Exhibit 99.1 shall not be deemed incorporated by reference into any filing under the Exchange Act or the Securities Act of 1933, as amended, except to the extent that the Company specifically incorporates it by reference.
| Item 8.01. | Other Events. |
The trial enrolled 72 patients with moderate-to-severe atopic dermatitis that previously failed one prior topical or systemic therapy. Thirty-five percent of the patients had received a prior systemic therapy. In each of cohorts 1-3, 16 patients were randomized in a 3:1 ratio to receive one of three 28-day dosing regimens (100 mg twice daily, 200 mg once daily or 200 mg twice daily) of soquelitinib or equivalent placebo. In cohort 4, 24 patients were randomized in a 1:1 ratio to receive a 56-day, 200 mg twice daily dosing regimen of soquelitinib or equivalent placebo. Patients in the study were monitored for a 30-day post treatment follow up period, except in cohort 3, which had an extended 90-day post treatment follow up period.
Clinical Highlights from Soquelitinib Phase 1 Atopic Dermatitis Clinical Trial
The data demonstrated safety and positive efficacy results, including in patients who received prior systemic therapy and were treatment resistant. In addition, there was a dose dependent efficacy trend in cohorts 1-3, and additional clinical benefit was observed with longer treatment in cohort 4. Across all four cohorts, no significant safety issues were observed. Reported adverse events occurred in 41.7% of soquelitinib patients and 41.7% of placebo patients; all were Grade 1-2 and did not result in any dose modifications or interruptions. No severe or serious adverse events were reported. No significant lab abnormalities were seen.
Key efficacy results from cohorts 3 and 4 (200 mg twice daily) include:
| • | Cohort 3: 50% of soquelitinib patients achieved EASI 75, 8% achieved EASI 90 and 25% achieved IGA 0/1 |
| • | Cohort 4: 75% of soquelitinib patients achieved EASI 75, 25% achieved EASI 90 and 33% achieved IGA 0/1 |
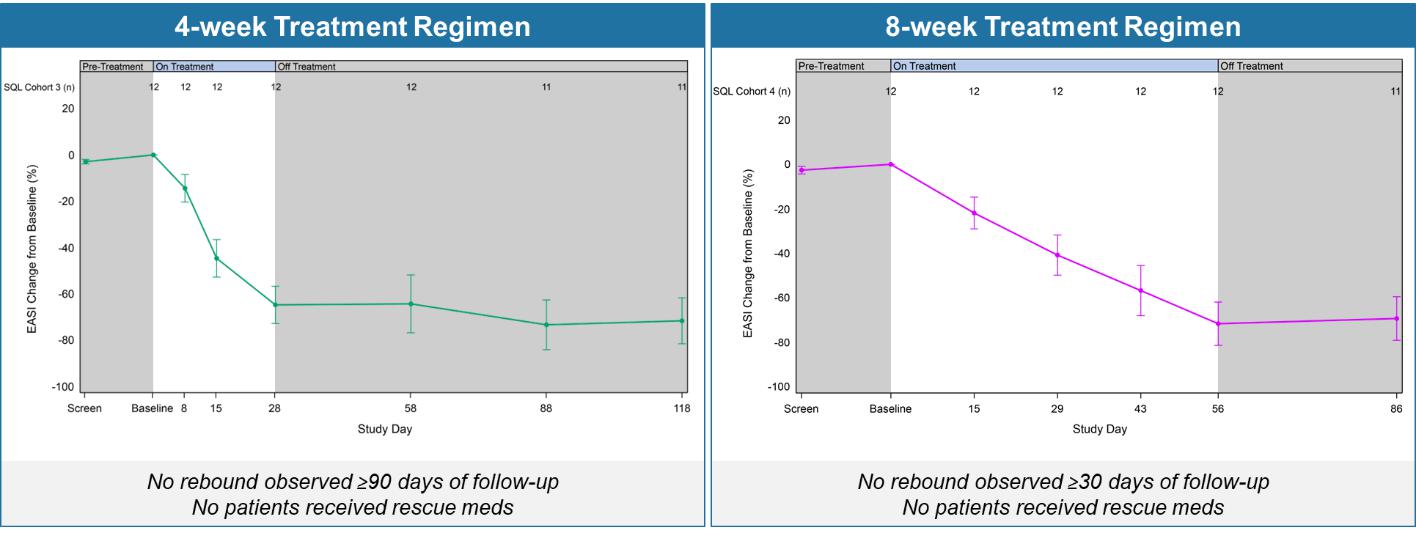
| • | In both cohorts 3 and 4, disease control continued throughout the post treatment follow up periods (90 and 30 days, respectively), see Figure 1 below; this compares to published data from approved systemic therapies that show a worsening or rebound of disease usually occurring within four weeks of stopping therapy and in some instances requiring the need for rescue medication. |
Figure 1 below shows the percent reduction in EASI for cohort 3 (left) and cohort 4 (right). No disease rebound was observed and no rescue medications were required.
Figure 1: Soquelitinib Treatment Leads to Durable Remissions with No Rebound Following Four and Eight Weeks of Treatment.
Figure 2 below shows the durability of remission in patients achieving EASI 75 and IGA 0/1 in cohorts 3 and 4. The percent of patients achieving EASI 75 and IGA0/1 is maintained during the drug-free follow up period.
Figure 2: Percentage Patients Achieving EASI 75 and IGA 0/1.
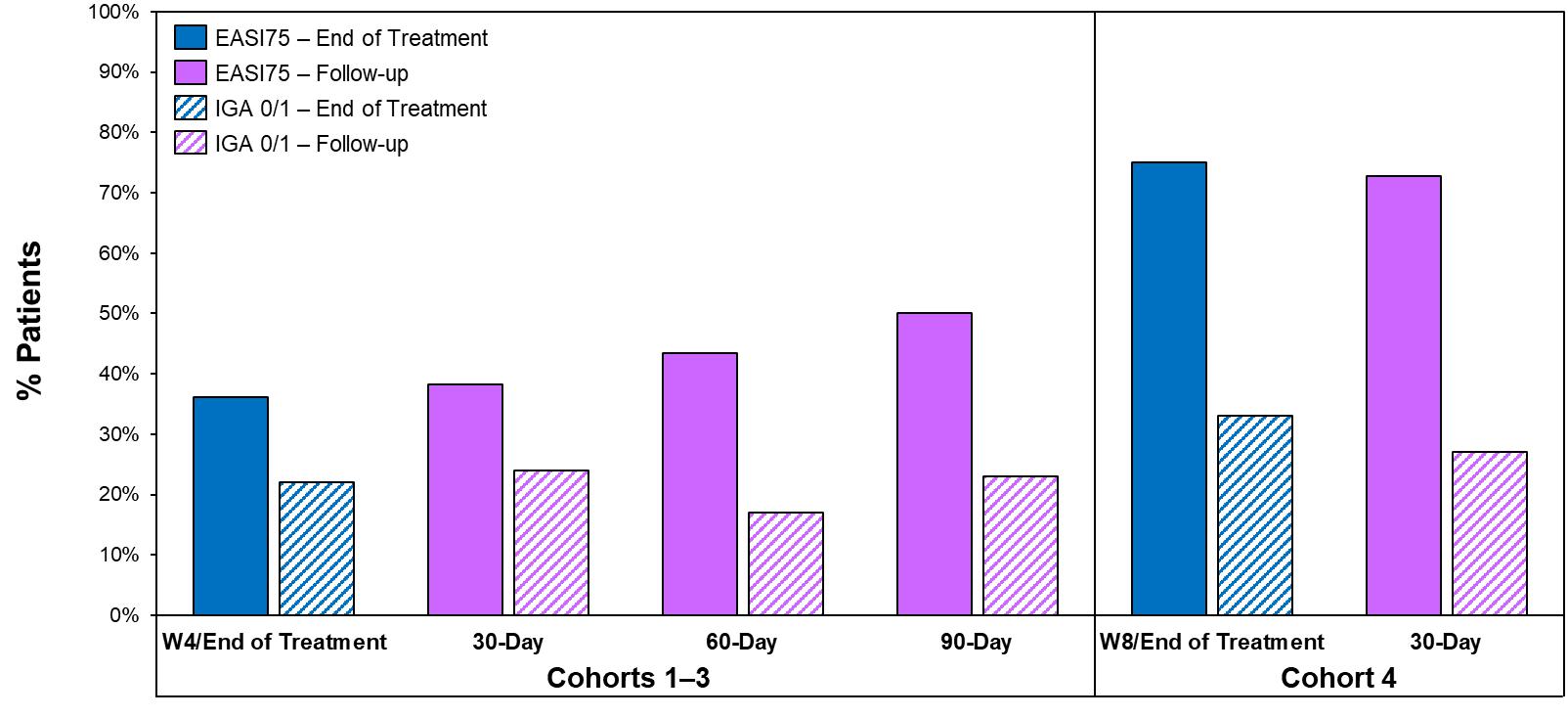
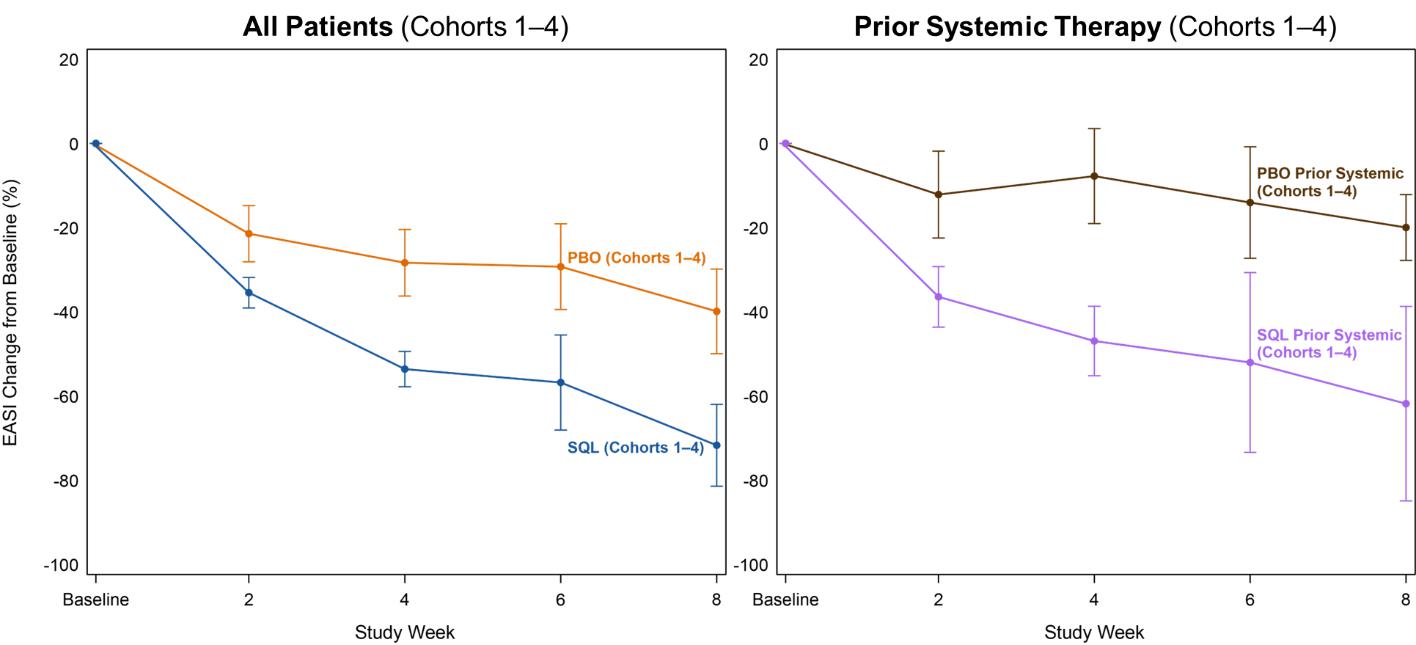
Figure 3 below shows the percent reduction in EASI scores for all patients (left) in cohorts 1-4 and the EASI curves for patients who had received prior systemic therapies (right). The data shows comparable efficacy in patients with prior systemic therapy and the all patients group.
Figure 3: Efficacy in Patients with Prior Systemic Therapy (Cohorts 1–4).
Biomarker Highlights and Immunologic Studies from Soquelitinib Phase 1 Atopic Dermatitis Clinical Trial
Soquelitinib is designed to specifically bind and inhibit ITK in T cells, modulating T cell signaling and differentiation. This results in the blockade of Th2 and Th17 cell function and their secretion of various inflammatory cytokines such as IL-4, IL-5, IL-13, IL-17 and others. ITK also regulates a switch from Th17 cell differentiation to T regulatory (Treg) cells, which suppress inflammation and autoimmunity. Inhibition of ITK by soquelitinib produces a reduction of Th17 and an increase in Treg function. Immunologic and molecular studies on peripheral blood taken from patients in the study were conducted and support soquelitinib’s mechanism of action, including the potential for drug-free remissions:
| • | Blocking Th2 and Th17 function and their related downstream cytokines (IL-4, IL-5, IL-13). See Figures 4a and 4b below. |
| • | Increasing persistent Treg cells, both during treatment and in the post-treatment, drug-free period, by regulating the switch to Treg cells from Th17 cells. See Figures 5a and 5b below. |
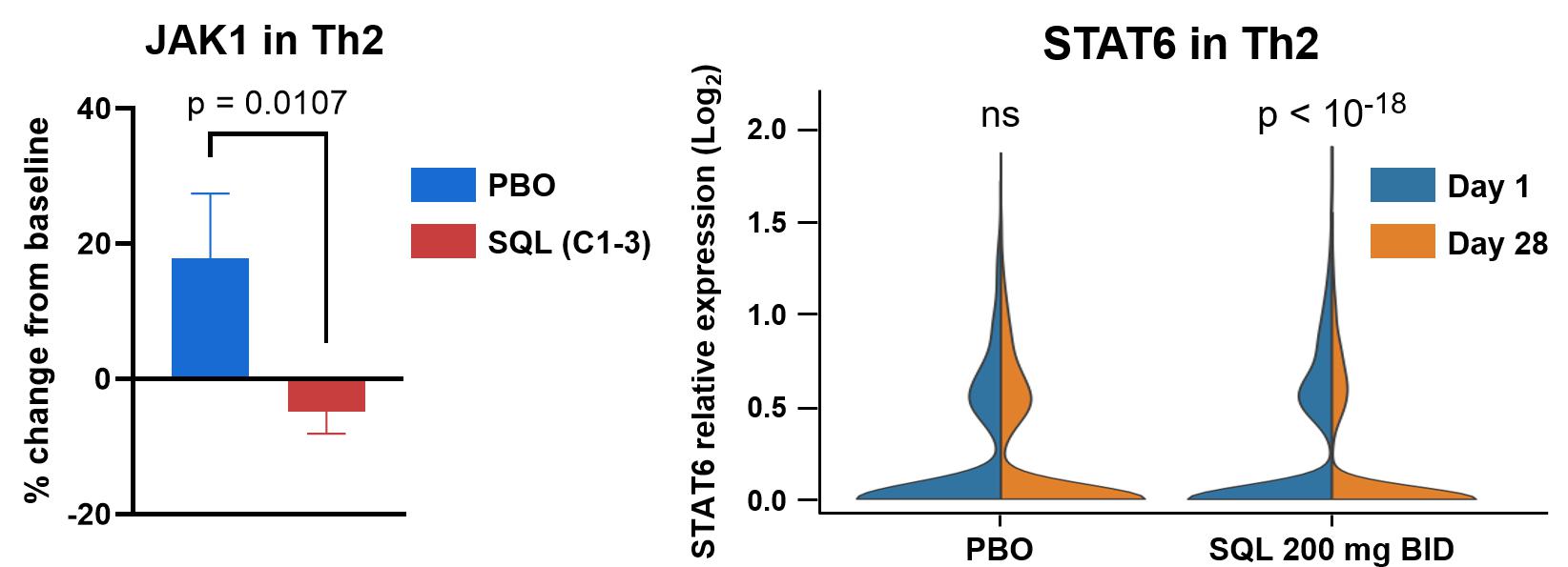
| • | Inhibiting JAK-STAT signaling, upregulating SOCS3 (suppressor of cytokine signaling 3 protein, a negative regulator of JAK-STAT signaling) and reducing JAK1 and STAT6. See Figures 6a and 6b below. |
Together, these immunomodulatory effects reduce inflammation and restore immune balance by enhancing Treg function. The observed clinical manifestations of these effects are 1) prompt responses; 2) clinical responses that are durable without rebound; and 3) specificity of soquelitinib for ITK confers safety without immunosuppression.
Figure 4a below shows a dose dependent reduction in proliferating circulating Th2 cells measured by scRNAseq in blood from patients evaluated in cohorts 1-3 receiving placebo, soquelitinib 200 mg once a day or 200 mg twice per day. Each dot represents a patient with changes compared to baseline. (Ki-67, proliferation marker; GATA3, c-MAF, CCR4 and PTGDR2 are Th2 markers; STAT6 is involved in inflammatory signaling.)
Figure 4a: Dose-dependent Reduction in Proliferating Th2*.
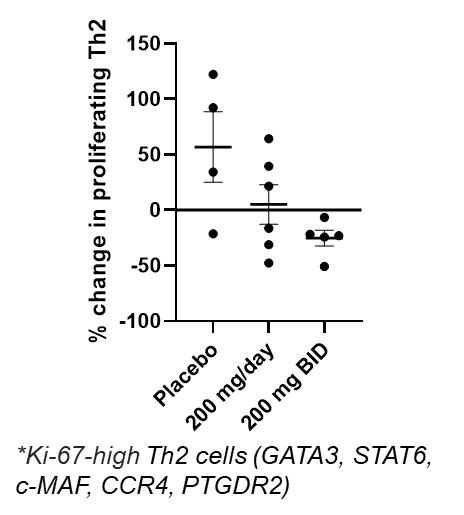
Figure 4b below shows median values of serum cytokines measured over time from cohorts 3 and 4. The decrease in levels of Th2 cytokines and TARC continue after the treatment is discontinued (drug-free period).
Figure 4b: Reduction in IL-4, IL-5, IL-13 and TARC.
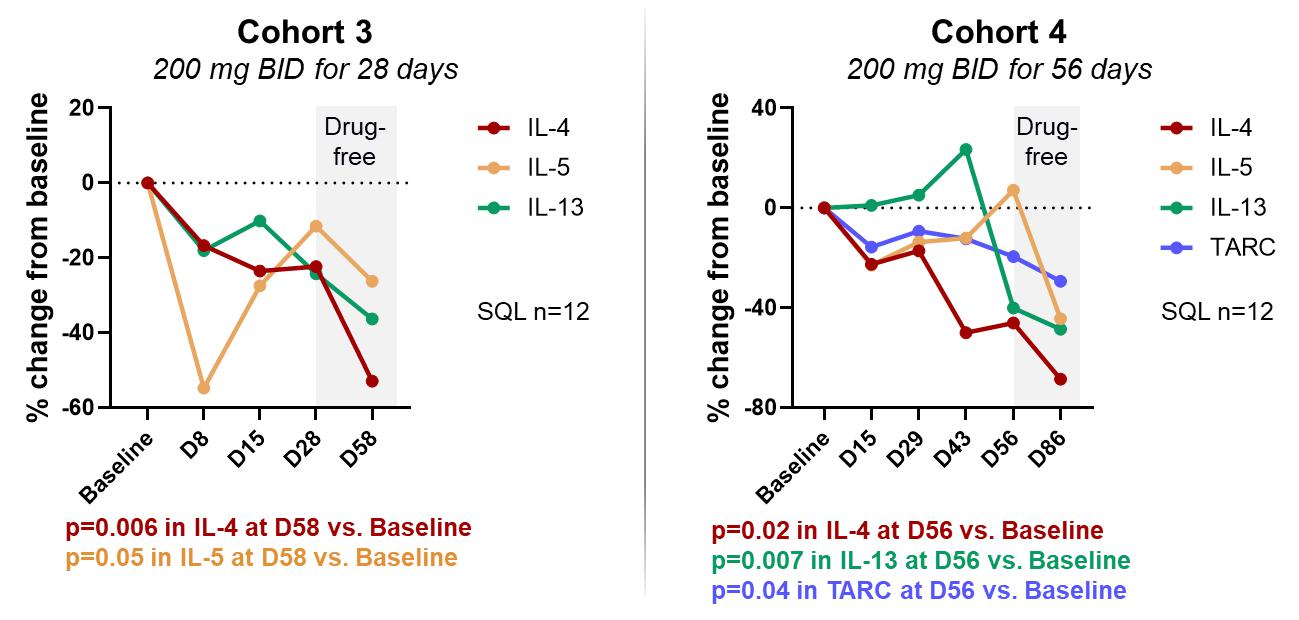
Figure 5a below shows percent change from baseline in circulating Treg cells for placebo (N=23 for cohort 1-4 combined) and treated patients (N=24) from cohort 3, cohort 4 and combined. The top row shows values after 28 days of therapy and the bottom row shows values 30 days after stopping therapy (drug-free period).
Figure 5a: Soquelitinib Treatment Leads to Increase in Persistent Tregs (CD4+, Foxp3+, CD25Hi ) measured by flow cytometry.
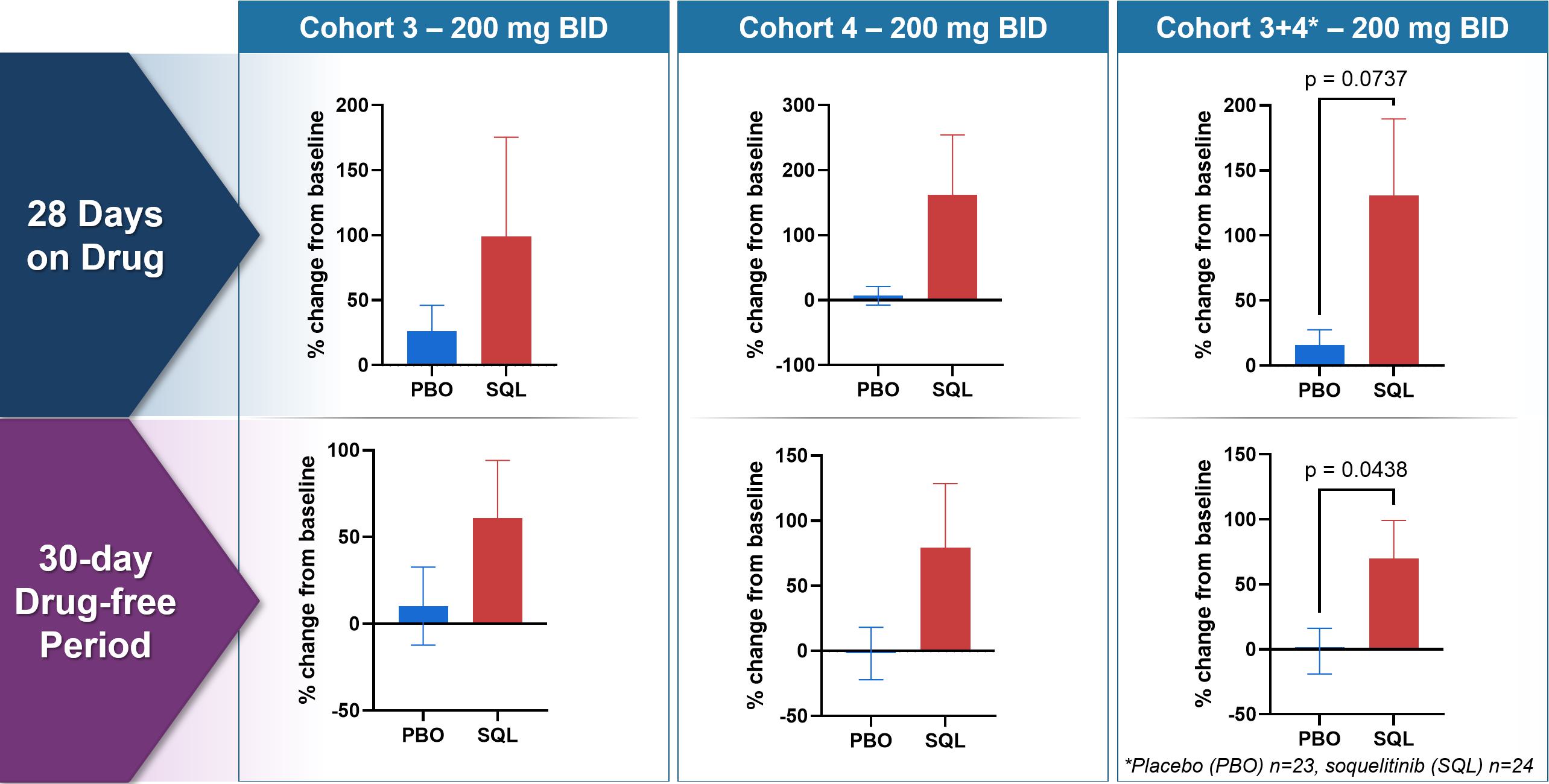
Figure 5b below shows changes from baseline for markers of Tregs and Th17 cells (patients as in Figure 4). BACH2 is a transcription factor that promotes Treg function and stability by binding to Foxp3 promotor. RORγT is the master transcription factor for Th17 cell function. The data demonstrates an increase in Tregs and a decrease in Th17, consistent with soquelitinib induced “switch.”
Figure 5b: Inhibiting ITK Regulates Switch to Treg from Th17 - Increased BACH2 and Reduced RORγT Expression measured using scRNAseq.
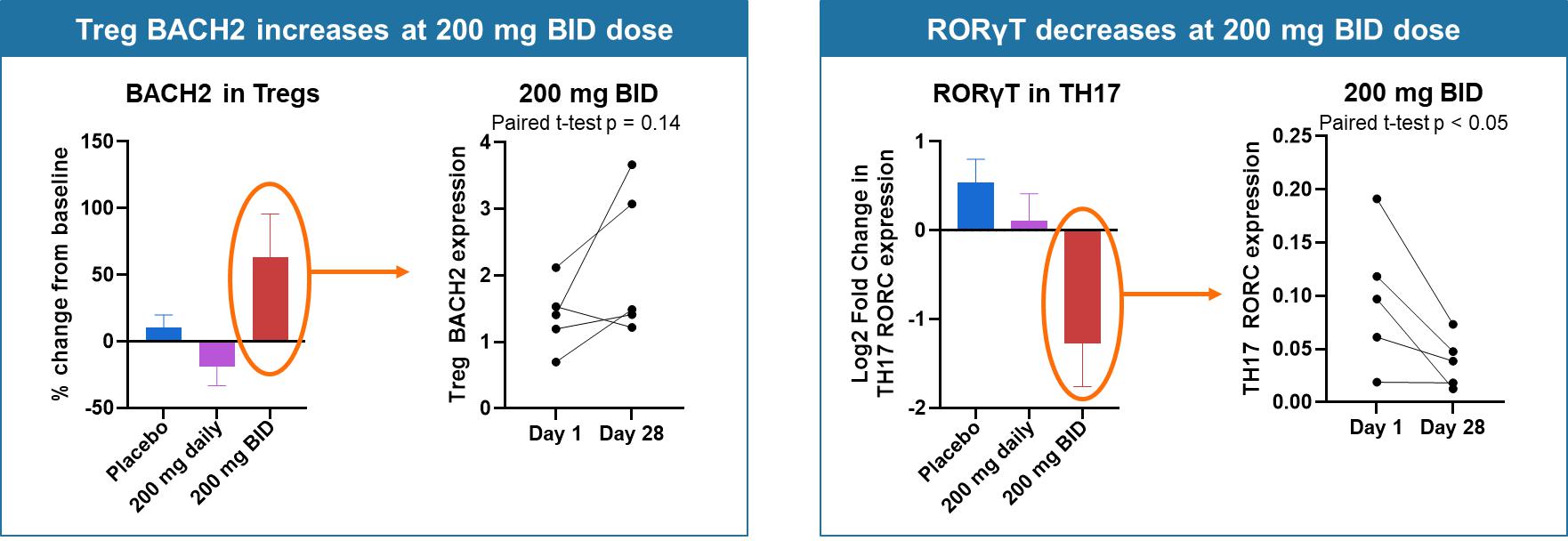
Figure 6a below shows percent change from baseline of SOCS3 (suppressor of cytokine signaling-3) in Th2, Th1 and Tc17 cells for placebo and treated patients from cohorts 1-3. SOCS3 regulates cytokine signaling in the JAK/STAT pathway, with increased levels of SOCS3 inhibiting T cell responses to cytokines. Tc17 cells produce IL-17, demonstrate high plasticity, are driven by transcription factor RORγT and are important in autoimmune diseases. These findings indicate that soquelitinib will reduce IL-17 production.
Figure 6a: SOCS3 Increases in Circulating T cells.
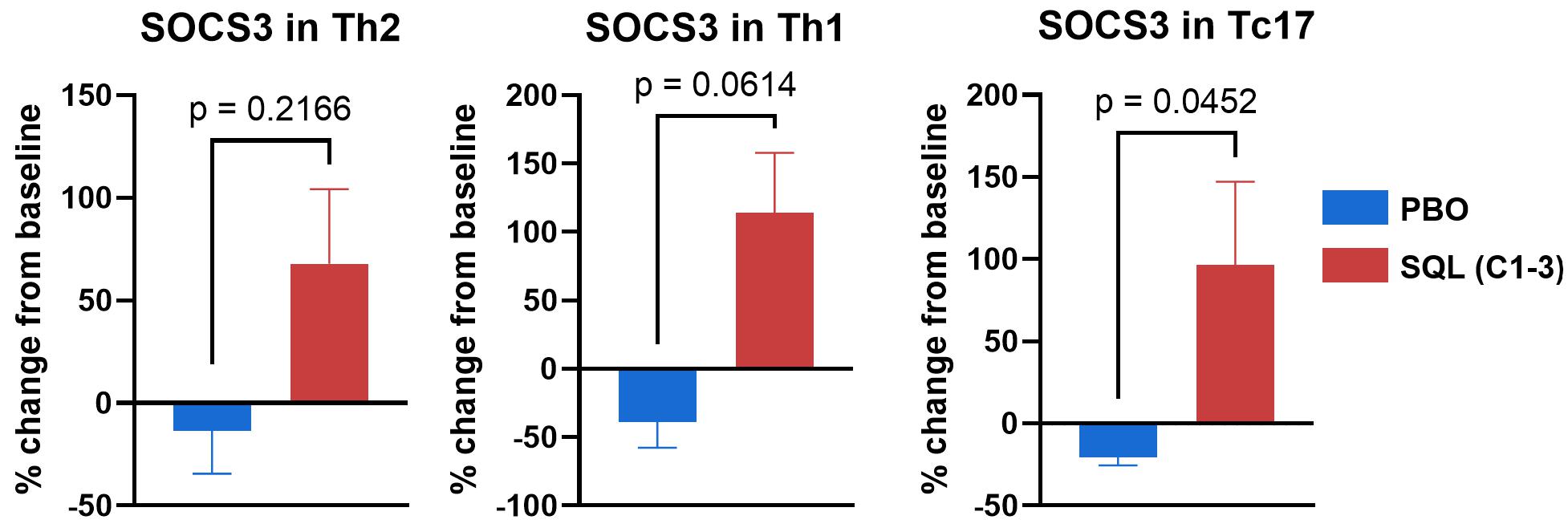
Figure 6b below shows change from baseline (Cohorts 1-3) in JAK1 and STAT6 resulting from treatment with soquelitinib compared to placebo. The violin plots on the right show a reduction in STAT6 expression at day 28 (gold) compared to baseline (blue) for the 200 mg twice daily (N=5) patients; no significant change was seen in placebo (N=4) patients.
Figure 6b: JAK1 and STAT6 Decreases in Circulating Th2 Cells measured by scRNAseq.
Forward-Looking Statements
This Current Report on Form 8-K contains forward-looking statements, including statements related to soquelitinib’s potential, including efficacy, safety and ability to provide durable, drug-free remissions. All statements other than statements of historical fact contained in this report are forward-looking statements. These statements often include words such as “believe,” “expect,” “anticipate,” “intend,” “plan,” “estimate,” “seek,” “will,” “may” or similar expressions. Forward-looking statements are subject to a number of risks and uncertainties, many of which involve factors or circumstances that are beyond the Company’s control. The Company’s actual results could differ materially from those stated or implied in forward-looking statements due to a number of factors, including but not limited to, risks detailed in the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2026, filed with the Securities and Exchange Commission on May 7, 2026, as well as other documents that may be filed by the Company from time to time with the Securities and Exchange Commission. In particular, the following factors, among others, could cause results to differ materially from those expressed or implied by such forward-looking statements: the Company’s ability to demonstrate sufficient evidence of efficacy and safety in its clinical trials of its product candidates; the accuracy of the Company’s estimates relating to its ability to initiate and/or complete preclinical studies and clinical trials and release data from such studies and clinical trials; the results of preclinical studies and interim data from clinical trials not being predictive of future results; the Company’s ability to enroll sufficient numbers of patients in its clinical trials; the unpredictability of the regulatory process; regulatory developments in the United States and foreign countries; the costs of clinical trials may exceed expectations; the Company’s ability to accurately estimate the cash on hand providing funding into the second quarter of 2028 and the Company’s ability to raise additional capital. Although the Company believes that the expectations reflected in the forward-looking statements are reasonable, it cannot guarantee that the events and circumstances reflected in the forward-looking statements will be achieved or occur, and the timing of events and circumstances and actual results could differ materially from those projected in the forward-looking statements. Accordingly, you should not place undue reliance on these forward-looking statements. All such statements speak only as of the date made, and the Company undertakes no obligation to update or revise publicly any forward-looking statements, whether as a result of new information, future events or otherwise.
Item 9.01 Financial Statements and Exhibits.
| Exhibit No. | Description | |
| 99.1 | Press release of Corvus Pharmaceuticals, Inc. dated May 14, 2026. | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document) |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| CORVUS PHARMACEUTICALS, INC. | |||
| Date: May 14, 2026 | By: | /s/ Leiv Lea | |
| Leiv Lea | |||
| Chief Financial Officer | |||