| December 2023 NASDAQ: NRBO 1 January 2026 MetaVia Inc. NASDAQ: MTVA Issuer Free Writing Prospectus Filed Pursuant to Rule 433 Relating to Form S-1 dated January 5, 2026 Registration Statement No. 333-292581 January 5, 2026 |

| 2 Forward-Looking Statements MetaVia Inc. (the “Company,” “we,” or “us” or “our”) is offering Class A Units, with each Class A Unit consisting of (i) one share of our common stock, par value $0.001 per share and (ii) one Series C common warrant to purchase one share of common stock, and Class B Units with each Class B Unit consisting of (i) one pre-funded warrant to purchase one share of common stock and (ii) one Series C common warrant to purchase one share of common stock (the "Securities") in a public offering (the "Offering"). The proceeds of the Offering are intended primarily for working capital and general corporate purposes, including to continue the clinical development of DA-1726 for the treatment of obesity. This presentation (the “Presentation”) includes forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. Forward-looking statements include all statements that do not relate solely to historical or current facts and can be identified by the use of words such as “believes”, “expects”, “anticipates”, “may”, “will”, “should”, “seeks”, “approximately”, “intends”, “projects”, “plans”, “estimates” or the negative of these words or other comparable terminology (as well as other words or expressions referencing future events, conditions or circumstances). Forward-looking statements are predictions, projections and other statements about future events that are based on current expectations and assumptions and, as a result, are subject to risks and uncertainties. These forward-looking statements include, but are not limited to, statements regarding the market size and potential growth opportunities of our current product candidates; the safety, efficacy, tolerability and other potential benefits, such as weight loss, associated with our current product candidates; the competitive differentiators of our current product candidates; potential collaborations and/or licensing partners for our current product candidates; our planned clinical trial activities for our current product candidates; the expected timeline for releasing topline data and other information about our product candidates; and our planned submissions of investigational new drug applications and meetings with the U.S. Food and Drug Administration. Many factors could cause actual future events to differ materially from the forward-looking statements in this Presentation, including, without limitation, those risks associated with our ability to execute our commercial strategy; the sufficiency of our existing cash on hand to fund our operations; the timeline for regulatory submissions, regulatory steps and potential regulatory approval of our current and future product candidates; the ability to realize the benefits of the license agreement with Dong-A ST Co., Ltd., including the impact on our future financial and operating results; the ability to integrate our current and future product candidates into our business in a timely and cost-efficient manner; the cooperation of our contract manufacturers, clinical study partners and others involved in the development of our current and future product candidates; our ability to initiate clinical trials on a timely basis; our planned clinical trials and our ability to recruit subjects for our clinical trials; the costs related to the license agreement, known and unknown, including costs of any litigation or regulatory actions relating to the license agreement; the changes in applicable laws or regulations; and the effects of changes to our stock price on the terms of the license agreement and any future fundraising. These forward-looking statements are based on information currently available to us and our current plans or expectations and are subject to a number of known and unknown uncertainties, risks and other important factors that may cause our actual results, performance or achievementsto differ materially from those expressed or implied by the forward-looking statements. This Presentation also may contain estimates and other statistical data made by independent parties and by us relating to market size and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. This Presentation speaks only as of the date of the information contained herein and the Company does not have any obligation to update or correct any information herein. |
| 3 Free Writing Prospectus The Company has filed a registration statement (including a prospectus) with the SEC for the offering to which this communication relates. The registration statement can be accessed here https://www.sec.gov/ix?doc=/Archives/edgar/data/1638287/000110465926000695/mtva-20250930xs1.htm. Before you invest, you should read the prospectus in that registration statement and other documents the Company has filed with the SEC for more complete information about the Company and this offering. You may get these documents for free by visiting EDGAR on the SEC website at www.sec.gov. Alternatively, we or any underwriter participating in the offering will arrange to send you the prospectus if you request it by calling Ladenburg Thalmann & Co. Inc. toll-free at 1-800-573-2541, by written request addressed to Syndicate Department, 640 5th Avenue, 4th Floor New York, NY 10019 or by e-mail: prospectus@ladenburg.com This Presentation shall not constitute an offer to sell, or the solicitation of an offer to buy, nor will there be any sale of these Securities in any state or other jurisdiction in which such offer, solicitation or sale would be unlawful. Neither the United States Securities and Exchange Commission nor any other regulatory body has approved or disapproved of our securities or passed upon the accuracy or adequacy of this Presentation. Any representation to the contrary is a criminal offense. |
| 4 Risk Factors Investing in our securities includes a high degree of risk. You should consider carefully the risk factors described in our Annual Report on Form 10-K for the year ended December 31, 2024, including specific factors discussed below, together with all of the other risk factors and information contained in our SEC filings. If any of the following risks actually occurs, our business, financial condition, results of operations and future prospects would likely be materially and adversely affected. This could cause the market price of our securities to decline and could cause you to lose all or part of your investment. Risks include but are not limited to: We have incurred net losses since inception, and we anticipate that we will continue to incur net losses for the foreseeable future. We require additional capital to accomplish our business plan and the failure to obtain necessary capital when needed on acceptable terms, or at all, could force us to delay, limit, reduce or terminate our operations. As we do no generate any revenue, we are dependent on working capital to fund our business plan, and raising additional capital may cause dilution to existing stockholders, restrict our operations or require us to relinquish rights to our technologies. Nasdaq may delist our common stock from its exchange, which could limit your ability to make transactionsin our securities and subject us to additional trading restrictions. Future sales, or the perception of future sales, by us or our securityholders could cause the market price of our common stock to decline. Adverse global economic conditions could have a material adverse effect on our business, results of operations and financial condition and liquidity. We may expend our limited resources to pursue a particular product candidate or indication and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success. Public opinion and scrutiny of treatments for obesity and overweight patients may impact public perception of our Company and DA-1726, or may adversely affect our ability to conduct our business and our business plans. We may be required to make significant payments under the 2022 License Agreement. Even if we obtain favorable clinical results, we may not be able to obtain regulatory approval for, or successfully commercialize Vanoglipel (DA-1241) and DA-1726. Preliminary, interim and topline data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changesin the final data. Results of earlier clinical trials may not be predictive of results of later-stage clinical trials. Product candidates may cause undesirable side effects that could delay or prevent their marketing approval, limit the commercial profile of an approved label, or result in significant negative consequences following marketing approval, if any, including marketing withdrawal. Our effortsto discover drug candidates beyond our current drug candidates may not succeed, and any drug candidates we recommend for clinical development may not actually begin clinical trials. Delays in our clinical trials may lead to a delay in the submission of marketing approval applications and jeopardize our ability to potentially receive approvals and generate revenues from the sale of our products. We may develop Vanoglipel (DA-1241) and DA-1726, and potentially future product candidates, in combination with other therapies, which exposes us to additional risks. Any collaboration arrangementthat we may enter into in the future may not be successful, which could adversely affect our ability to develop and commercialize our current and potential future drug candidates. Enrollment and retention of patients in clinical trials is an expensive and time-consuming process and could be made more difficult or rendered impossible by multiple factors outside our control, including difficulties in identifying patients with MASH and significant competition for recruiting such patientsin clinical trials. We face substantial competition, which may result in others discovering, developing or commercializing products before or more successfully than we do. We may engage in strategic transactionsthat could impact on our liquidity, increase our expenses and present significant distractionsto our management. Government shutdowns or inadequate funding of the FDA and other government agencies could hinder their ability to hire and retain key leadership and other personnel, prevent new products and services from being developed or commercialized in a timely manner or otherwise prevent those agencies from performing normal business functions on which the operation of our business may rely, which could negatively impact our business. We may engage in future acquisitions, mergers or in-licenses and out-licenses of technology that could disrupt our business, cause dilution to the organization’s stockholders and harm our financial condition and operating results. |

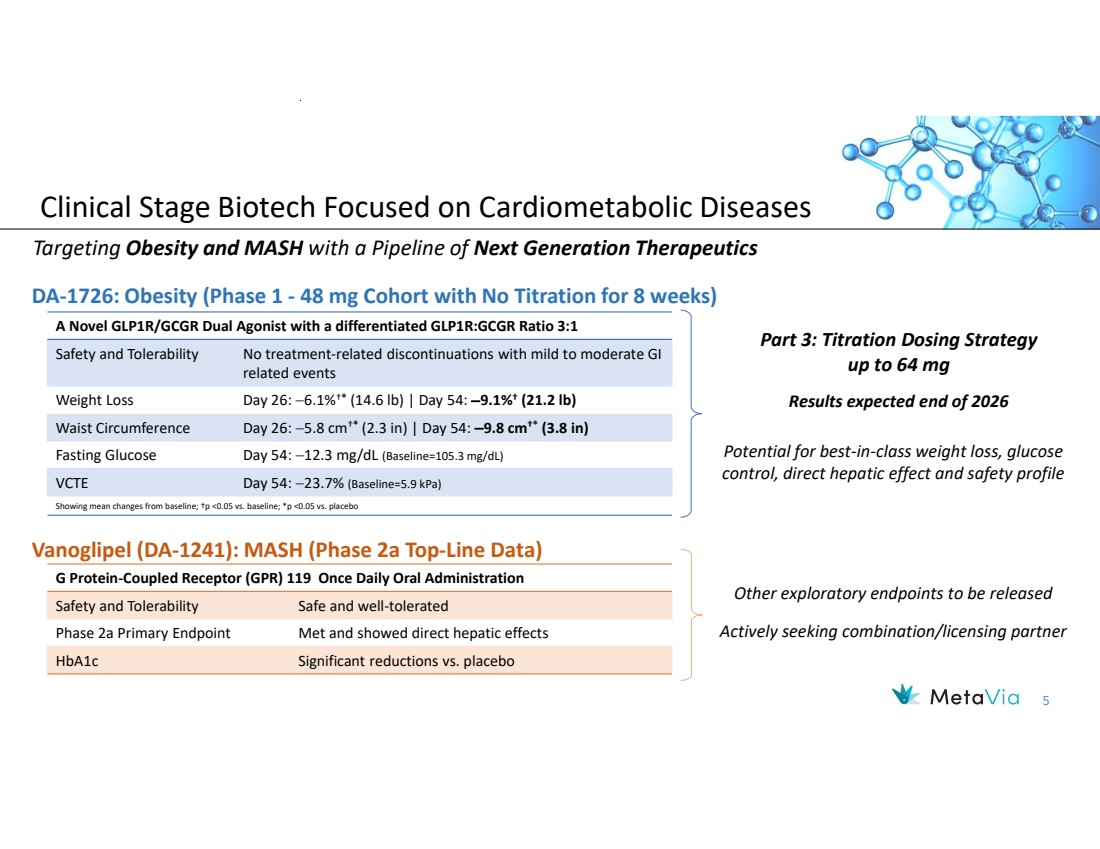
| 5 Clinical Stage Biotech Focused on Cardiometabolic Diseases Targeting Obesity and MASH with a Pipeline of Next Generation Therapeutics A Novel GLP1R/GCGR Dual Agonist with a differentiated GLP1R:GCGR Ratio 3:1 No treatment-related discontinuations with mild to moderate GI related events Safety and Tolerability Day 26: 6.1%†* (14.6 lb) | Day 54: 9.1%† Weight Loss (21.2 lb) Day 26: 5.8 cm†* (2.3 in) | Day 54: 9.8 cm†* Waist Circumference (3.8 in) Fasting Glucose Day 54: 12.3 mg/dL (Baseline=105.3 mg/dL) VCTE Day 54: 23.7% (Baseline=5.9 kPa) Showing mean changes from baseline; †p <0.05 vs. baseline; *p <0.05 vs. placebo DA-1726: Obesity (Phase 1 - 48 mg Cohort with No Titration for 8 weeks) Vanoglipel (DA-1241): MASH (Phase 2a Top-Line Data) G Protein-Coupled Receptor (GPR) 119 Once Daily Oral Administration Safety and Tolerability Safe and well-tolerated Phase 2a Primary Endpoint Met and showed direct hepatic effects HbA1c Significant reductions vs. placebo Other exploratory endpoints to be released Actively seeking combination/licensing partner Potential for best-in-class weight loss, glucose control, direct hepatic effect and safety profile Part 3: Titration Dosing Strategy up to 64 mg Results expected end of 2026 |
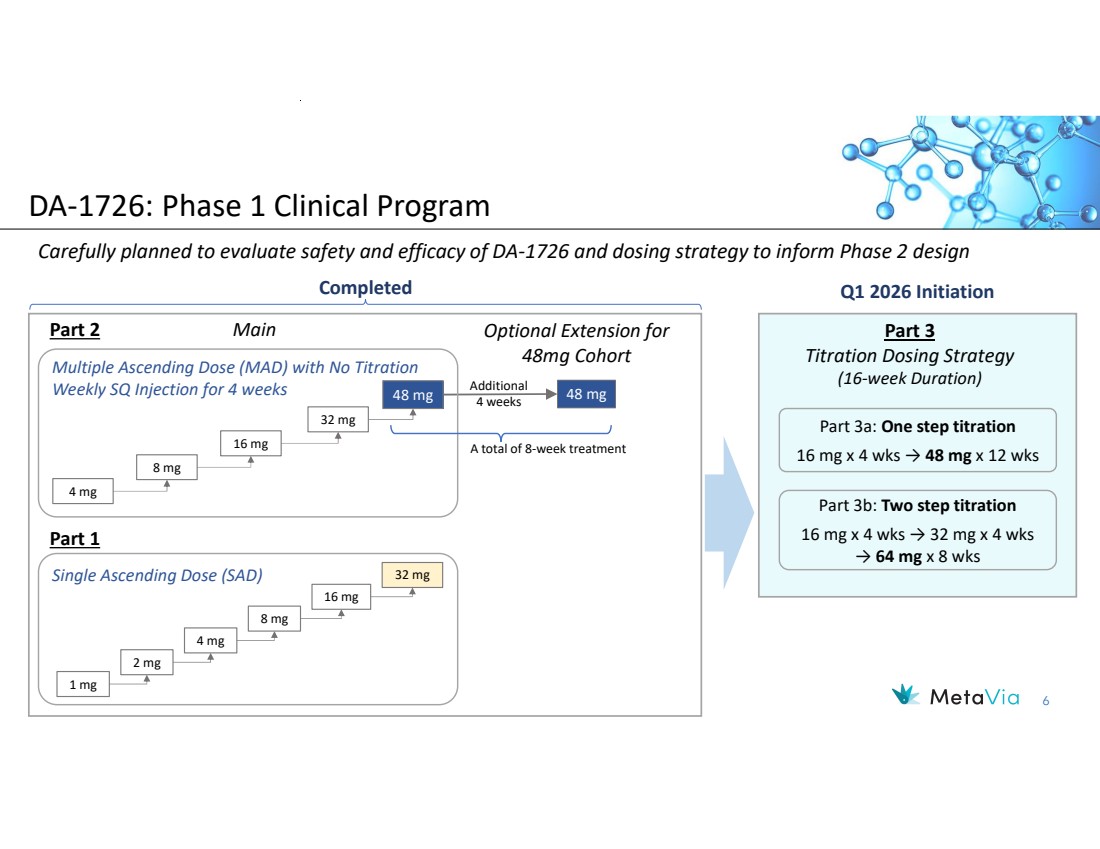
| 6 DA-1726: Phase 1 Clinical Program Carefully planned to evaluate safety and efficacy of DA-1726 and dosing strategy to inform Phase 2 design Main Optional Extension for 48mg Cohort Part 3 Titration Dosing Strategy (16-week Duration) 48 mg 48 mg Q1 2026 Initiation Additional 4 weeks 16 mg 4 mg 8 mg Multiple Ascending Dose (MAD) with No Titration Weekly SQ Injection for 4 weeks Single Ascending Dose (SAD) 32 mg 16 mg 1 mg 2 mg 4 mg 8 mg Completed 32 mg A total of 8-week treatment Part 2 Part 1 Part 3a: One step titration 16 mg x 4 wks → 48 mg x 12 wks Part 3b: Two step titration 16 mg x 4 wks → 32 mg x 4 wks → 64 mg x 8 wks |
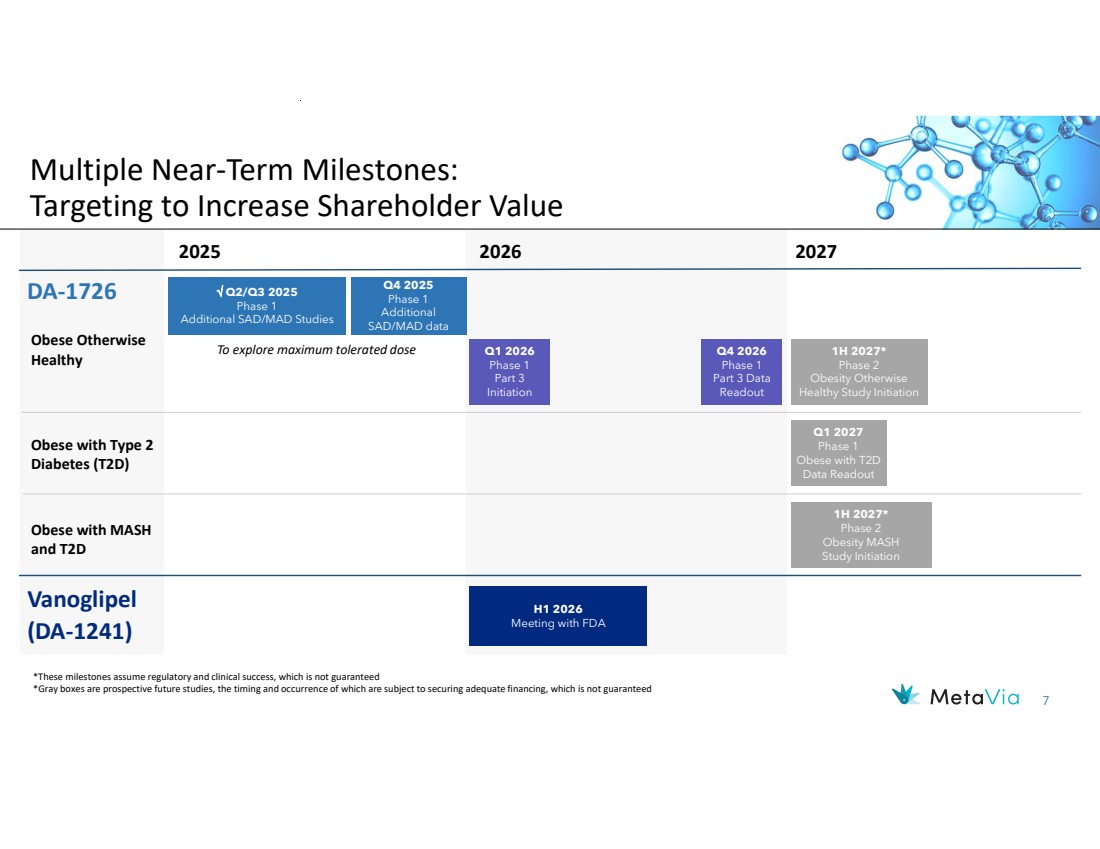
| 7 Multiple Near-Term Milestones: Targeting to Increase Shareholder Value 2026 Vanoglipel (DA-1241) H1 2026 Meeting with FDA DA-1726 *These milestones assume regulatory and clinical success, which is not guaranteed *Gray boxes are prospective future studies, the timing and occurrence of which are subject to securing adequate financing, which is not guaranteed Q2/Q3 2025 Phase 1 Additional SAD/MAD Studies Q2/Q3 2025 Phase 1 Additional SAD/MAD Studies Q4 2025 Phase 1 Additional SAD/MAD data To explore maximum tolerated dose 2025 Q1 2027 Phase 1 Obese with T2D Data Readout Obese Otherwise Healthy Obese with Type 2 Diabetes (T2D) 2027 Obese with MASH and T2D 1H 2027* Phase 2 Obesity MASH Study Initiation Q1 2026 Phase 1 Part 3 Initiation 1H 2027* Phase 2 Obesity Otherwise Healthy Study Initiation Q4 2026 Phase 1 Part 3 Data Readout |
| December 2023 NASDAQ: NRBO 8 DA -1726 A Novel GLP1R/GCGR Dual Agonist for the Treatment of Obesity |

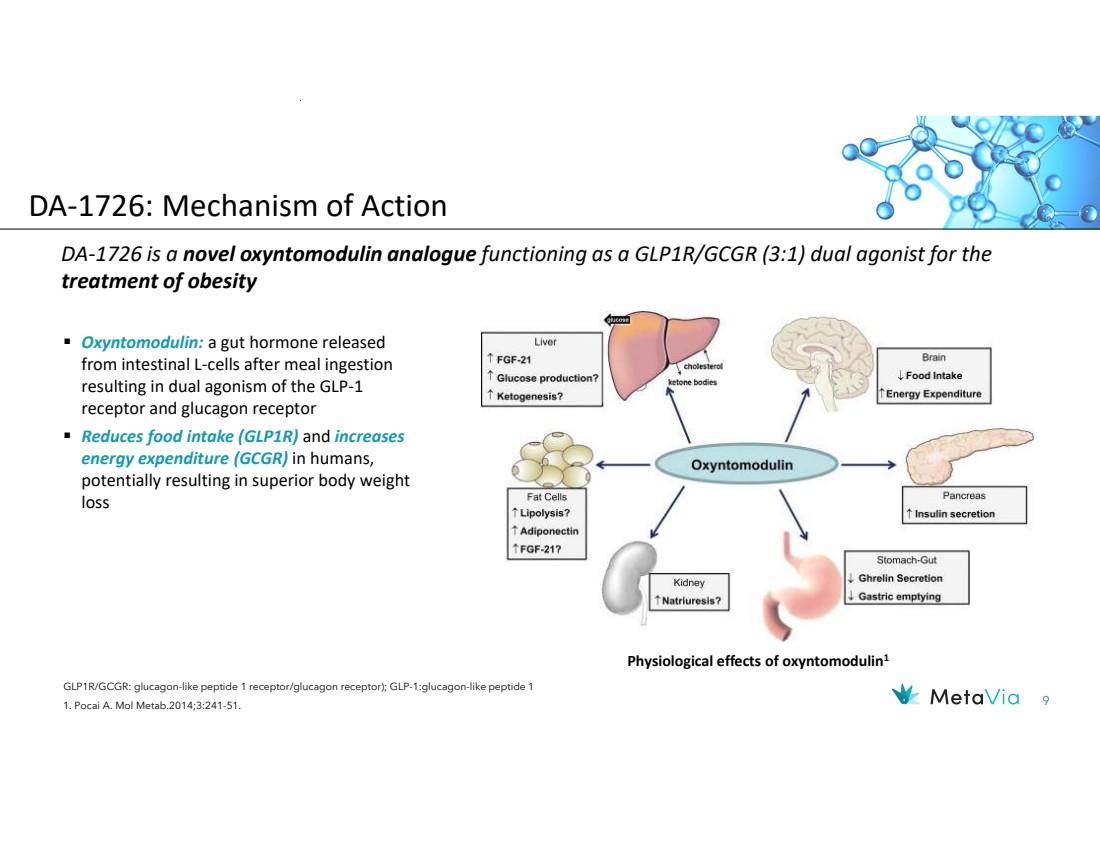
| 9 DA-1726 is a novel oxyntomodulin analogue functioning as a GLP1R/GCGR (3:1) dual agonist for the treatment of obesity GLP1R/GCGR: glucagon-like peptide 1 receptor/glucagon receptor); GLP-1:glucagon-like peptide 1 1. Pocai A. Mol Metab.2014;3:241-51. Oxyntomodulin: a gut hormone released from intestinal L-cells after meal ingestion resulting in dual agonism of the GLP-1 receptor and glucagon receptor Reduces food intake (GLP1R) and increases energy expenditure (GCGR) in humans, potentially resulting in superior body weight loss Physiological effects of oxyntomodulin1 DA-1726: Mechanism of Action |
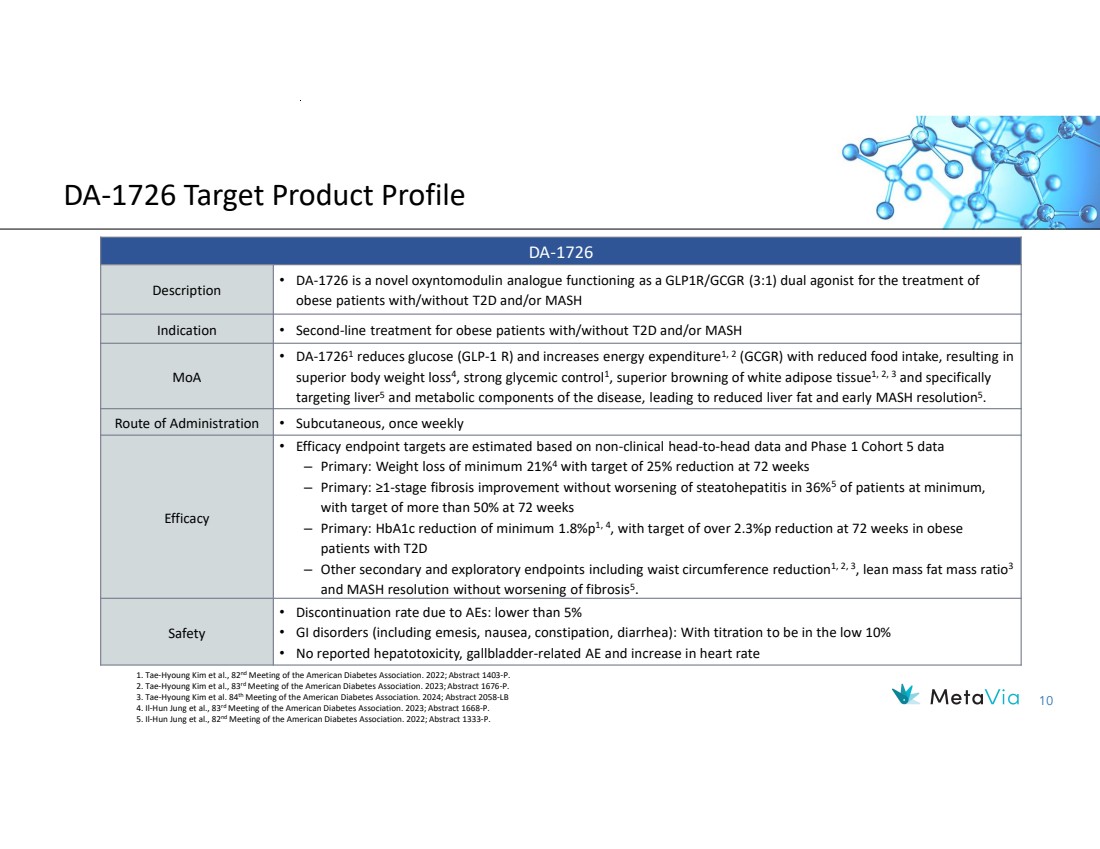
| 10 DA-1726 Target Product Profile DA-1726 • DA-1726 is a novel oxyntomodulin analogue functioning as a GLP1R/GCGR (3:1) dual agonist for the treatment of obese patients with/without T2D and/or MASH Description Indication • Second-line treatment for obese patients with/without T2D and/or MASH • DA-17261 reduces glucose (GLP-1 R) and increases energy expenditure1, 2 (GCGR) with reduced food intake, resulting in superior body weight loss4 , strong glycemic control1 , superior browning of white adipose tissue1, 2, 3 and specifically targeting liver5 and metabolic components of the disease, leading to reduced liver fat and early MASH resolution5 . MoA Route of Administration • Subcutaneous, once weekly • Efficacy endpoint targets are estimated based on non-clinical head-to-head data and Phase 1 Cohort 5 data – Primary: Weight loss of minimum 21%4 with target of 25% reduction at 72 weeks – Primary: ≥1-stage fibrosis improvement without worsening of steatohepatitis in 36%5 of patients at minimum, with target of more than 50% at 72 weeks – Primary: HbA1c reduction of minimum 1.8%p1, 4, with target of over 2.3%p reduction at 72 weeks in obese patients with T2D – Other secondary and exploratory endpoints including waist circumference reduction1, 2, 3, lean mass fat mass ratio3 and MASH resolution without worsening of fibrosis5 . Efficacy • Discontinuation rate due to AEs: lower than 5% • GI disorders (including emesis, nausea, constipation, diarrhea): With titration to be in the low 10% • No reported hepatotoxicity, gallbladder-related AE and increase in heart rate Safety 1. Tae-Hyoung Kim et al., 82nd Meeting of the American Diabetes Association. 2022; Abstract 1403-P. 2. Tae-Hyoung Kim et al., 83rd Meeting of the American Diabetes Association. 2023; Abstract 1676-P. 3. Tae-Hyoung Kim et al. 84th Meeting of the American Diabetes Association. 2024; Abstract 2058-LB 4. Il-Hun Jung et al., 83rd Meeting of the American Diabetes Association. 2023; Abstract 1668-P. 5. Il-Hun Jung et al., 82nd Meeting of the American Diabetes Association. 2022; Abstract 1333-P. |
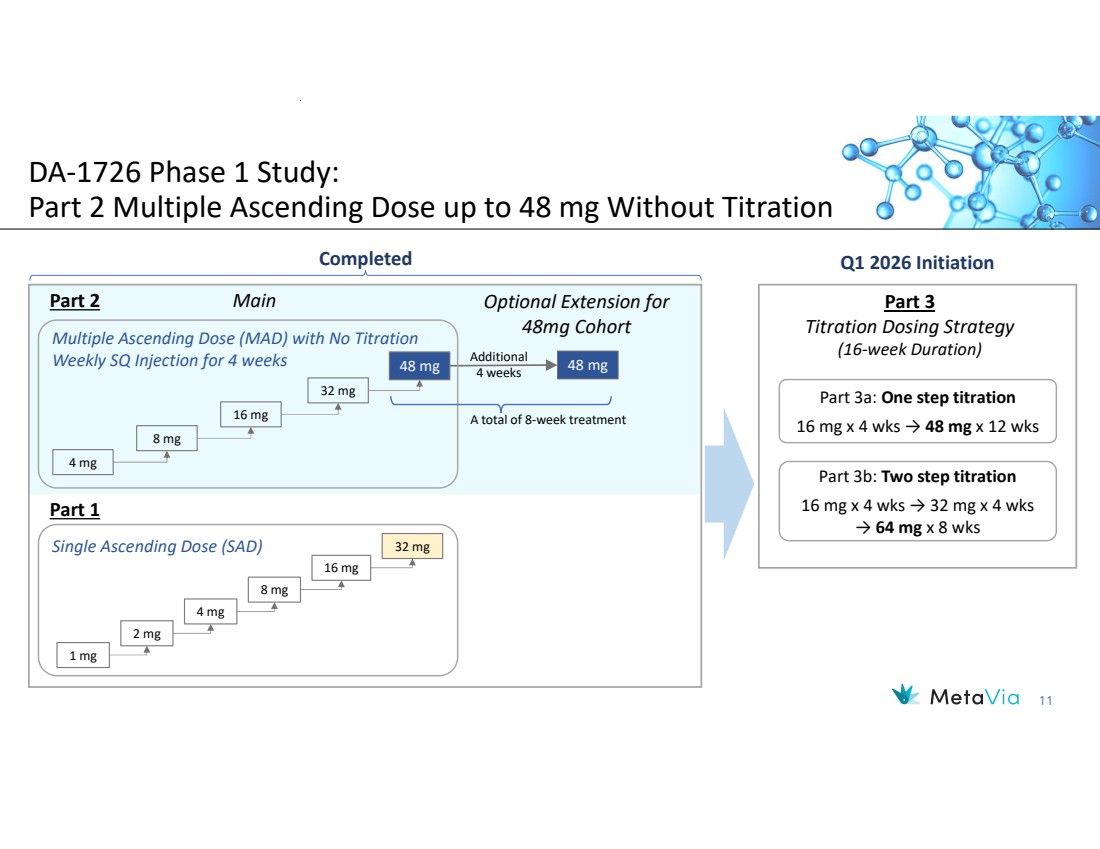
| 11 DA-1726 Phase 1 Study: Part 2 Multiple Ascending Dose up to 48 mg Without Titration Main Optional Extension for 48mg Cohort Part 3 Titration Dosing Strategy (16-week Duration) 48 mg 48 mg Q1 2026 Initiation Additional 4 weeks 16 mg 4 mg 8 mg Multiple Ascending Dose (MAD) with No Titration Weekly SQ Injection for 4 weeks Single Ascending Dose (SAD) 32 mg 16 mg 1 mg 2 mg 4 mg 8 mg Completed 32 mg A total of 8-week treatment Part 2 Part 1 Part 3a: One step titration 16 mg x 4 wks → 48 mg x 12 wks Part 3b: Two step titration 16 mg x 4 wks → 32 mg x 4 wks → 64 mg x 8 wks |
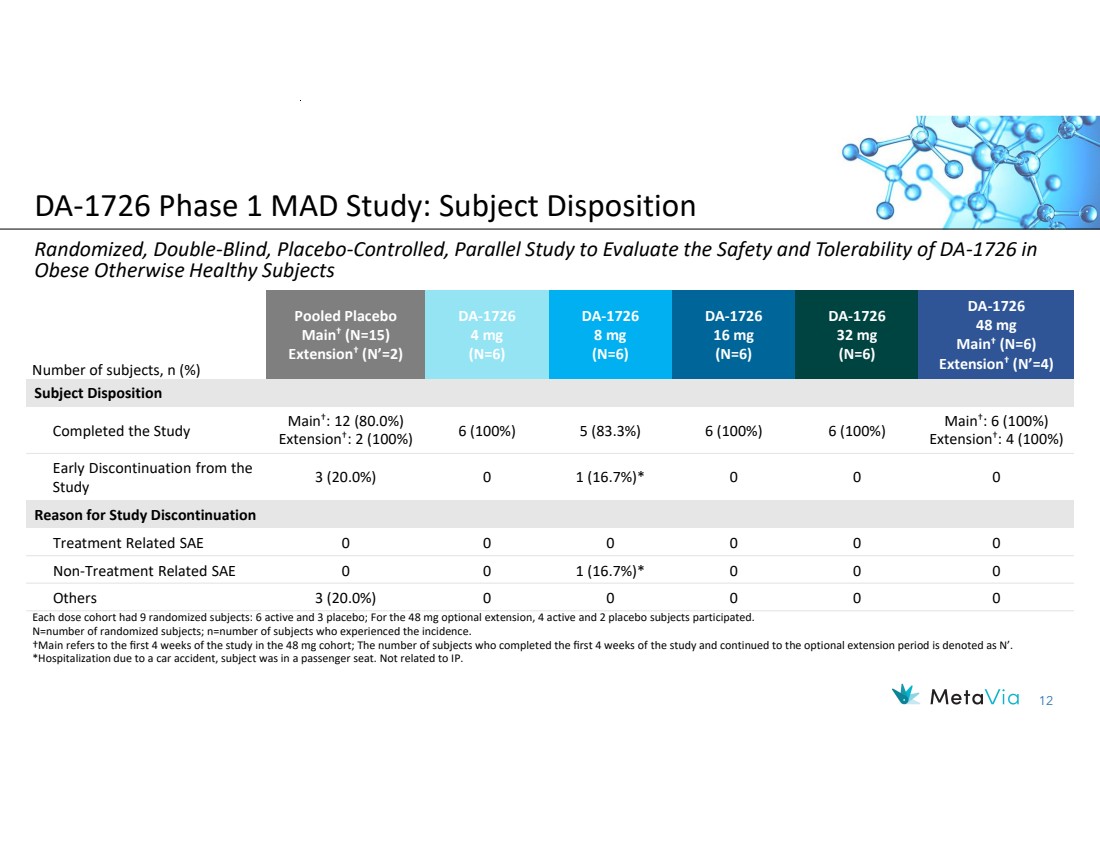
| 12 DA-1726 48 mg Main† (N=6) Extension† (N’=4) DA-1726 32 mg (N=6) DA-1726 16 mg (N=6) DA-1726 8 mg (N=6) DA-1726 4 mg (N=6) Pooled Placebo Main† (N=15) Extension† (N’=2) Number of subjects, n (%) Subject Disposition Main† : 6 (100%) Extension† : 4 (100%) 6 (100%) 5 (83.3%) 6 (100%) 6 (100%) Main† : 12 (80.0%) Extension† : 2 (100%) Completed the Study 3 (20.0%) 0 1 (16.7%)* 0 0 0 Early Discontinuation from the Study Reason for Study Discontinuation Treatment Related SAE 0 0 0 0 0 0 Non-Treatment Related SAE 0 0 1 (16.7%)* 0 0 0 Others 3 (20.0%) 0 0 0 0 0 Each dose cohort had 9 randomized subjects: 6 active and 3 placebo; For the 48 mg optional extension, 4 active and 2 placebo subjects participated. N=number of randomized subjects; n=number of subjects who experienced the incidence. †Main refers to the first 4 weeks of the study in the 48 mg cohort; The number of subjects who completed the first 4 weeks of the study and continued to the optional extension period is denoted as N’. *Hospitalization due to a car accident, subject was in a passenger seat. Not related to IP. Randomized, Double-Blind, Placebo-Controlled, Parallel Study to Evaluate the Safety and Tolerability of DA-1726 in Obese Otherwise Healthy Subjects DA-1726 Phase 1 MAD Study: Subject Disposition |
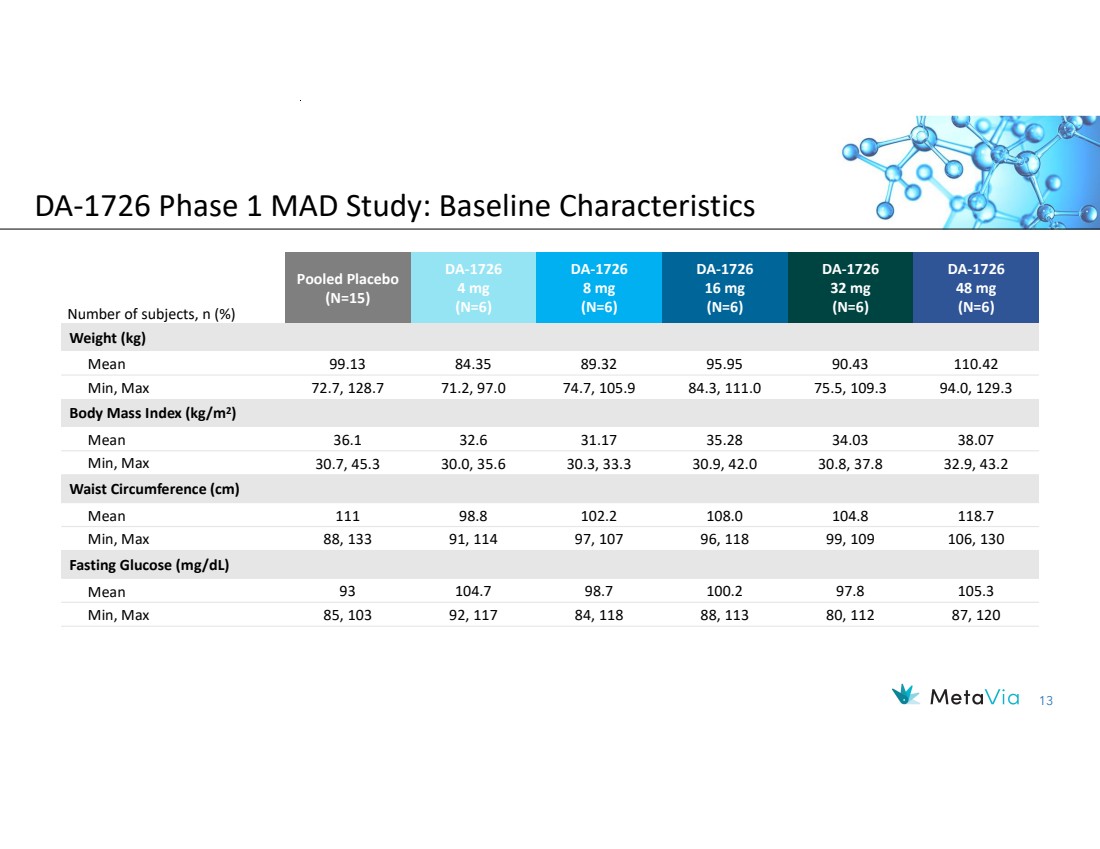
| 13 DA-1726 48 mg (N=6) DA-1726 32 mg (N=6) DA-1726 16 mg (N=6) DA-1726 8 mg (N=6) DA-1726 4 mg (N=6) Pooled Placebo (N=15) Number of subjects, n (%) Weight (kg) Mean 99.13 84.35 89.32 95.95 90.43 110.42 Min, Max 72.7, 128.7 71.2, 97.0 74.7, 105.9 84.3, 111.0 75.5, 109.3 94.0, 129.3 Body Mass Index (kg/m2 ) Mean 36.1 32.6 31.17 35.28 34.03 38.07 Min, Max 30.7, 45.3 30.0, 35.6 30.3, 33.3 30.9, 42.0 30.8, 37.8 32.9, 43.2 Waist Circumference (cm) Mean 111 98.8 102.2 108.0 104.8 118.7 Min, Max 88, 133 91, 114 97, 107 96, 118 99, 109 106, 130 Fasting Glucose (mg/dL) Mean 93 104.7 98.7 100.2 97.8 105.3 Min, Max 85, 103 92, 117 84, 118 88, 113 80, 112 87, 120 DA-1726 Phase 1 MAD Study: Baseline Characteristics |
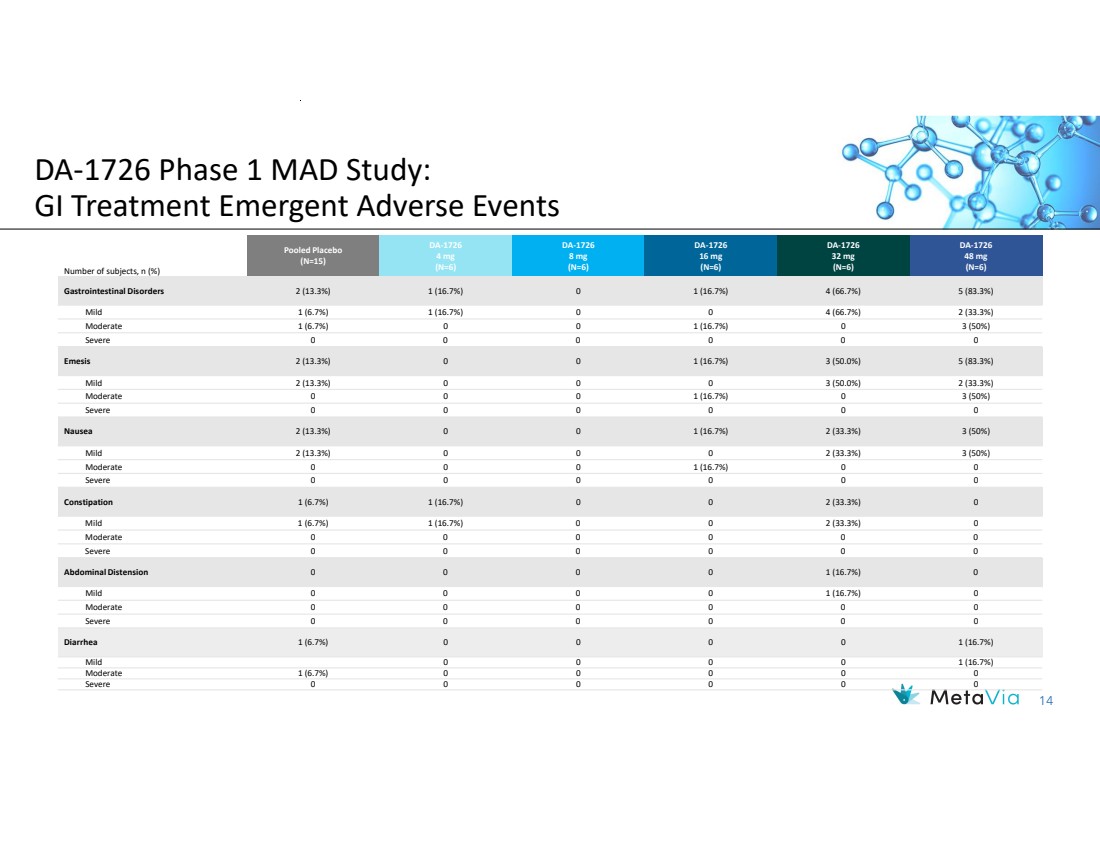
| 14 DA-1726 48 mg (N=6) DA-1726 32 mg (N=6) DA-1726 16 mg (N=6) DA-1726 8 mg (N=6) DA-1726 4 mg (N=6) Pooled Placebo (N=15) Number of subjects, n (%) Gastrointestinal Disorders 2 (13.3%) 1 (16.7%) 0 1 (16.7%) 4 (66.7%) 5 (83.3%) Mild 1 (6.7%) 1 (16.7%) 0 0 4 (66.7%) 2 (33.3%) Moderate 1 (6.7%) 0 0 1 (16.7%) 0 3 (50%) Severe 0 0 0 0 0 0 Emesis 2 (13.3%) 0 0 1 (16.7%) 3 (50.0%) 5 (83.3%) Mild 2 (13.3%) 0 0 0 3 (50.0%) 2 (33.3%) Moderate 0 0 0 1 (16.7%) 0 3 (50%) Severe 0 0 0 0 0 0 Nausea 2 (13.3%) 0 0 1 (16.7%) 2 (33.3%) 3 (50%) Mild 2 (13.3%) 0 0 0 2 (33.3%) 3 (50%) Moderate 0 0 0 1 (16.7%) 0 0 Severe 0 0 0 0 0 0 Constipation 1 (6.7%) 1 (16.7%) 0 0 2 (33.3%) 0 Mild 1 (6.7%) 1 (16.7%) 0 0 2 (33.3%) 0 Moderate 0 0 0 0 0 0 Severe 0 0 0 0 0 0 Abdominal Distension 0 0 0 0 1 (16.7%) 0 Mild 0 0 0 0 1 (16.7%) 0 Moderate 0 0 0 0 0 0 Severe 0 0 0 0 0 0 Diarrhea 1 (6.7%) 0 0 0 0 1 (16.7%) Mild 0 0 0 0 1 (16.7%) Moderate 1 (6.7%) 0 0 0 0 0 Severe 0 0 0 0 0 0 DA-1726 Phase 1 MAD Study: GI Treatment Emergent Adverse Events |
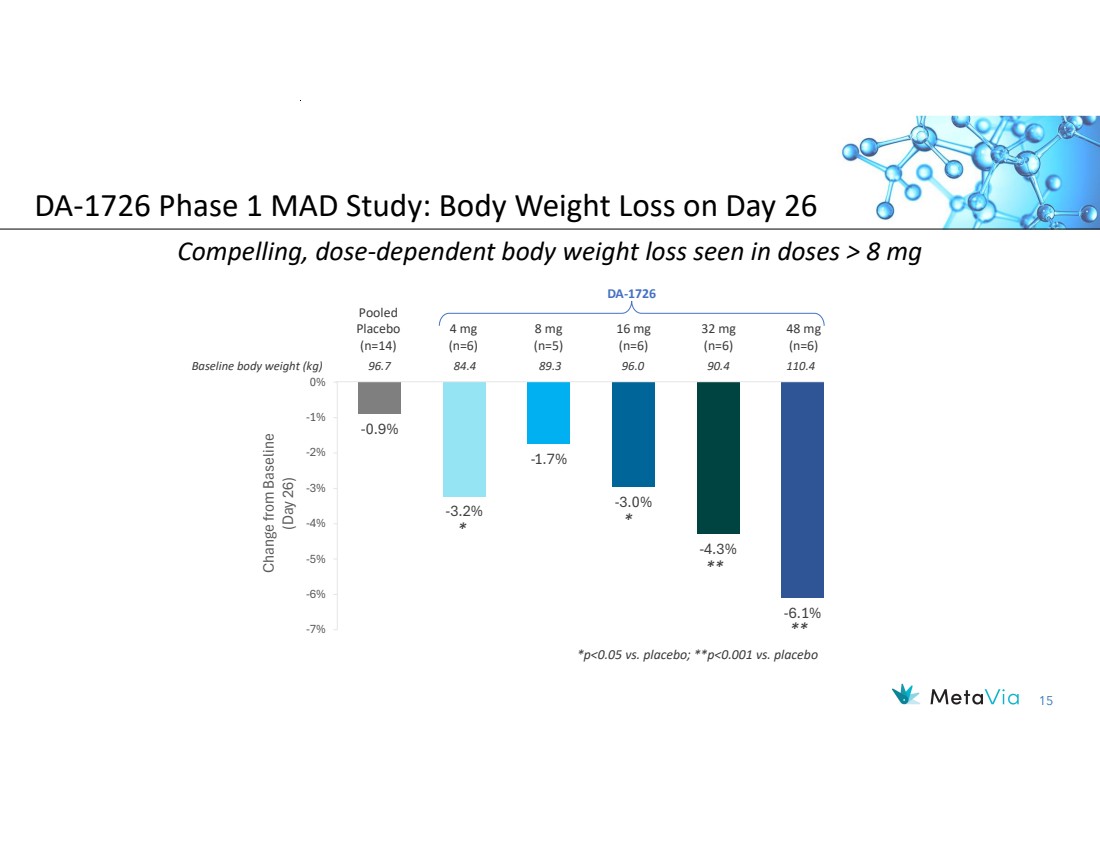
| 15 -0.9% -3.2% -1.7% -3.0% -4.3% -6.1% -7% -6% -5% -4% -3% -2% -1% 0% Change fro m Baseline (Day 2 6) Baseline body weight (kg) 96.7 84.4 89.3 96.0 90.4 110.4 Compelling, dose-dependent body weight loss seen in doses > 8 mg 48 mg (n=6) 32 mg (n=6) 16 mg (n=6) 8 mg (n=5) 4 mg (n=6) Pooled Placebo (n=14) DA-1726 * * ** ** DA-1726 Phase 1 MAD Study: Body Weight Loss on Day 26 *p<0.05 vs. placebo; **p<0.001 vs. placebo |
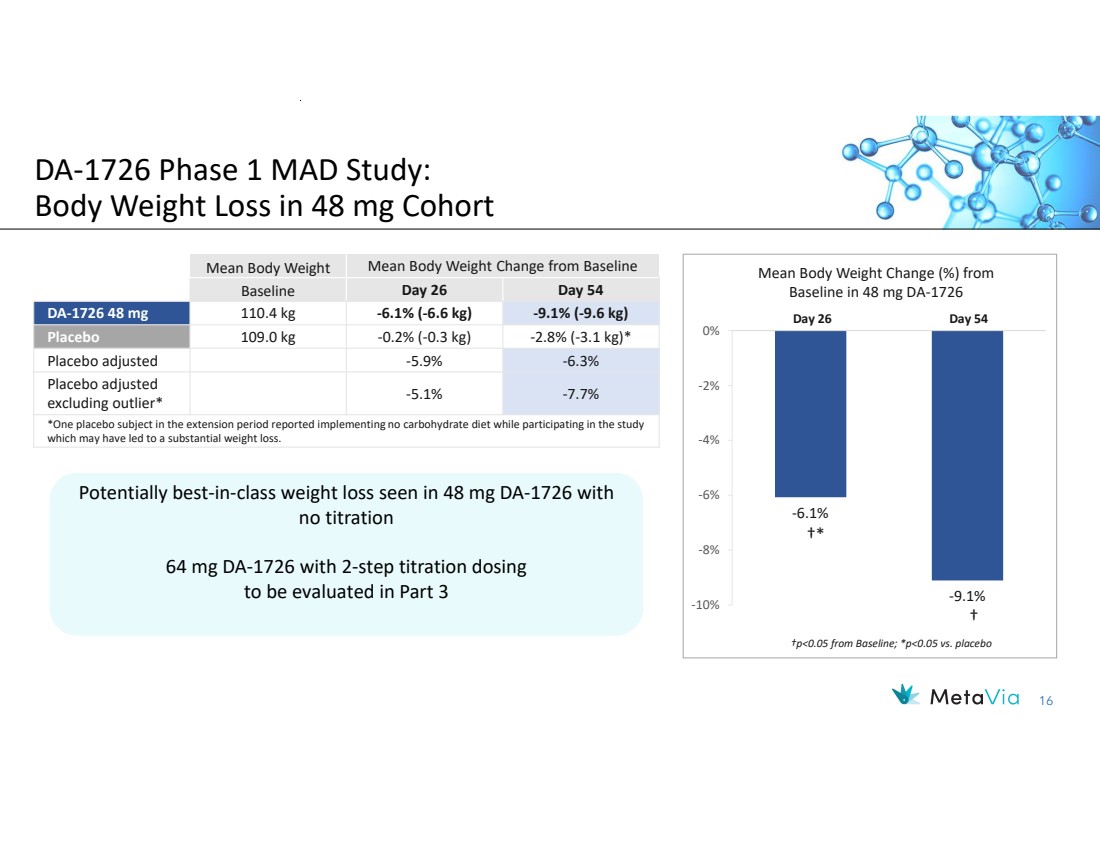
| 16 Mean Body Weight Mean Body Weight Change from Baseline Baseline Day 26 Day 54 DA-1726 48 mg 110.4 kg -6.1% (-6.6 kg) -9.1% (-9.6 kg) Placebo 109.0 kg -0.2% (-0.3 kg) -2.8% (-3.1 kg)* Placebo adjusted -5.9% -6.3% -5.1% -7.7% Placebo adjusted excluding outlier* *One placebo subject in the extension period reported implementing no carbohydrate diet while participating in the study which may have led to a substantial weight loss. Potentially best-in-class weight loss seen in 48 mg DA-1726 with no titration 64 mg DA-1726 with 2-step titration dosing to be evaluated in Part 3 Potentially best-in-class weight loss seen in 48 mg DA-1726 with no titration 64 mg DA-1726 with 2-step titration dosing to be evaluated in Part 3 DA-1726 Phase 1 MAD Study: Body Weight Loss in 48 mg Cohort -6.1% -9.1% -10% -8% -6% -4% -2% 0% Mean Body Weight Change (%) from Baseline in 48 mg DA-1726 †p<0.05 from Baseline; *p<0.05 vs. placebo †* † Day 26 Day 54 |
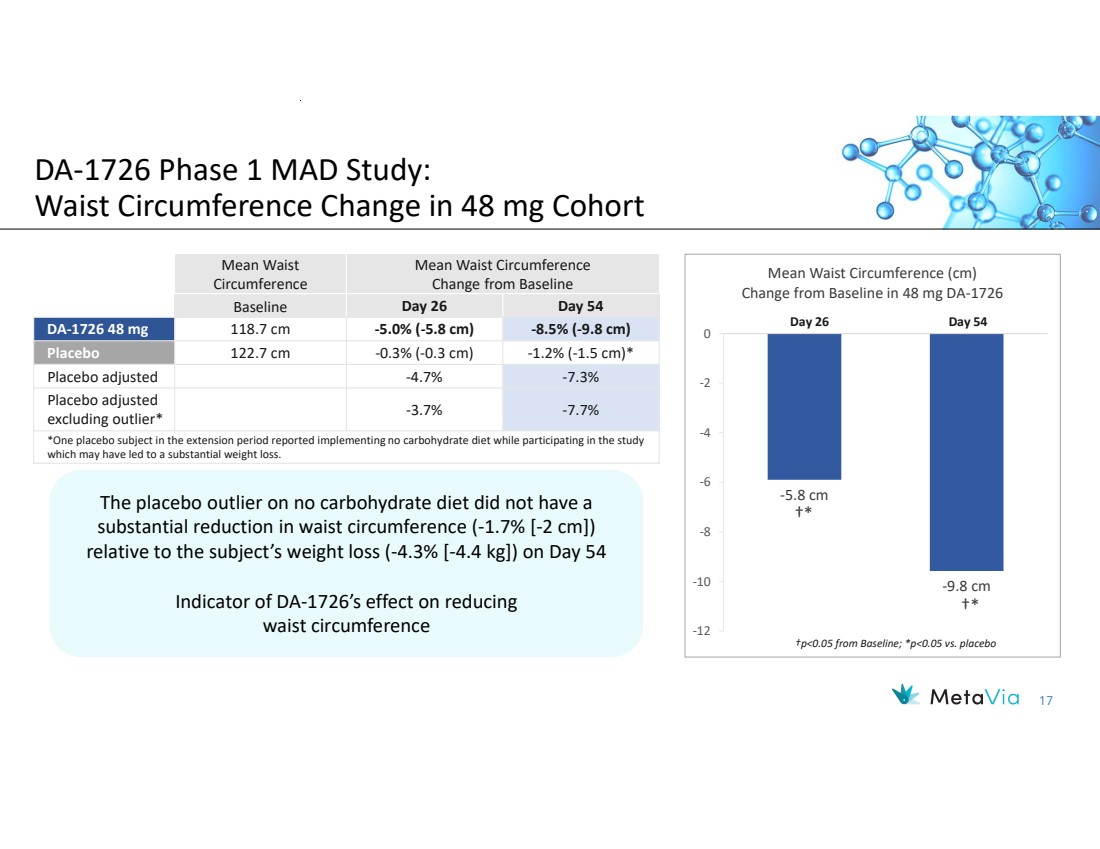
| 17 -5.8 cm -9.8 cm -12 -10 -8 -6 -4 -2 0 Mean Waist Circumference (cm) Change from Baseline in 48 mg DA-1726 †* †* Day 26 Day 54 †p<0.05 from Baseline; *p<0.05 vs. placebo Mean Waist Circumference Change from Baseline Mean Waist Circumference Baseline Day 26 Day 54 DA-1726 48 mg 118.7 cm -5.0% (-5.8 cm) -8.5% (-9.8 cm) Placebo 122.7 cm -0.3% (-0.3 cm) -1.2% (-1.5 cm)* Placebo adjusted -4.7% -7.3% -3.7% -7.7% Placebo adjusted excluding outlier* *One placebo subject in the extension period reported implementing no carbohydrate diet while participating in the study which may have led to a substantial weight loss. DA-1726 Phase 1 MAD Study: Waist Circumference Change in 48 mg Cohort The placebo outlier on no carbohydrate diet did not have a substantial reduction in waist circumference (-1.7% [-2 cm]) relative to the subject’s weight loss (-4.3% [-4.4 kg]) on Day 54 Indicator of DA-1726’s effect on reducing waist circumference The placebo outlier on no carbohydrate diet did not have a substantial reduction in waist circumference (-1.7% [-2 cm]) relative to the subject’s weight loss (-4.3% [-4.4 kg]) on Day 54 Indicator of DA-1726’s effect on reducing waist circumference |
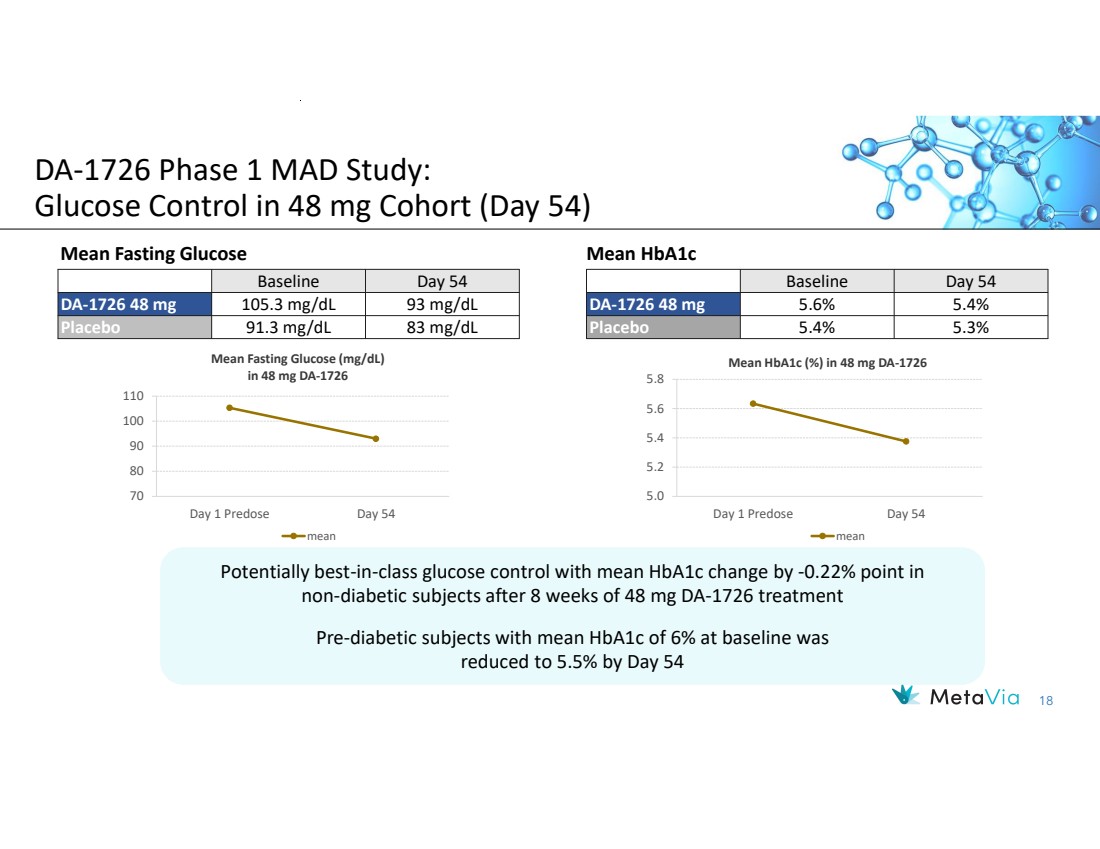
| 18 Baseline Day 54 DA-1726 48 mg 105.3 mg/dL 93 mg/dL Placebo 91.3 mg/dL 83 mg/dL 70 80 90 100 110 Day 1 Predose Day 54 Mean Fasting Glucose (mg/dL) in 48 mg DA-1726 mean Mean Fasting Glucose Baseline Day 54 DA-1726 48 mg 5.6% 5.4% Placebo 5.4% 5.3% Mean HbA1c 5.0 5.2 5.4 5.6 5.8 Day 1 Predose Day 54 Mean HbA1c (%) in 48 mg DA-1726 mean DA-1726 Phase 1 MAD Study: Glucose Control in 48 mg Cohort (Day 54) Potentially best-in-class glucose control with mean HbA1c change by -0.22% point in non-diabetic subjects after 8 weeks of 48 mg DA-1726 treatment Pre-diabetic subjects with mean HbA1c of 6% at baseline was reduced to 5.5% by Day 54 Potentially best-in-class glucose control with mean HbA1c change by -0.22% point in non-diabetic subjects after 8 weeks of 48 mg DA-1726 treatment Pre-diabetic subjects with mean HbA1c of 6% at baseline was reduced to 5.5% by Day 54 |
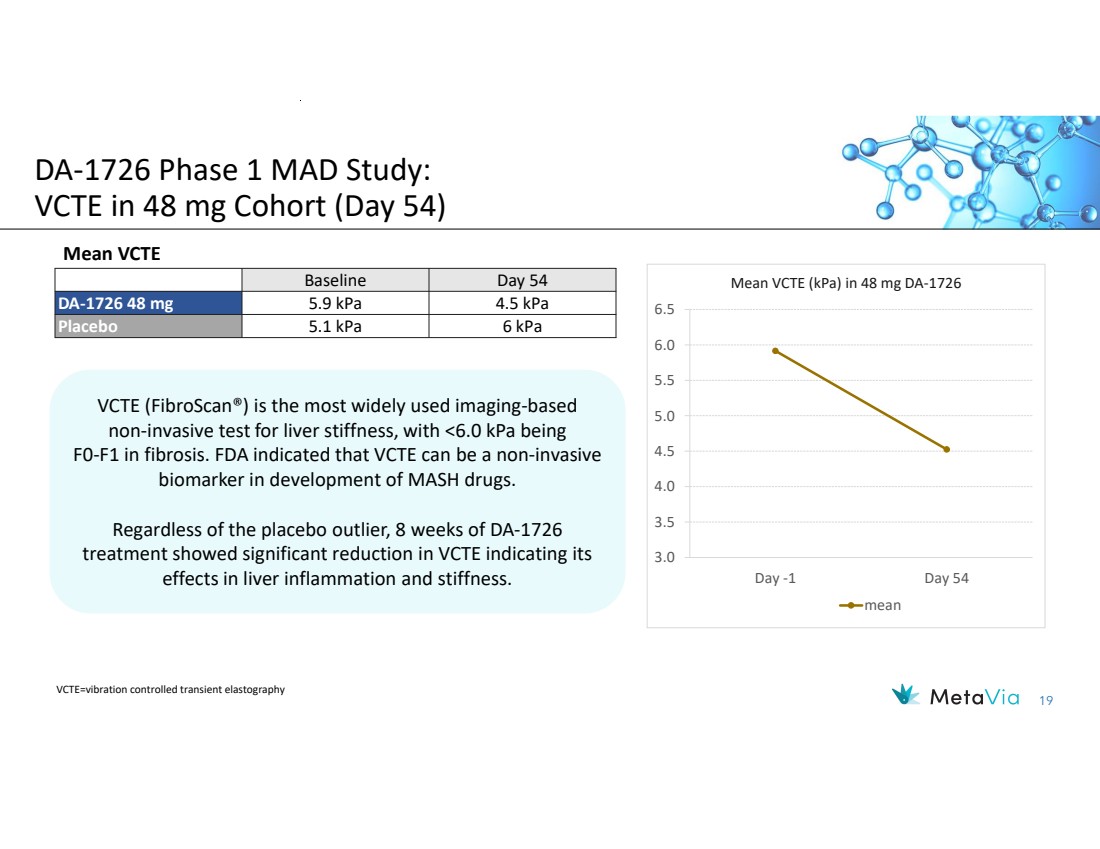
| 19 Baseline Day 54 DA-1726 48 mg 5.9 kPa 4.5 kPa Placebo 5.1 kPa 6 kPa 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5 Day -1 Day 54 Mean VCTE (kPa) in 48 mg DA-1726 mean DA-1726 Phase 1 MAD Study: VCTE in 48 mg Cohort (Day 54) Mean VCTE VCTE=vibration controlled transient elastography VCTE (FibroScan®) is the most widely used imaging-based non-invasive test for liver stiffness, with <6.0 kPa being F0-F1 in fibrosis. FDA indicated that VCTE can be a non-invasive biomarker in development of MASH drugs. Regardless of the placebo outlier, 8 weeks of DA-1726 treatment showed significant reduction in VCTE indicating its effects in liver inflammation and stiffness. VCTE (FibroScan®) is the most widely used imaging-based non-invasive test for liver stiffness, with <6.0 kPa being F0-F1 in fibrosis. FDA indicated that VCTE can be a non-invasive biomarker in development of MASH drugs. Regardless of the placebo outlier, 8 weeks of DA-1726 treatment showed significant reduction in VCTE indicating its effects in liver inflammation and stiffness. |
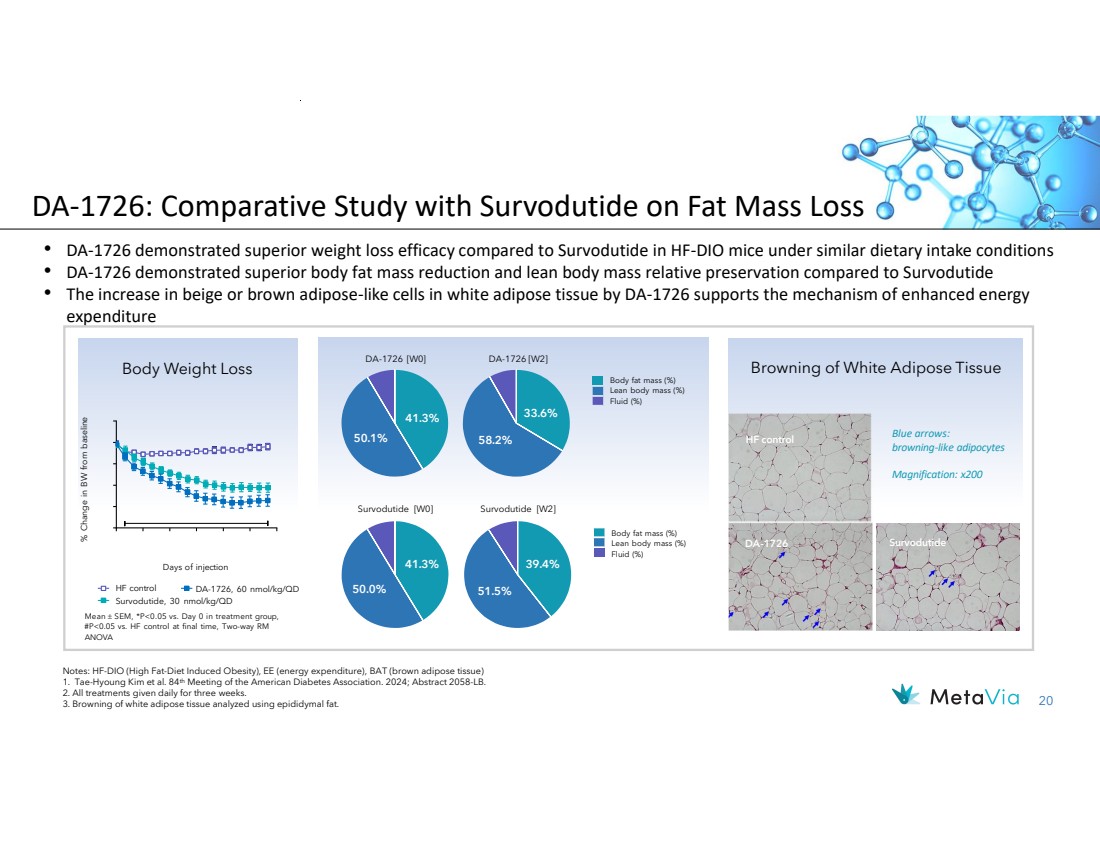
| 20 DA-1726: Comparative Study with Survodutide on Fat Mass Loss • DA-1726 demonstrated superior weight loss efficacy compared to Survodutide in HF-DIO mice under similar dietary intake conditions • DA-1726 demonstrated superior body fat mass reduction and lean body mass relative preservation compared to Survodutide • The increase in beige or brown adipose-like cells in white adipose tissue by DA-1726 supports the mechanism of enhanced energy expenditure Browning of White Adipose Tissue 41.3% 50.1% Survodutide [W0] 41.3% 50.0% 33.6% 58.2% Body fat mass (%) Lean body mass (%) Fluid (%) Survodutide [W2] 39.4% 51.5% Body fat mass (%) Lean body mass (%) Fluid (%) DA-1726 Survodutide HF control Blue arrows: browning-like adipocytes Magnification: x200 HF control Survodutide, 30 nmol/kg/QD DA-1726, 60 nmol/kg/QD Days of injection % Change in BW from baseline Body Weight Loss DA-1726 [W0] DA-1726 [W2] Notes: HF-DIO (High Fat-Diet Induced Obesity), EE (energy expenditure), BAT (brown adipose tissue) 1. Tae-Hyoung Kim et al. 84th Meeting of the American Diabetes Association. 2024; Abstract 2058-LB. 2. All treatments given daily for three weeks. 3. Browning of white adipose tissue analyzed using epididymal fat. Mean SEM, *P<0.05 vs. Day 0 in treatment group, #P<0.05 vs. HF control at final time, Two-way RM ANOVA |
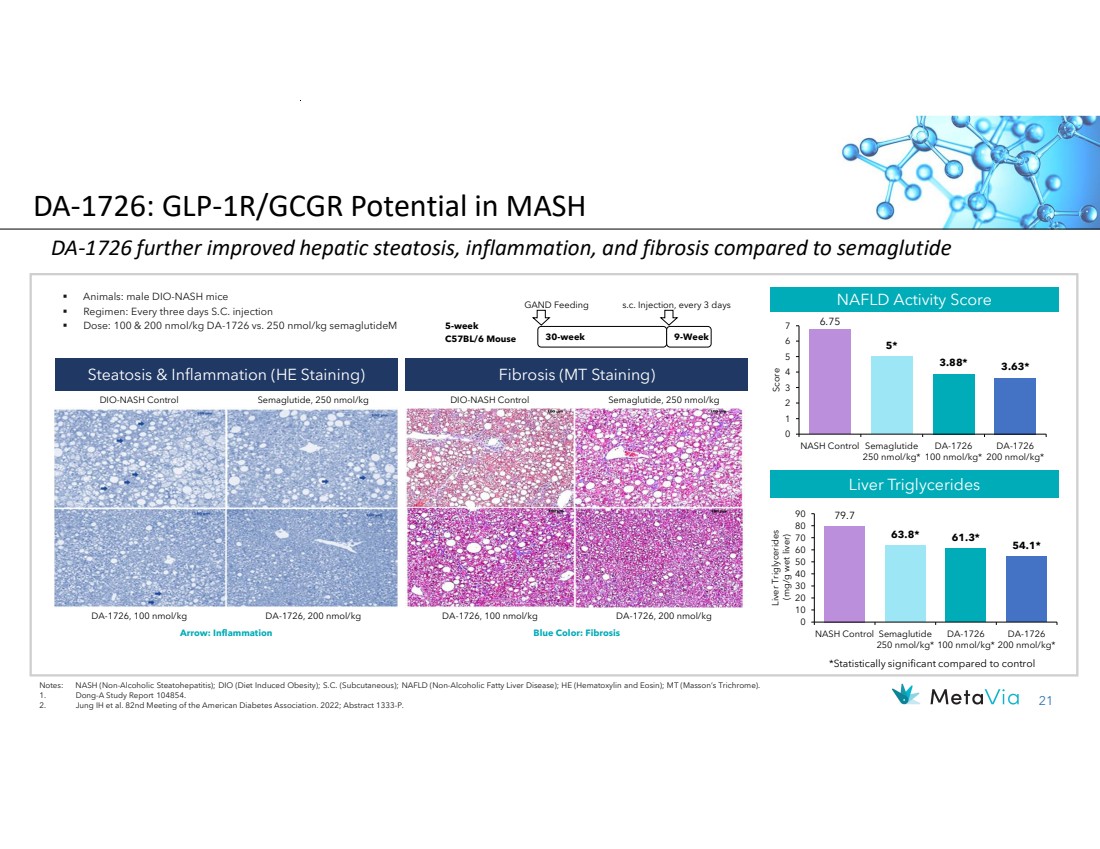
| 21 6.75 5* 3.88* 3.63* 0 1 2 3 4 5 6 7 NASH Control Semaglutide 250 nmol/kg* DA-1726 100 nmol/kg* DA-1726 200 nmol/kg* Score DA-1726 further improved hepatic steatosis, inflammation, and fibrosis compared to semaglutide Animals: male DIO-NASH mice Regimen: Every three days S.C. injection Dose: 100 & 200 nmol/kg DA-1726 vs. 250 nmol/kg semaglutideM Steatosis & Inflammation (HE Staining) DA-1726, 100 nmol/kg Notes: NASH (Non-Alcoholic Steatohepatitis); DIO (Diet Induced Obesity); S.C. (Subcutaneous); NAFLD (Non-Alcoholic Fatty Liver Disease); HE (Hematoxylin and Eosin); MT (Masson’s Trichrome). 1. Dong-A Study Report 104854. 2. Jung IH et al. 82nd Meeting of the American Diabetes Association. 2022; Abstract 1333-P. 30-week GAND Feeding s.c. Injection, every 3 days 5-week C57BL/6 Mouse 9-Week NAFLD Activity Score Fibrosis (MT Staining) DA-1726, 200 nmol/kg DIO-NASH Control Semaglutide, 250 nmol/kg DIO-NASH Control Semaglutide, 250 nmol/kg DA-1726, 100 nmol/kg DA-1726, 200 nmol/kg Liver Triglycerides Arrow: Inflammation Blue Color: Fibrosis 79.7 63.8* 61.3* 54.1* 0 10 20 30 40 50 60 70 80 90 NASH Control Semaglutide 250 nmol/kg* DA-1726 100 nmol/kg* DA-1726 200 nmol/kg* Liver Triglycerides (mg/g wet liver) *Statistically significant compared to control DA-1726: GLP-1R/GCGR Potential in MASH |
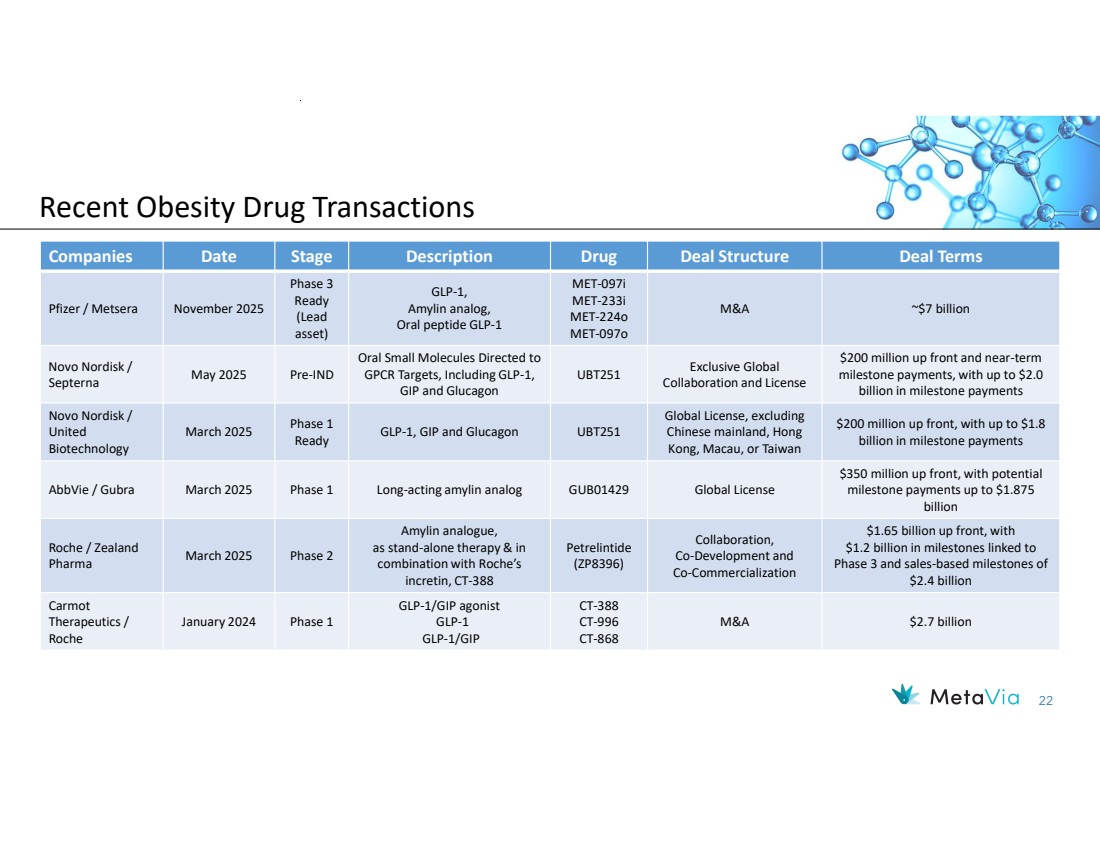
| 22 Recent Obesity Drug Transactions Companies Date Stage Description Drug Deal Structure Deal Terms M&A ~$7 billion MET-097i MET-233i MET-224o MET-097o GLP-1, Amylin analog, Oral peptide GLP-1 Phase 3 Ready (Lead asset) Pfizer / Metsera November 2025 $200 million up front and near-term milestone payments, with up to $2.0 billion in milestone payments Exclusive Global Collaboration and License UBT251 Oral Small Molecules Directed to GPCR Targets, Including GLP-1, GIP and Glucagon May 2025 Pre-IND Novo Nordisk / Septerna $200 million up front, with up to $1.8 billion in milestone payments Global License, excluding Chinese mainland, Hong Kong, Macau, or Taiwan GLP-1, GIP and Glucagon UBT251 Phase 1 Ready March 2025 Novo Nordisk / United Biotechnology $350 million up front, with potential milestone payments up to $1.875 billion AbbVie / Gubra March 2025 Phase 1 Long-acting amylin analog GUB01429 Global License $1.65 billion up front, with $1.2 billion in milestones linked to Phase 3 and sales-based milestones of $2.4 billion Collaboration, Co-Development and Co-Commercialization Petrelintide (ZP8396) Amylin analogue, as stand-alone therapy & in combination with Roche’s incretin, CT-388 March 2025 Phase 2 Roche / Zealand Pharma M&A $2.7 billion CT-388 CT-996 CT-868 GLP-1/GIP agonist GLP-1 GLP-1/GIP January 2024 Phase 1 Carmot Therapeutics / Roche |
| December 2023 NASDAQ: NRBO 23 Vanoglipel (D A -1241) Orally Available, Potential Firs t -in -Class GPR119 Agonist for the Treatment of Metabolic Dysfunction -associated Steatohepatitis (MASH) |

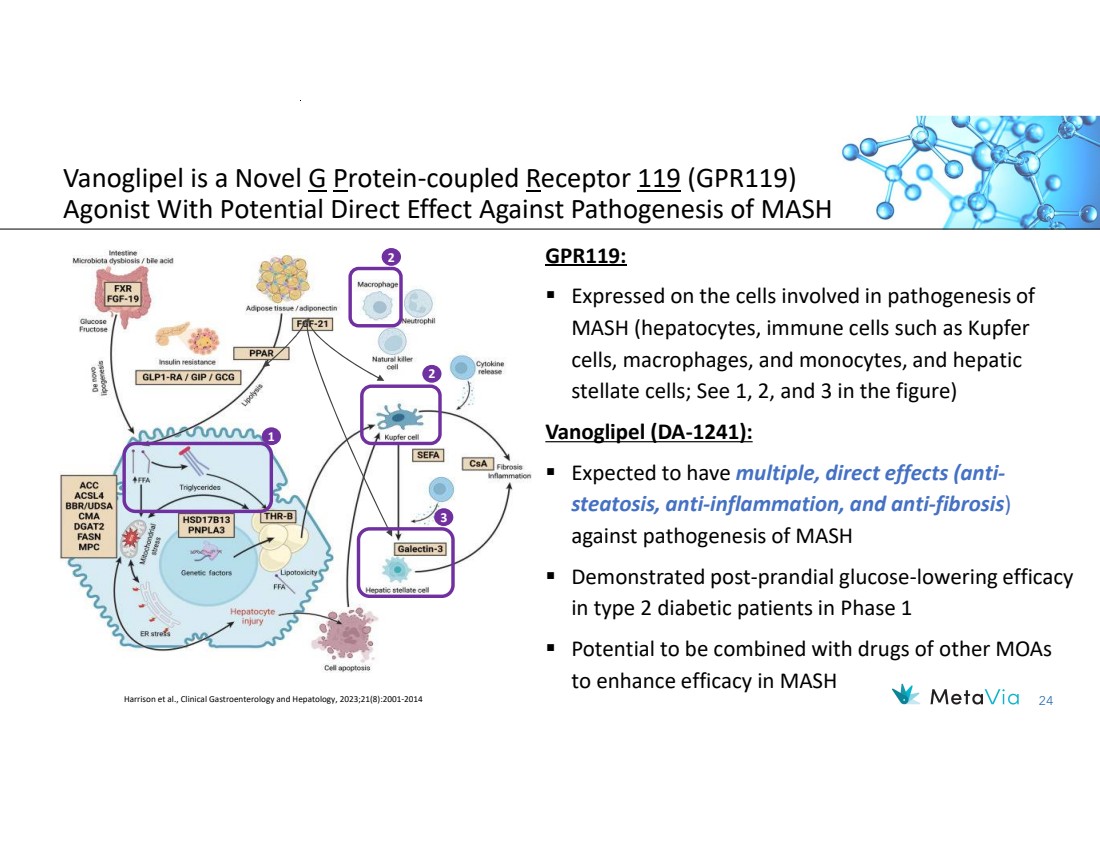
| 24 GPR119: Expressed on the cells involved in pathogenesis of MASH (hepatocytes, immune cells such as Kupfer cells, macrophages, and monocytes, and hepatic stellate cells; See 1, 2, and 3 in the figure) Vanoglipel (DA-1241): Expected to have multiple, direct effects (anti-steatosis, anti-inflammation, and anti-fibrosis) against pathogenesis of MASH Demonstrated post-prandial glucose-lowering efficacy in type 2 diabetic patients in Phase 1 Potential to be combined with drugs of other MOAs to enhance efficacy in MASH Vanoglipel is a Novel G Protein-coupled Receptor 119 (GPR119) Agonist With Potential Direct Effect Against Pathogenesis of MASH 1 2 2 3 Harrison et al., Clinical Gastroenterology and Hepatology, 2023;21(8):2001-2014 |
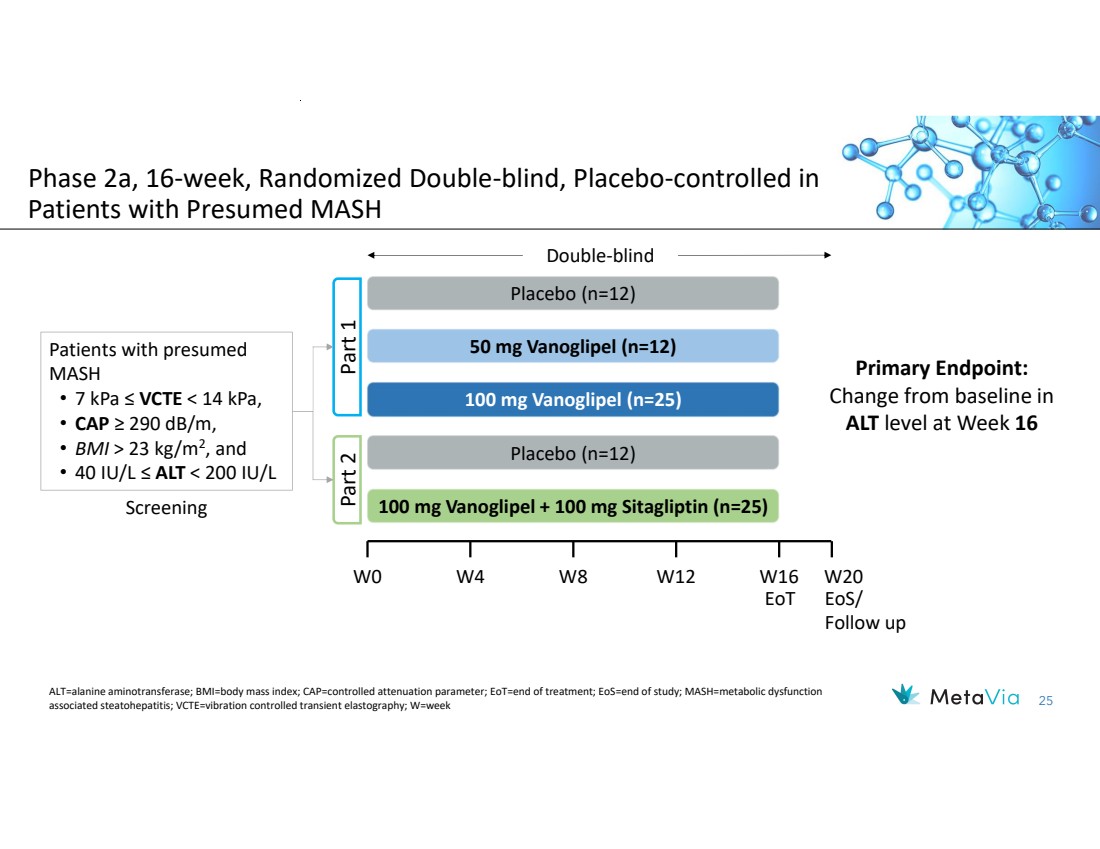
| 25 Phase 2a, 16-week, Randomized Double-blind, Placebo-controlled in Patients with Presumed MASH Primary Endpoint: Change from baseline in ALT level at Week 16 50 mg Vanoglipel (n=12) 100 mg Vanoglipel (n=25) Placebo (n=12) P art 1 Placebo (n=12) P 100 mg Vanoglipel + 100 mg Sitagliptin (n=25) art 2 Patients with presumed MASH • 7 kPa ≤ VCTE < 14 kPa, • CAP ≥ 290 dB/m, • BMI > 23 kg/m2 , and • 40 IU/L ≤ ALT < 200 IU/L Double-blind Screening W0 W4 W8 W12 W16 W20 EoT EoS/ Follow up ALT=alanine aminotransferase; BMI=body mass index; CAP=controlled attenuation parameter; EoT=end of treatment; EoS=end of study; MASH=metabolic dysfunction associated steatohepatitis; VCTE=vibration controlled transient elastography; W=week |
| 26 Vanoglipel (DA-1241) Demonstrated Both Hepatoprotective and Glucose-regulating Effects in Patients with Presumed MASH significantly decreased plasma ALT levels, with a mean reduction of 22.8 U/L after 16 week-treatment improved systemic inflammatory and fibrosis biomarkers, suggesting beneficial effects on liver health efficiently improved glucose control in patients with comorbidity of type 2 diabetes was well-tolerated in presumed MASH patients, with no TEAE leading to IP discontinuation in any treatment groups except one in the PBO group had a similar safety profile of the combination arm compared to placebo, indicating combinability of vanoglipel with other drugs In a 16-week, randomized double-blind, placebo-controlled Phase 2a study, vanoglipel: |
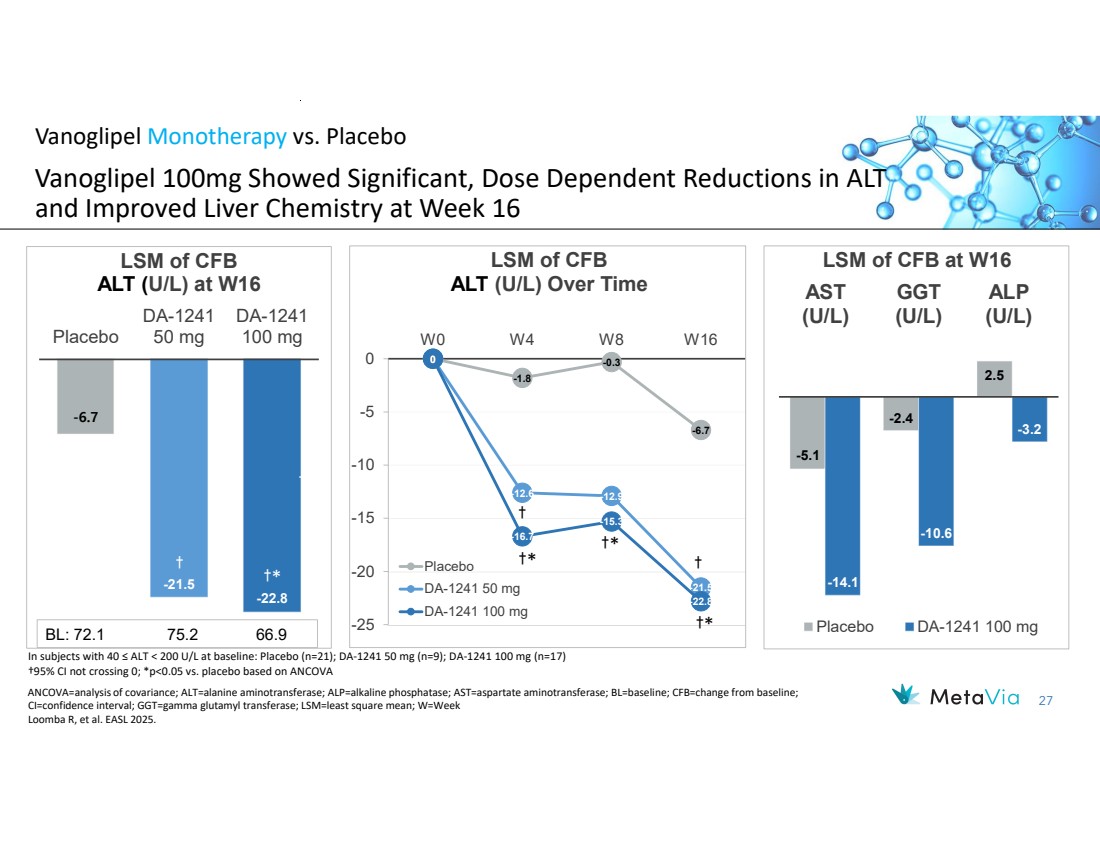
| 27 Vanoglipel Monotherapy vs. Placebo Vanoglipel 100mg Showed Significant, Dose Dependent Reductions in ALT and Improved Liver Chemistry at Week 16 -6.7 -21.5 -22.8 Placebo DA-1241 50 mg DA-1241 100 mg LSM of CFB ALT (U/L) at W16 †* † † BL: 72.1 75.2 66.9 -5.1 -2.4 2.5 -14.1 -10.6 -3.2 AST (U/L) GGT (U/L) ALP (U/L) LSM of CFB at W16 Placebo DA-1241 100 mg ANCOVA=analysis of covariance; ALT=alanine aminotransferase; ALP=alkaline phosphatase; AST=aspartate aminotransferase; BL=baseline; CFB=change from baseline; CI=confidence interval; GGT=gamma glutamyl transferase; LSM=least square mean; W=Week Loomba R, et al. EASL 2025. In subjects with 40 ≤ ALT < 200 U/L at baseline: Placebo (n=21); DA-1241 50 mg (n=9); DA-1241 100 mg (n=17) †95% CI not crossing 0; *p<0.05 vs. placebo based on ANCOVA 0 -1.8 -0.3 -6.7 0 -12.6 -12.9 -21.5 0 -16.7 -15.3 -22.8 -25 -20 -15 -10 -5 0 W0 W4 W8 W16 LSM of CFB ALT (U/L) Over Time Placebo DA-1241 50 mg DA-1241 100 mg †* †* †* † † |
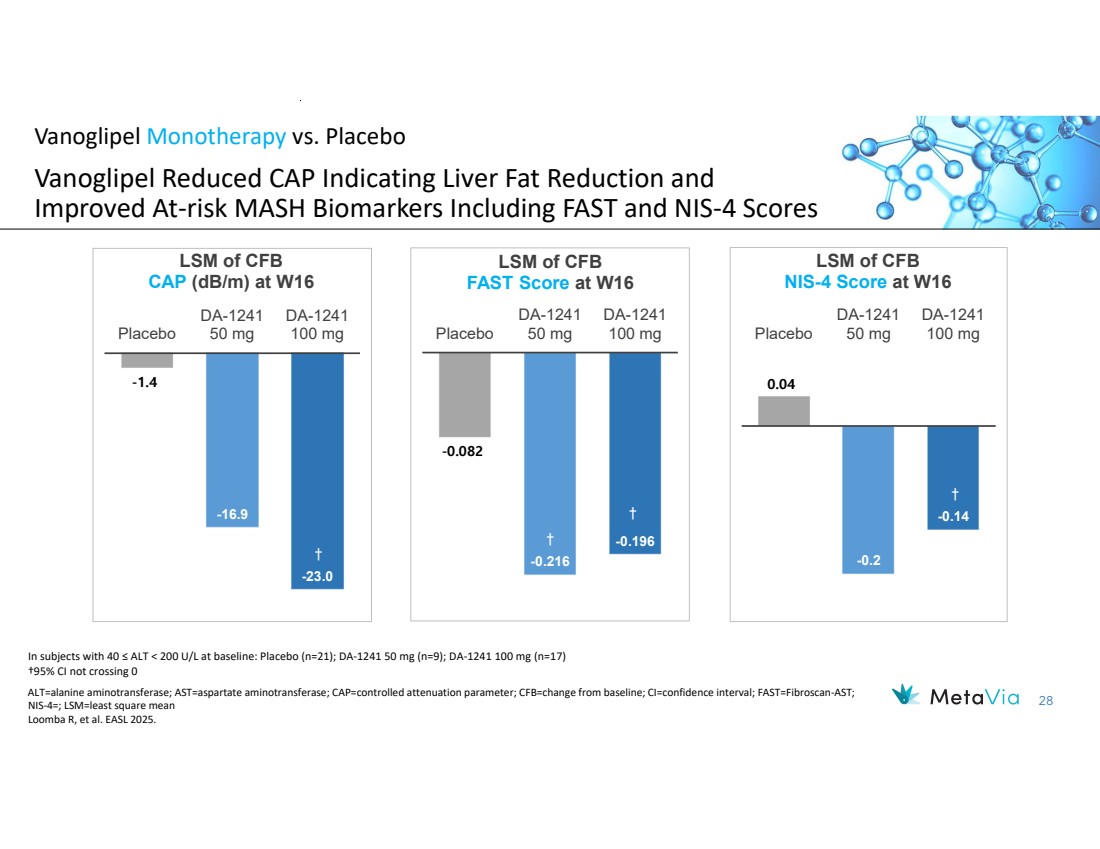
| 28 Vanoglipel Monotherapy vs. Placebo Vanoglipel Reduced CAP Indicating Liver Fat Reduction and Improved At-risk MASH Biomarkers Including FAST and NIS-4 Scores -1.4 -16.9 -23.0 Placebo DA-1241 50 mg DA-1241 100 mg LSM of CFB CAP (dB/m) at W16 † † -0.082 -0.216 -0.196 Placebo DA-1241 50 mg DA-1241 100 mg LSM of CFB FAST Score at W16 † † 0.04 -0.2 -0.14 Placebo DA-1241 50 mg DA-1241 100 mg LSM of CFB NIS-4 Score at W16 † ALT=alanine aminotransferase; AST=aspartate aminotransferase; CAP=controlled attenuation parameter; CFB=change from baseline; CI=confidence interval; FAST=Fibroscan-AST; NIS-4=; LSM=least square mean Loomba R, et al. EASL 2025. In subjects with 40 ≤ ALT < 200 U/L at baseline: Placebo (n=21); DA-1241 50 mg (n=9); DA-1241 100 mg (n=17) †95% CI not crossing 0 |
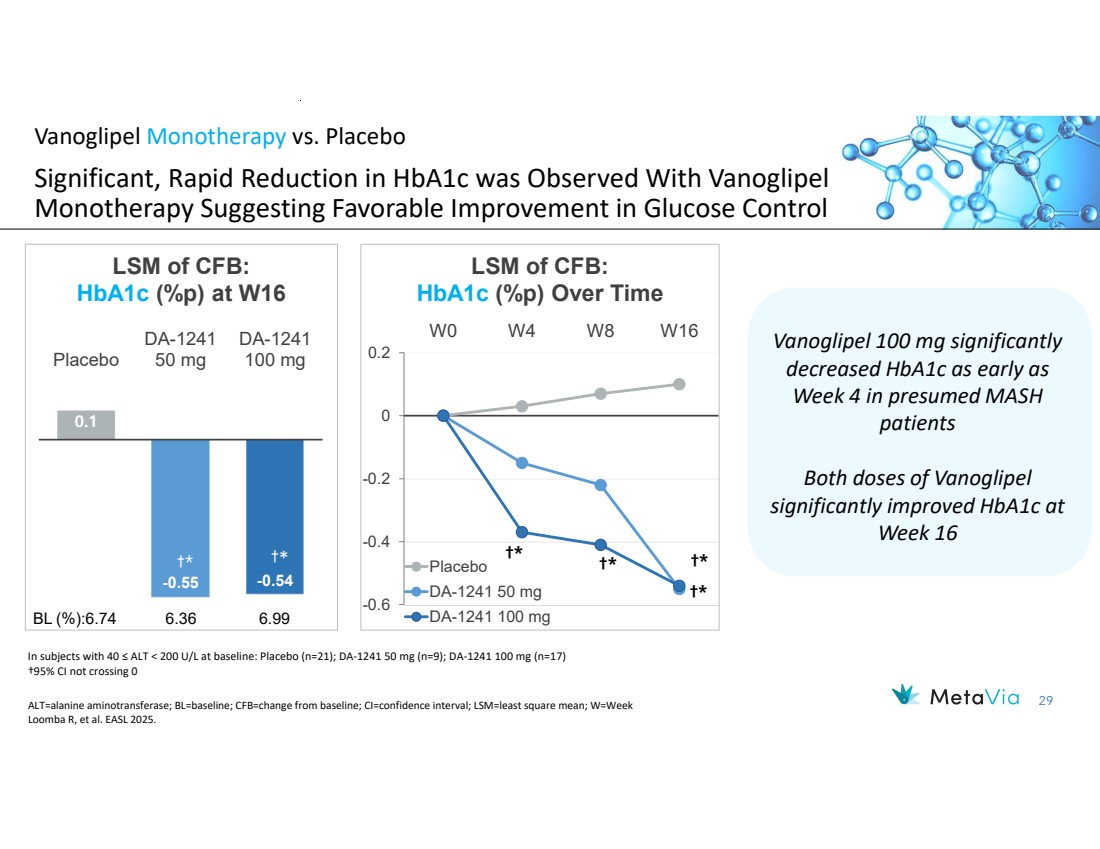
| 29 †* †* †* †* -0.6 -0.4 -0.2 0 0.2 W0 W4 W8 W16 LSM of CFB: HbA1c (%p) Over Time Placebo DA-1241 50 mg DA-1241 100 mg 0.1 -0.55 -0.54 Placebo DA-1241 50 mg DA-1241 100 mg LSM of CFB: HbA1c (%p) at W16 †* †* BL (%):6.74 6.36 6.99 Vanoglipel Monotherapy vs. Placebo Significant, Rapid Reduction in HbA1c was Observed With Vanoglipel Monotherapy Suggesting Favorable Improvement in Glucose Control Vanoglipel 100 mg significantly decreased HbA1c as early as Week 4 in presumed MASH patients Both doses of Vanoglipel significantly improved HbA1c at Week 16 In subjects with 40 ≤ ALT < 200 U/L at baseline: Placebo (n=21); DA-1241 50 mg (n=9); DA-1241 100 mg (n=17) †95% CI not crossing 0 ALT=alanine aminotransferase; BL=baseline; CFB=change from baseline; CI=confidence interval; LSM=least square mean; W=Week Loomba R, et al. EASL 2025. |
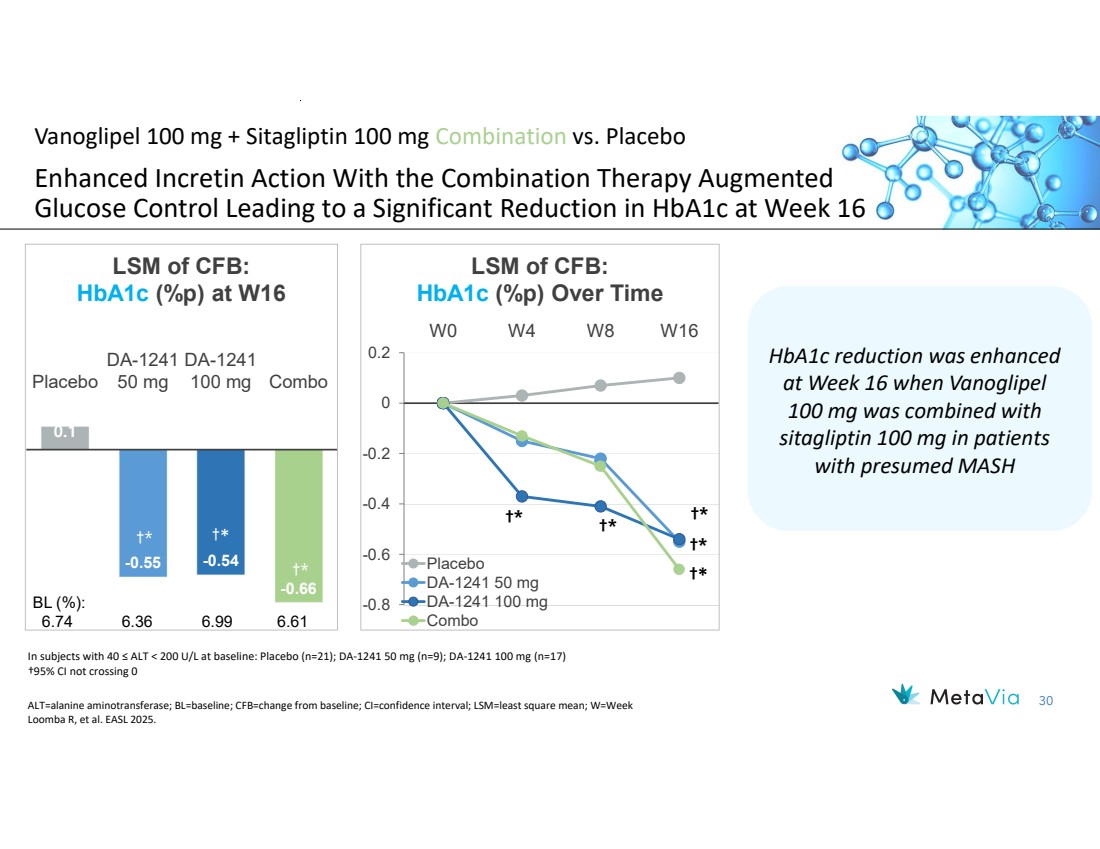
| 30 0.1 -0.55 -0.54 -0.66 Placebo DA-1241 50 mg DA-1241 100 mg Combo LSM of CFB: HbA1c (%p) at W16 †* †* BL (%): 6.74 6.36 6.99 6.61 Vanoglipel 100 mg + Sitagliptin 100 mg Combination vs. Placebo Enhanced Incretin Action With the Combination Therapy Augmented Glucose Control Leading to a Significant Reduction in HbA1c at Week 16 ALT=alanine aminotransferase; BL=baseline; CFB=change from baseline; CI=confidence interval; LSM=least square mean; W=Week Loomba R, et al. EASL 2025. In subjects with 40 ≤ ALT < 200 U/L at baseline: Placebo (n=21); DA-1241 50 mg (n=9); DA-1241 100 mg (n=17) †95% CI not crossing 0 †* †* †* †* -0.8 -0.6 -0.4 -0.2 0 0.2 W0 W4 W8 W16 LSM of CFB: HbA1c (%p) Over Time Placebo DA-1241 50 mg DA-1241 100 mg Combo †* †* HbA1c reduction was enhanced at Week 16 when Vanoglipel 100 mg was combined with sitagliptin 100 mg in patients with presumed MASH |
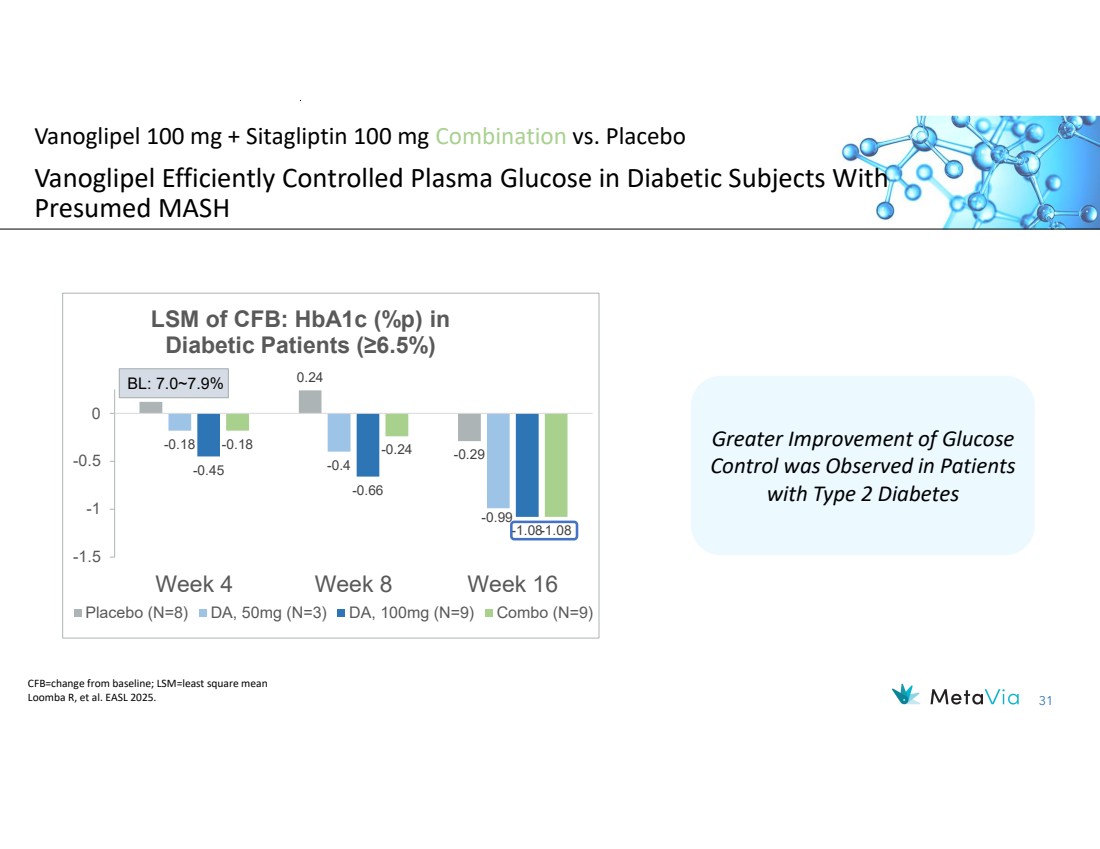
| 31 †* †* Vanoglipel 100 mg + Sitagliptin 100 mg Combination vs. Placebo Vanoglipel Efficiently Controlled Plasma Glucose in Diabetic Subjects With Presumed MASH CFB=change from baseline; LSM=least square mean Loomba R, et al. EASL 2025. †* Greater Improvement of Glucose Control was Observed in Patients with Type 2 Diabetes †* †* †* 0.12 0.24 -0.29 -0.18 -0.4 -0.99 -0.45 -0.66 -1.08 -0.18 -0.24 -1.08 -1.5 -1 -0.5 0 Week 4 Week 8 Week 16 LSM of CFB: HbA1c (%p) in Diabetic Patients (≥6.5%) Placebo (N=8) DA, 50mg (N=3) DA, 100mg (N=9) Combo (N=9) BL: 7.0~7.9% |
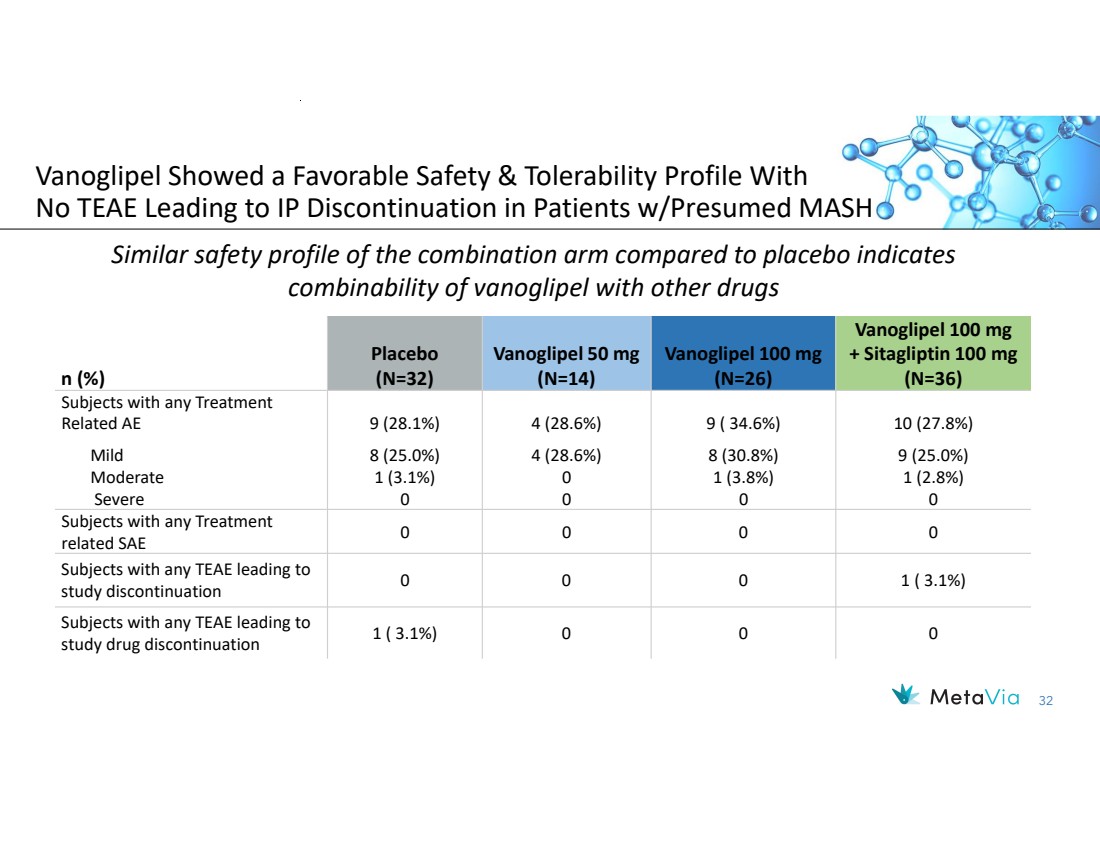
| 32 Vanoglipel Showed a Favorable Safety & Tolerability Profile With No TEAE Leading to IP Discontinuation in Patients w/Presumed MASH Vanoglipel 100 mg + Sitagliptin 100 mg (N=36) Vanoglipel 100 mg (N=26) Vanoglipel 50 mg (N=14) Placebo n (%) (N=32) 10 (27.8%) 9 (25.0%) 1 (2.8%) 0 9 ( 34.6%) 8 (30.8%) 1 (3.8%) 0 4 (28.6%) 4 (28.6%) 0 0 9 (28.1%) 8 (25.0%) 1 (3.1%) 0 Subjects with any Treatment Related AE Mild Moderate Severe 0 0 0 0 Subjects with any Treatment related SAE 0 0 0 1 ( 3.1%) Subjects with any TEAE leading to study discontinuation 1 ( 3.1%) 0 0 0 Subjects with any TEAE leading to study drug discontinuation Similar safety profile of the combination arm compared to placebo indicates combinability of vanoglipel with other drugs |
| 33 Vanoglipel+SEMA (GLP-1 RA) or Vanoglipel+EFX (FGF-21 Analog) Showed Additive Benefits in the GAN DIO-MASH Mouse Model Support the therapeutic potential of combining GPR119 agonists with GLP-1 RAs or FGF-21 analogues for the treatment of MASH: The combination improved plasma ALT, liver cholesterol, steatosis, inflammation, and fibrosis more effectively than either monotherapy 94% of combination-treated mice achieved ≥2-point NAS improvement from baseline Vanoglipel alone and in combination with EFX reduced inflammatory markers in the liver and plasma mRNA and histological analyses confirmed enhanced anti-inflammatory and anti-fibrotic effects Upregulation of Hhip suggests additional antifibrotic potential via hepatic stellate cell modulation Weight-neutrality of vanoglipel maintained; no additional weight loss beyond EFX alone |
| 34 Vanoglipel: Safety Data Provides Combination Therapy Opportunity for Patients with Large Unmet Need Vanoglipel has the unique advantage of clinical safety data in combination use that may lead to an improved treatment option of combination therapy By providing another MoA treatment option for MASH, vanoglipel may help to address the growing prevalence of MASH, thus leading to decreased morbidity and mortality as well as decreased costs associated with liver transplant |
| 35 Summary & Next Steps: Clinical Data Supports Development as Monotherapy or in Combination Opportunity in MASH and Metabolic Diseases MASH: Attractive area of large unmet need with ~$20B market by 2032 • Recent commercial success of Madrigal highlights large and growing untreated population Madrigal, Novo Nordisk, Roche recent acquisitions demonstrate belief in combination therapy benefit Vanoglipel: Clinical Stage Novel MOA (GRP119) for MASH & Metabolic Diseases Vanoglipel demonstrated both hepatoprotective and glucose-regulating effects in patients with presumed MASH • Significantly improved ALT and other liver enzymes, and efficiently lowered HbA1c • Safe and well tolerated in Phase 1 and 2a studies • Demonstrated combinability; safety profile of the combination arm in Phase 2 was similar to that of placebo • Additive benefits when combined with other MoAs demonstrated in the GAN DIO-MASH mouse model Vanoglipel shows promise in combination in Metabolic Disease, including Type 2 Diabetes • Demonstrated clean and tolerable profile plus glucose control Strong IP, including composition of matter patent Next Steps MetaVia has begun partnering discussions; seeking initial indications of interest in coming months |
| December 2023 NASDAQ: NRBO 36 Financials and Capitalization |

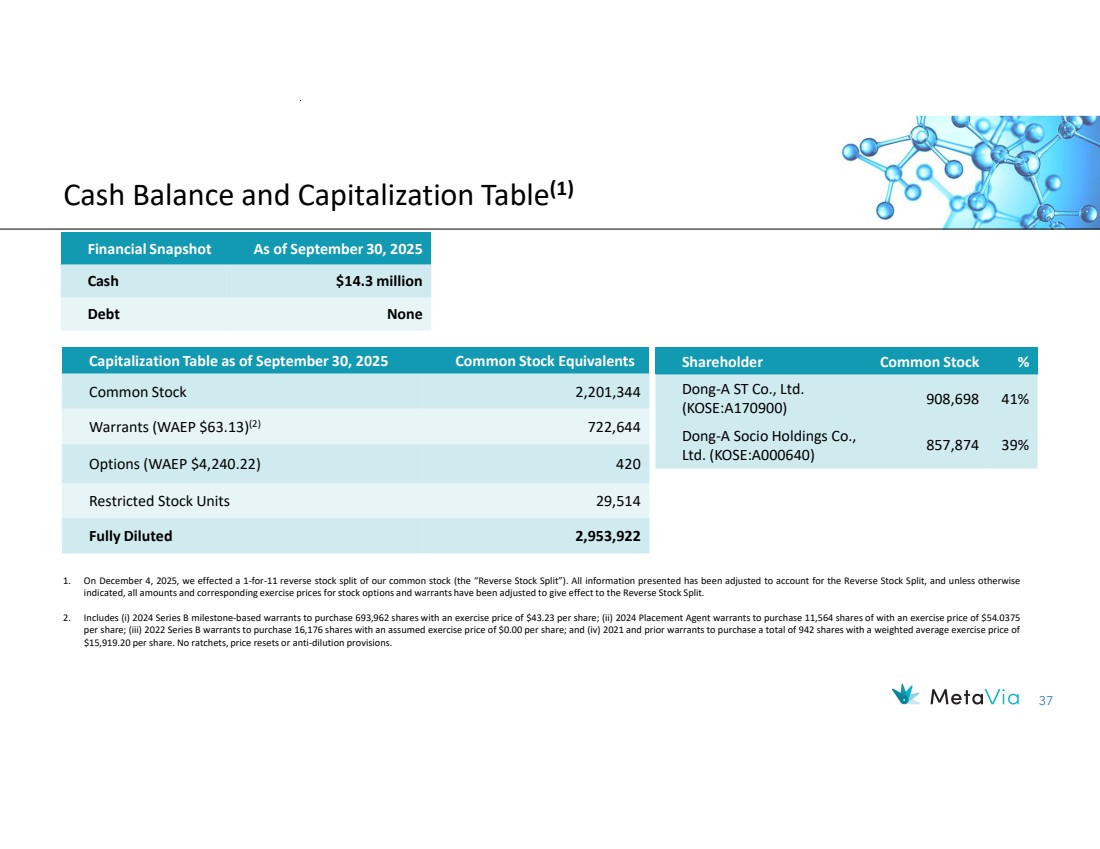
| 37 Cash Balance and Capitalization Table(1) Financial Snapshot As of September 30, 2025 Cash $14.3 million Debt None Capitalization Table as of September 30, 2025 Common Stock Equivalents Common Stock 2,201,344 Warrants (WAEP $63.13) 722,644 (2) Options (WAEP $4,240.22) 420 Restricted Stock Units 29,514 Fully Diluted 2,953,922 1. On December 4, 2025, we effected a 1-for-11 reverse stock split of our common stock (the “Reverse Stock Split”). All information presented has been adjusted to account for the Reverse Stock Split, and unless otherwise indicated, all amounts and corresponding exercise prices for stock options and warrants have been adjusted to give effect to the Reverse Stock Split. 2. Includes (i) 2024 Series B milestone-based warrants to purchase 693,962 shares with an exercise price of $43.23 per share; (ii) 2024 Placement Agent warrants to purchase 11,564 shares of with an exercise price of $54.0375 per share; (iii) 2022 Series B warrants to purchase 16,176 shares with an assumed exercise price of $0.00 per share; and (iv) 2021 and prior warrants to purchase a total of 942 shares with a weighted average exercise price of $15,919.20 per share. No ratchets, price resets or anti-dilution provisions. Shareholder Common Stock % 908,698 41% Dong-A ST Co., Ltd. (KOSE:A170900) 857,874 39% Dong-A Socio Holdings Co., Ltd. (KOSE:A000640) |
| 38 Compelling Investment Opportunity Targeting Obesity and MASH with a Pipeline of Next Generation Therapeutics Aiming to increase Shareholder Value through Multiple, Near-Term, Value Creating Milestones • DA-1726 Potential for best-in-class weight loss, glucose control, and direct hepatic effect Mean -9.1% weight loss, -3.8 inches reduction in waist, -0.22pp in HbA1c, and -23.7% VCTE reduction in non-titrated 48 mg With compelling safety profile with non-titrated 48 mg dosing, exploring better tolerability with titration dosing up to 64 mg One-Step titration (Part 3a) planned: 16 mg x 4 week → 48 mg x 12 week Two-Step titration (Part 3b) planned: 16 mg x 4 week → 32 mg x 4 week → 64 mg x 8 week Parts 3a and 3b data readout by end of 2026 16-week study in obese patients with T2D targeting FPI in 1H 2026 • Vanoglipel (DA-1241) Phase 2a top-line data in subjects with presumed MASH met primary endpoint and showed direct hepatic effects With added significant reductions in HbA1c from baseline at 100 mg vanoglipel compared to placebo at Week 16 o Other exploratory endpoints including MRI-PDFF to be released at major medical conferences o Actively seeking combination/licensing partner |
| December 2023 NASDAQ: NRBO 39 Thank You! Investor Contacts: Rx Communications Group Michael Miller +1 917.633.6086 mmiller@rxir.com MetaVia Marshall Woodworth +1 919.749.8748 marshall.woodworth@metaviatx.com |

| December 2023 NASDAQ: NRBO 40 Appendix |

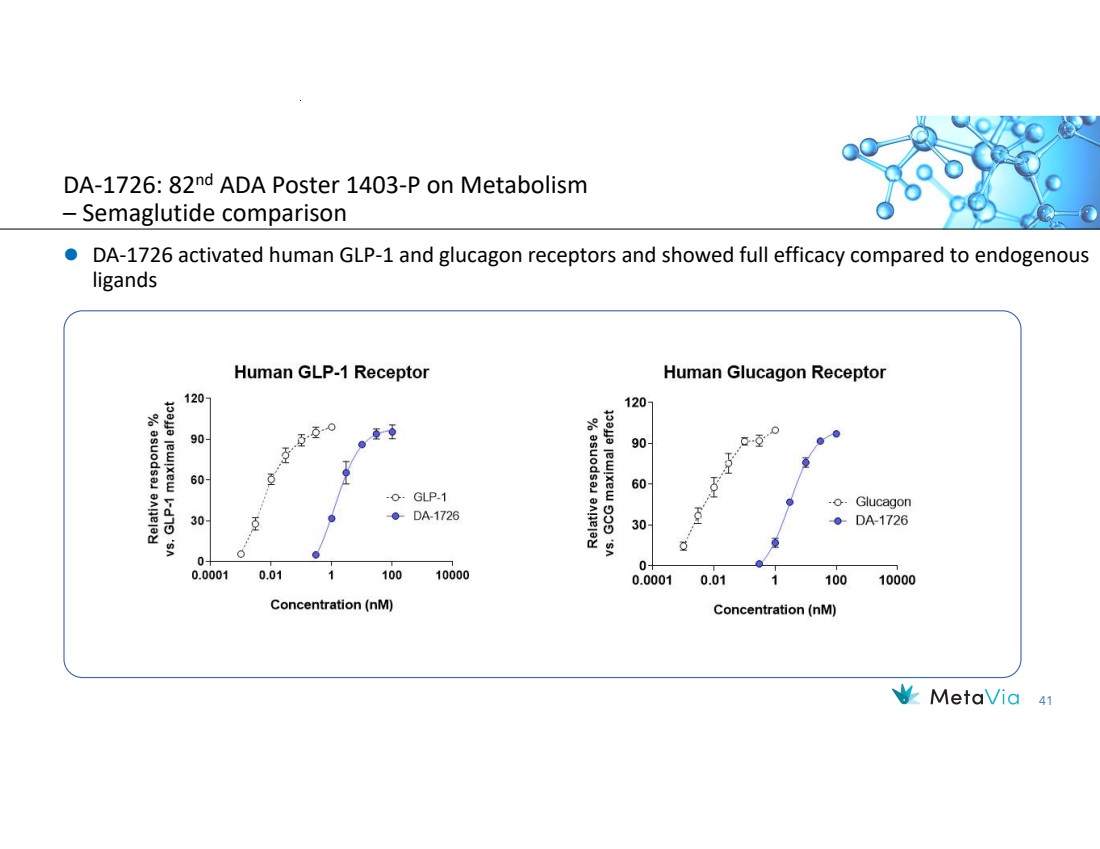
| 41 DA-1726 activated human GLP-1 and glucagon receptors and showed full efficacy compared to endogenous ligands DA-1726: 82nd ADA Poster 1403-P on Metabolism – Semaglutide comparison |
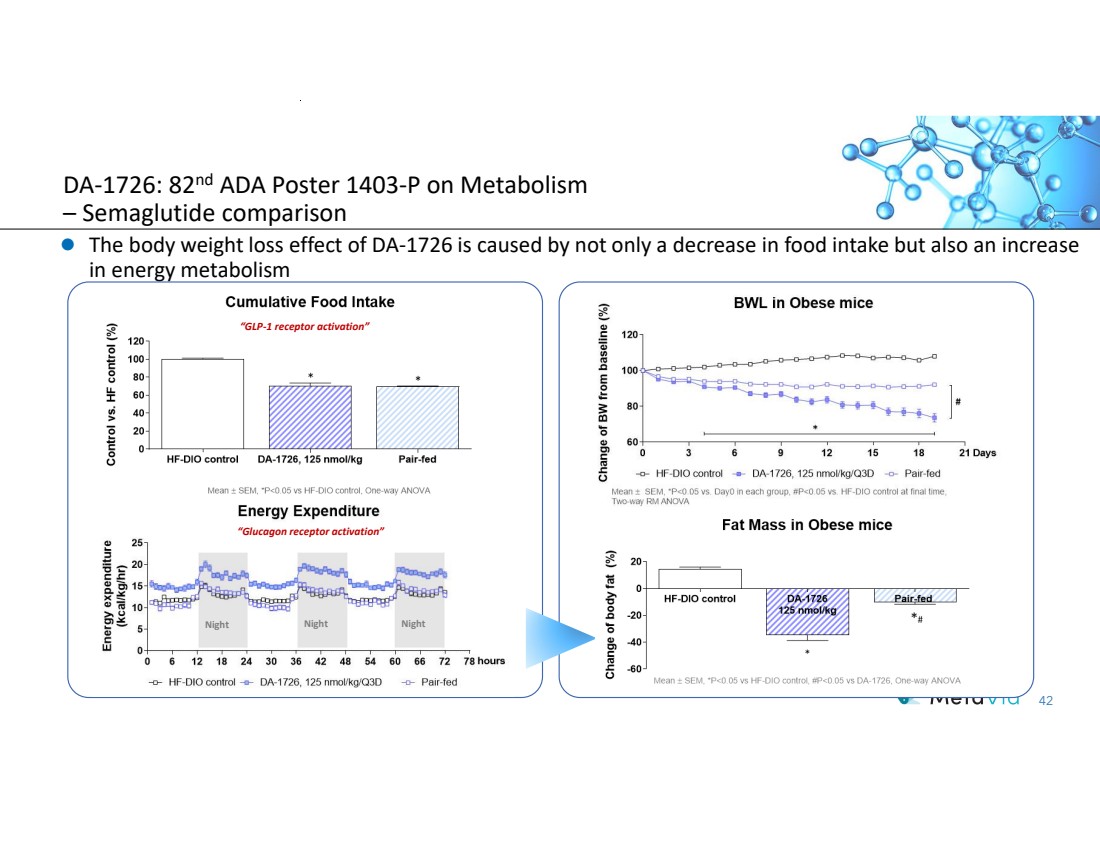
| 42 The body weight loss effect of DA-1726 is caused by not only a decrease in food intake but also an increase in energy metabolism Night Night Night “Glucagon receptor activation” “GLP-1 receptor activation” DA-1726: 82nd ADA Poster 1403-P on Metabolism – Semaglutide comparison |
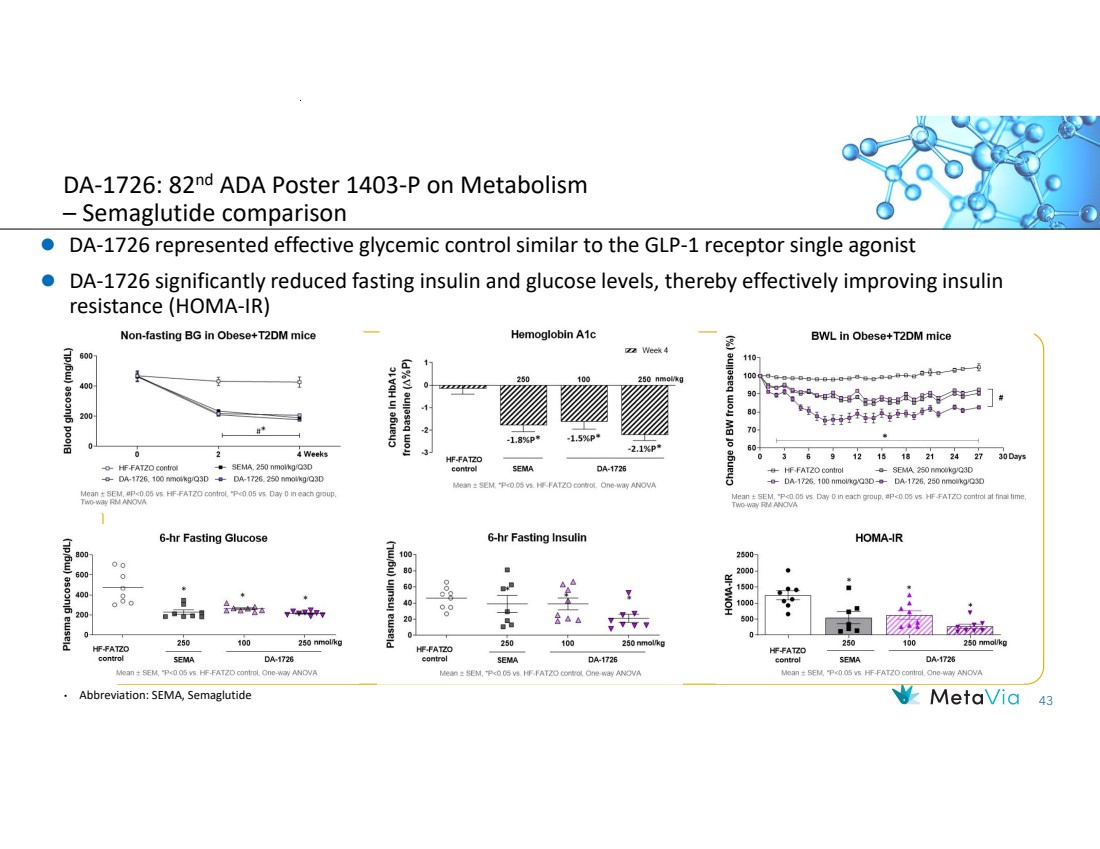
| 43 DA-1726 represented effective glycemic control similar to the GLP-1 receptor single agonist DA-1726 significantly reduced fasting insulin and glucose levels, thereby effectively improving insulin resistance (HOMA-IR) DA-1726: 82nd ADA Poster 1403-P on Metabolism – Semaglutide comparison • Abbreviation: SEMA, Semaglutide |
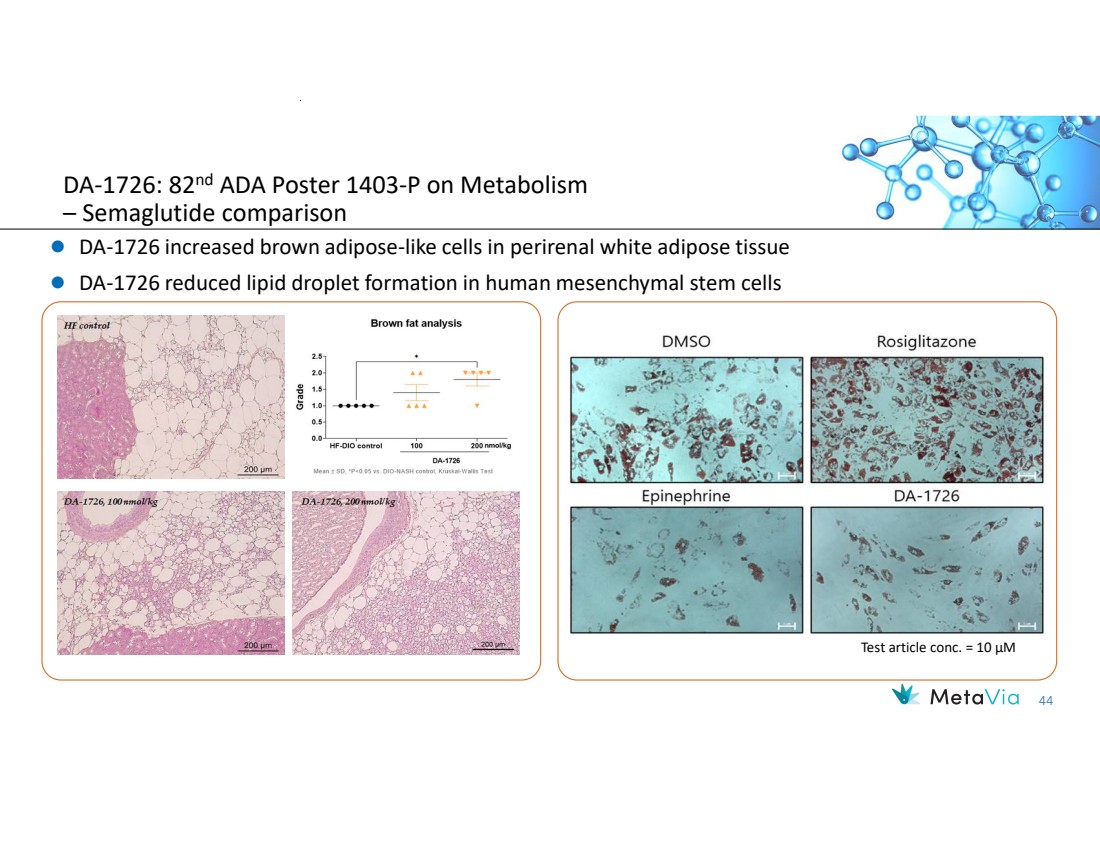
| 44 DA-1726 increased brown adipose-like cells in perirenal white adipose tissue DA-1726 reduced lipid droplet formation in human mesenchymal stem cells Test article conc. = 10 µM DA-1726: 82nd ADA Poster 1403-P on Metabolism – Semaglutide comparison |
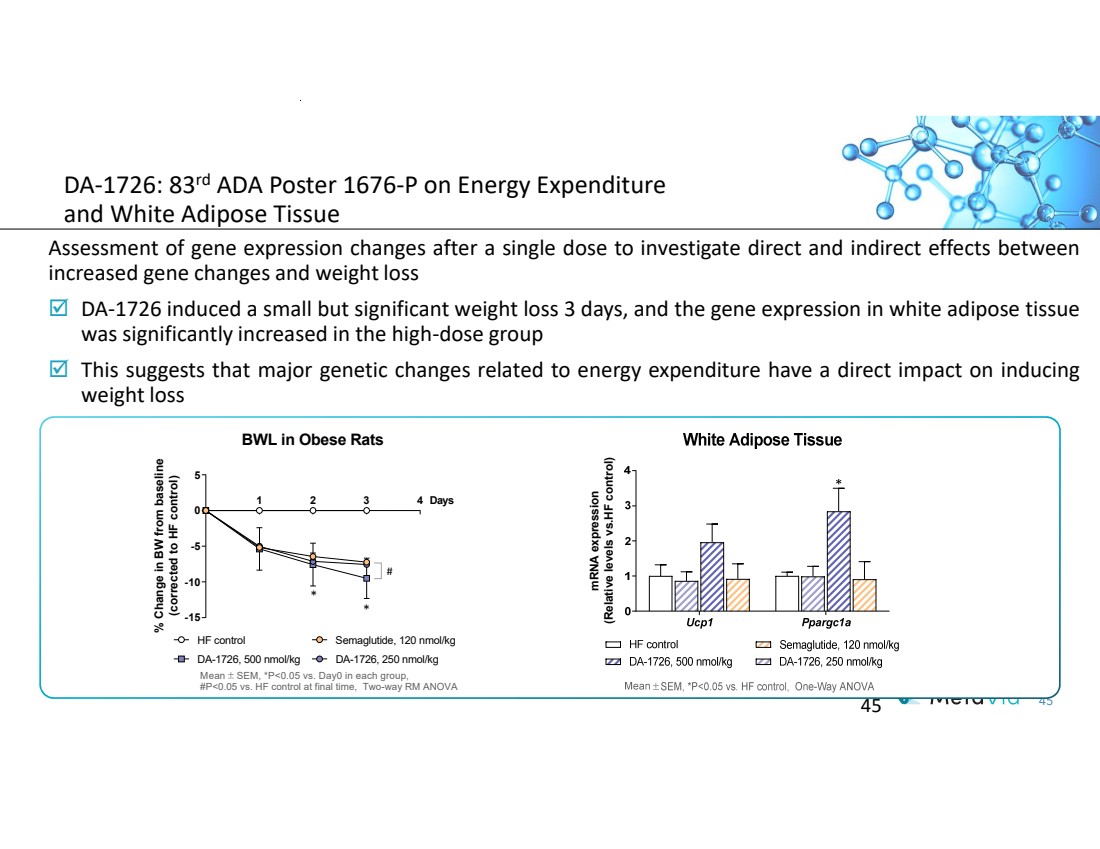
| 45 DA-1726: 83rd ADA Poster 1676-P on Energy Expenditure and White Adipose Tissue Assessment of gene expression changes after a single dose to investigate direct and indirect effects between increased gene changes and weight loss DA-1726 induced a small but significant weight loss 3 days, and the gene expression in white adipose tissue was significantly increased in the high-dose group This suggests that major genetic changes related to energy expenditure have a direct impact on inducing weight loss 45 BWL in Obese Rats 1 2 3 4 -15 -10 -5 0 5 DA-1726, 500 nmol/kg Mean SEM, *P<0.05 vs. Day0 in each group, #P<0.05 vs. HF control at final time, Two-way RM ANOVA HF control * DA-1726, 250 nmol/kg # * Semaglutide, 120 nmol/kg % Change in B W fro m baseline (corrected to HF control) Days m R N A expression (Relative levels vs.HF control) |
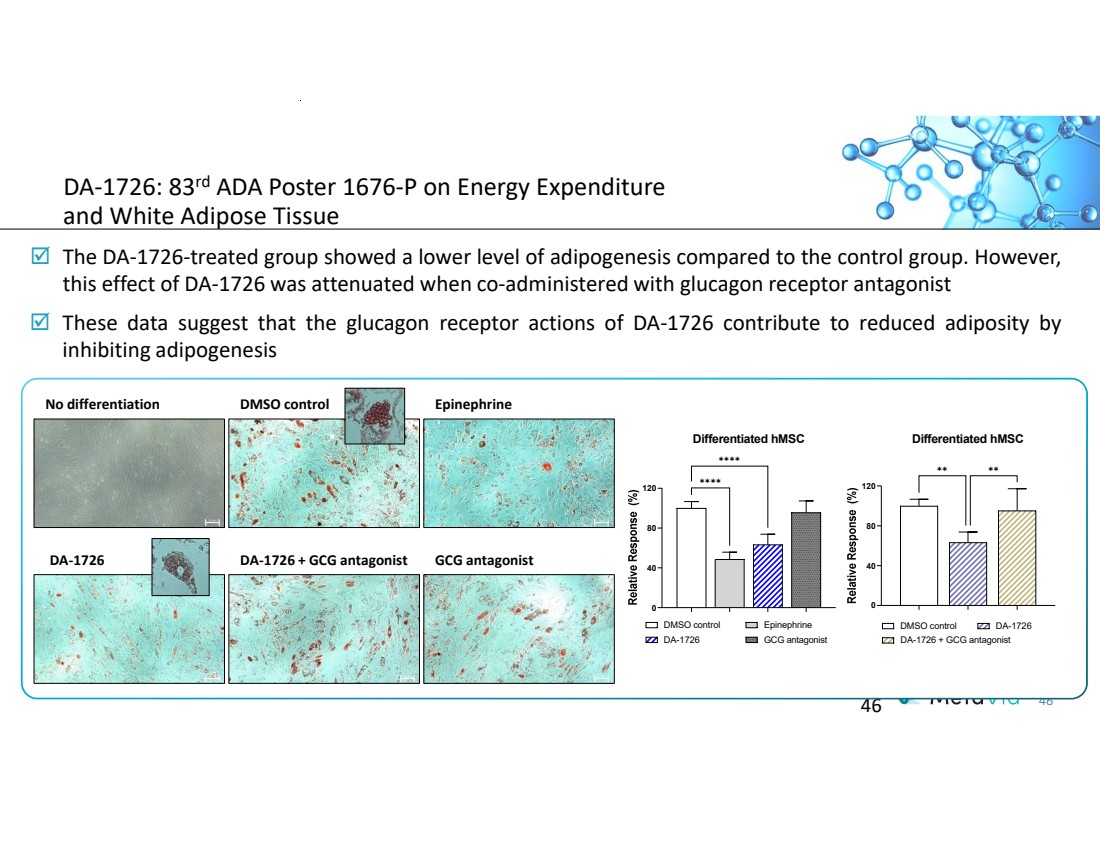
| 46 DA-1726: 83rd ADA Poster 1676-P on Energy Expenditure and White Adipose Tissue The DA-1726-treated group showed a lower level of adipogenesis compared to the control group. However, this effect of DA-1726 was attenuated when co-administered with glucagon receptor antagonist These data suggest that the glucagon receptor actions of DA-1726 contribute to reduced adiposity by inhibiting adipogenesis 46 No differentiation DMSO control Epinephrine DA-1726 DA-1726 + GCG antagonist GCG antagonist 0 40 80 120 Differentiated hMSC DMSO control Epinephrine DA-1726 GCG antagonist ✱✱✱✱ ✱✱✱✱ 0 40 80 120 Differentiated hMSC DMSO control DA-1726 DA-1726 + GCG antagonist ✱✱ ✱✱ |
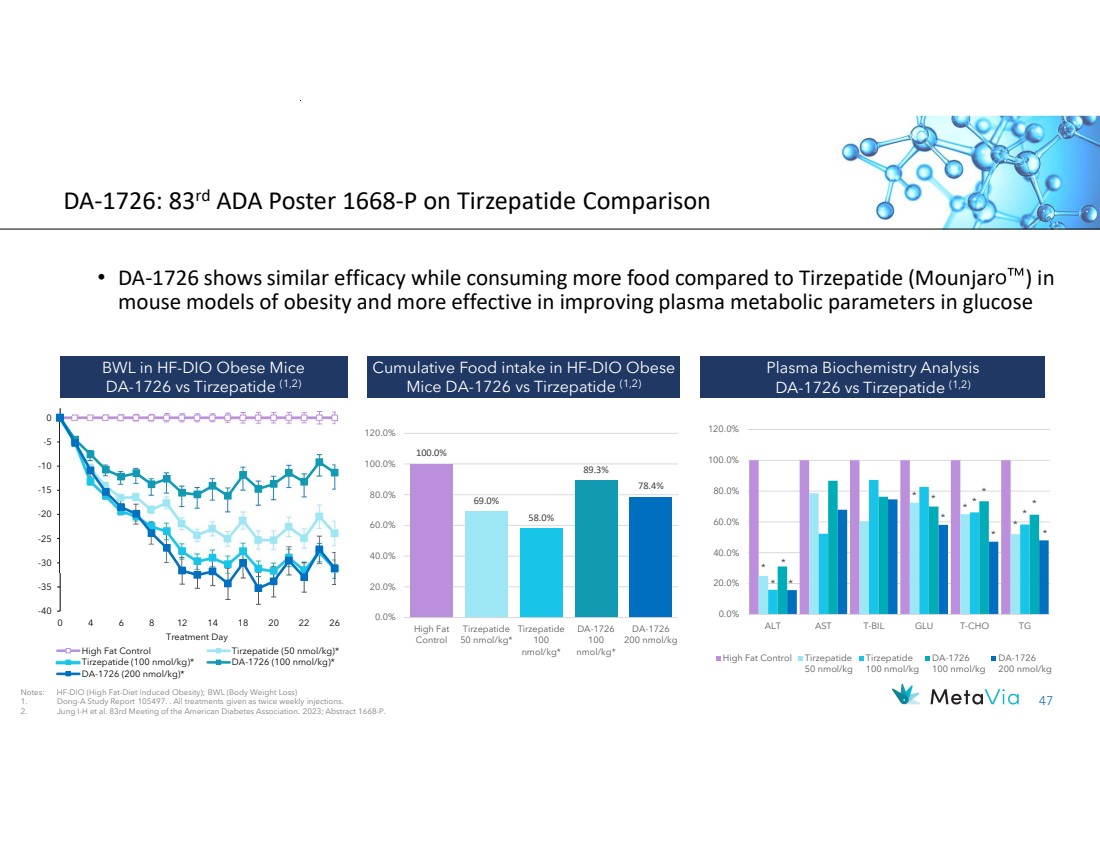
| 47 DA-1726: 83rd ADA Poster 1668-P on Tirzepatide Comparison • DA-1726 shows similar efficacy while consuming more food compared to Tirzepatide (Mounjaro ) in mouse models of obesity and more effective in improving plasma metabolic parameters in glucose Cumulative Food intake in HF-DIO Obese Mice DA-1726 vs Tirzepatide (1,2) BWL in HF-DIO Obese Mice DA-1726 vs Tirzepatide (1,2) Plasma Biochemistry Analysis DA-1726 vs Tirzepatide (1,2) Notes: HF-DIO (High Fat-Diet Induced Obesity); BWL (Body Weight Loss) 1. Dong-A Study Report 105497. . All treatments given as twice weekly injections. 2. Jung I-H et al. 83rd Meeting of the American Diabetes Association. 2023; Abstract 1668-P. -40 -35 -30 -25 -20 -15 -10 -5 0 0 4 6 8 12 14 18 20 22 26 Treatment Day High Fat Control Tirzepatide (50 nmol/kg)* Tirzepatide (100 nmol/kg)* DA-1726 (100 nmol/kg)* DA-1726 (200 nmol/kg)* 100.0% 69.0% 58.0% 89.3% 78.4% 0.0% 20.0% 40.0% 60.0% 80.0% 100.0% 120.0% High Fat Control Tirzepatide 50 nmol/kg* Tirzepatide 100 nmol/kg* DA-1726 100 nmol/kg* DA-1726 200 nmol/kg * * * * * * * * * * * * * * * 0.0% 20.0% 40.0% 60.0% 80.0% 100.0% 120.0% ALT AST T-BIL GLU T-CHO TG High Fat Control Tirzepatide 50 nmol/kg Tirzepatide 100 nmol/kg DA-1726 100 nmol/kg DA-1726 200 nmol/kg |
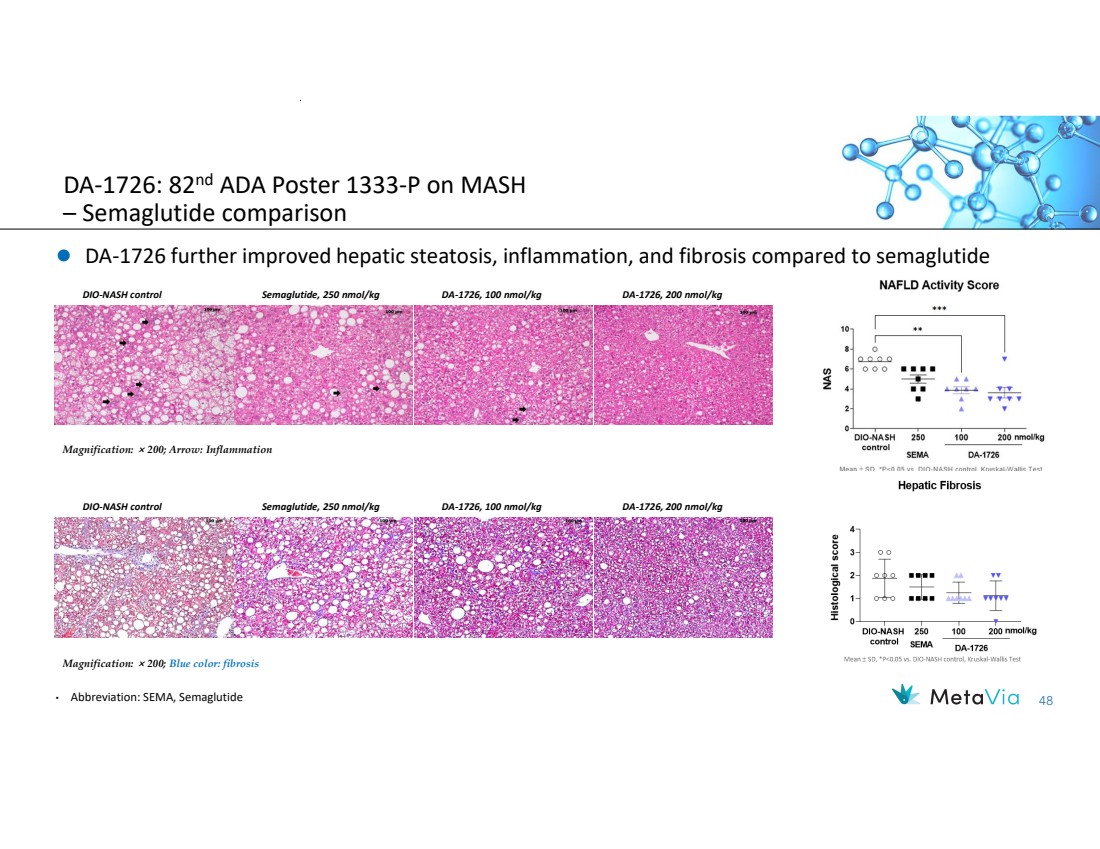
| 48 DA-1726: 82nd ADA Poster 1333-P on MASH – Semaglutide comparison DA-1726 further improved hepatic steatosis, inflammation, and fibrosis compared to semaglutide Magnification: × 200; Arrow: Inflammation DIO-NASH control Semaglutide, 250 nmol/kg DA-1726, 100 nmol/kg DA-1726, 200 nmol/kg DIO-NASH control Semaglutide, 250 nmol/kg DA-1726, 100 nmol/kg DA-1726, 200 nmol/kg Magnification: × 200; Blue color: fibrosis • Abbreviation: SEMA, Semaglutide |
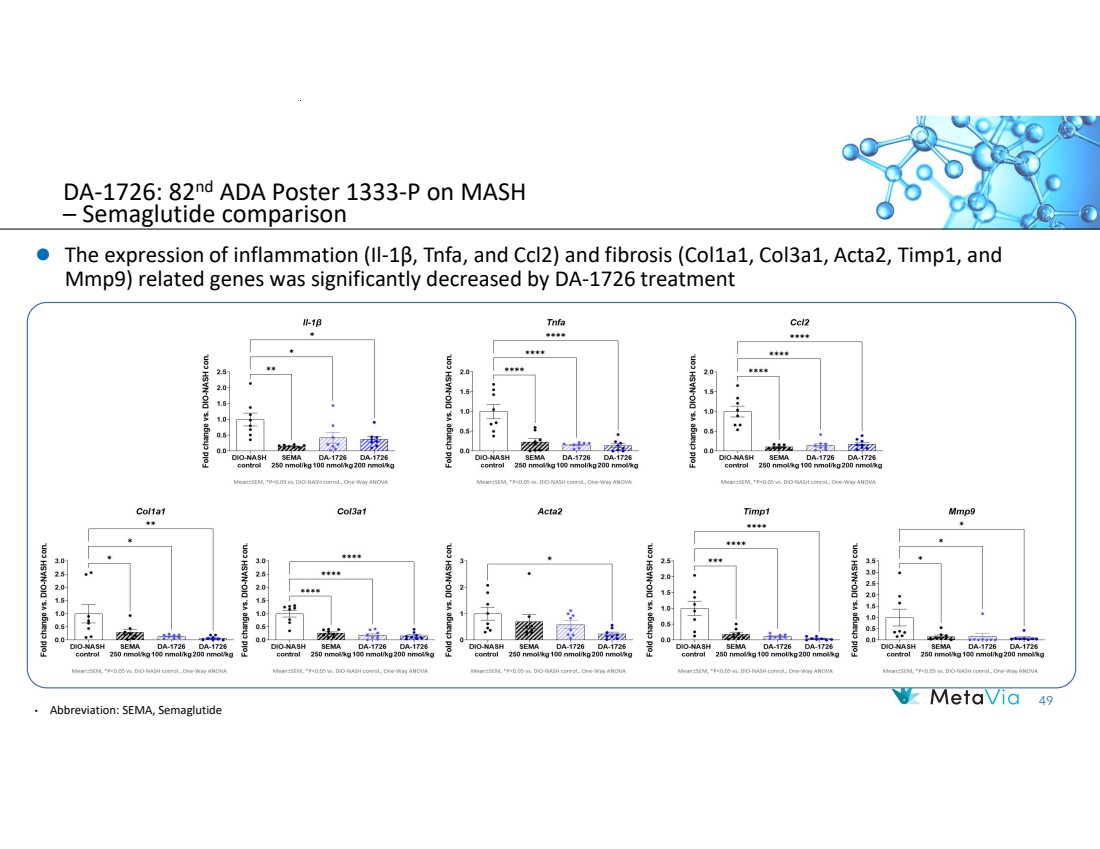
| 49 The expression of inflammation (Il-1β, Tnfa, and Ccl2) and fibrosis (Col1a1, Col3a1, Acta2, Timp1, and Mmp9) related genes was significantly decreased by DA-1726 treatment DA-1726: 82nd ADA Poster 1333-P on MASH – Semaglutide comparison • Abbreviation: SEMA, Semaglutide |
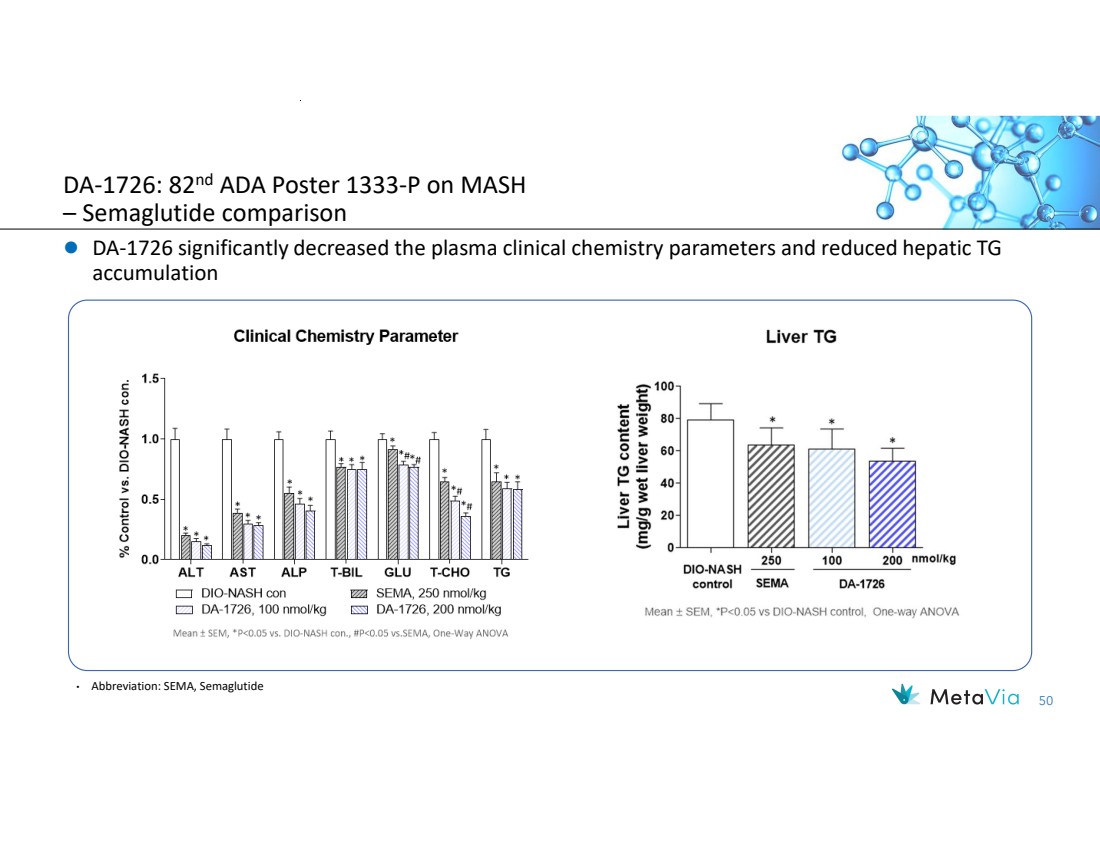
| 50 DA-1726 significantly decreased the plasma clinical chemistry parameters and reduced hepatic TG accumulation • Abbreviation: SEMA, Semaglutide DA-1726: 82nd ADA Poster 1333-P on MASH – Semaglutide comparison |
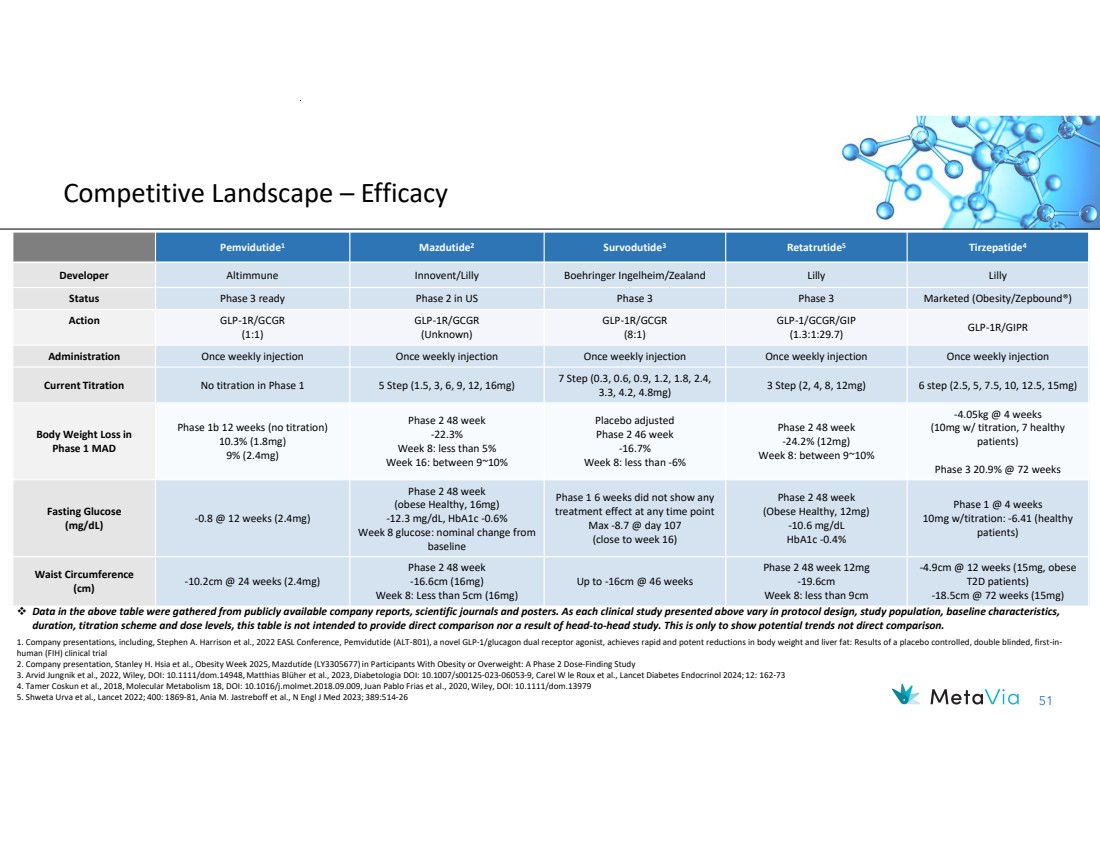
| 51 Competitive Landscape – Efficacy Tirzepatide4 Retatrutide5 Survodutide Mazdutide2 3 Pemvidutide1 Developer Altimmune Innovent/Lilly Boehringer Ingelheim/Zealand Lilly Lilly Status Phase 3 ready Phase 2 in US Phase 3 Phase 3 Marketed (Obesity/Zepbound®) GLP-1R/GIPR GLP-1/GCGR/GIP (1.3:1:29.7) GLP-1R/GCGR (8:1) GLP-1R/GCGR (Unknown) GLP-1R/GCGR (1:1) Action Administration Once weekly injection Once weekly injection Once weekly injection Once weekly injection Once weekly injection 3 Step (2, 4, 8, 12mg) 6 step (2.5, 5, 7.5, 10, 12.5, 15mg) 7 Step (0.3, 0.6, 0.9, 1.2, 1.8, 2.4, 3.3, 4.2, 4.8mg) Current Titration No titration in Phase 1 5 Step (1.5, 3, 6, 9, 12, 16mg) -4.05kg @ 4 weeks (10mg w/ titration, 7 healthy patients) Phase 3 20.9% @ 72 weeks Phase 2 48 week -24.2% (12mg) Week 8: between 9~10% Placebo adjusted Phase 2 46 week -16.7% Week 8: less than -6% Phase 2 48 week -22.3% Week 8: less than 5% Week 16: between 9~10% Phase 1b 12 weeks (no titration) 10.3% (1.8mg) 9% (2.4mg) Body Weight Loss in Phase 1 MAD Phase 1 @ 4 weeks 10mg w/titration: -6.41 (healthy patients) Phase 2 48 week (Obese Healthy, 12mg) -10.6 mg/dL HbA1c -0.4% Phase 1 6 weeks did not show any treatment effect at any time point Max -8.7 @ day 107 (close to week 16) Phase 2 48 week (obese Healthy, 16mg) -12.3 mg/dL, HbA1c -0.6% Week 8 glucose: nominal change from baseline -0.8 @ 12 weeks (2.4mg) Fasting Glucose (mg/dL) -4.9cm @ 12 weeks (15mg, obese T2D patients) -18.5cm @ 72 weeks (15mg) Phase 2 48 week 12mg -19.6cm Week 8: less than 9cm Up to -16cm @ 46 weeks Phase 2 48 week -16.6cm (16mg) Week 8: Less than 5cm (16mg) -10.2cm @ 24 weeks (2.4mg) Waist Circumference (cm) Data in the above table were gathered from publicly available company reports, scientific journals and posters. As each clinical study presented above vary in protocol design, study population, baseline characteristics, duration, titration scheme and dose levels, this table is not intended to provide direct comparison nor a result of head-to-head study. This is only to show potential trends not direct comparison. 1. Company presentations, including, Stephen A. Harrison et al., 2022 EASL Conference, Pemvidutide (ALT-801), a novel GLP-1/glucagon dual receptor agonist, achieves rapid and potent reductions in body weight and liver fat: Results of a placebo controlled, double blinded, first-in-human (FIH) clinical trial 2. Company presentation, Stanley H. Hsia et al., Obesity Week 2025, Mazdutide (LY3305677) in Participants With Obesity or Overweight: A Phase 2 Dose-Finding Study 3. Arvid Jungnik et al., 2022, Wiley, DOI: 10.1111/dom.14948, Matthias Blüher et al., 2023, Diabetologia DOI: 10.1007/s00125-023-06053-9, Carel W le Roux et al., Lancet Diabetes Endocrinol 2024; 12: 162-73 4. Tamer Coskun et al., 2018, Molecular Metabolism 18, DOI: 10.1016/j.molmet.2018.09.009, Juan Pablo Frias et al., 2020, Wiley, DOI: 10.1111/dom.13979 5. Shweta Urva et al., Lancet 2022; 400: 1869-81, Ania M. Jastreboff et al., N Engl J Med 2023; 389:514-26 |
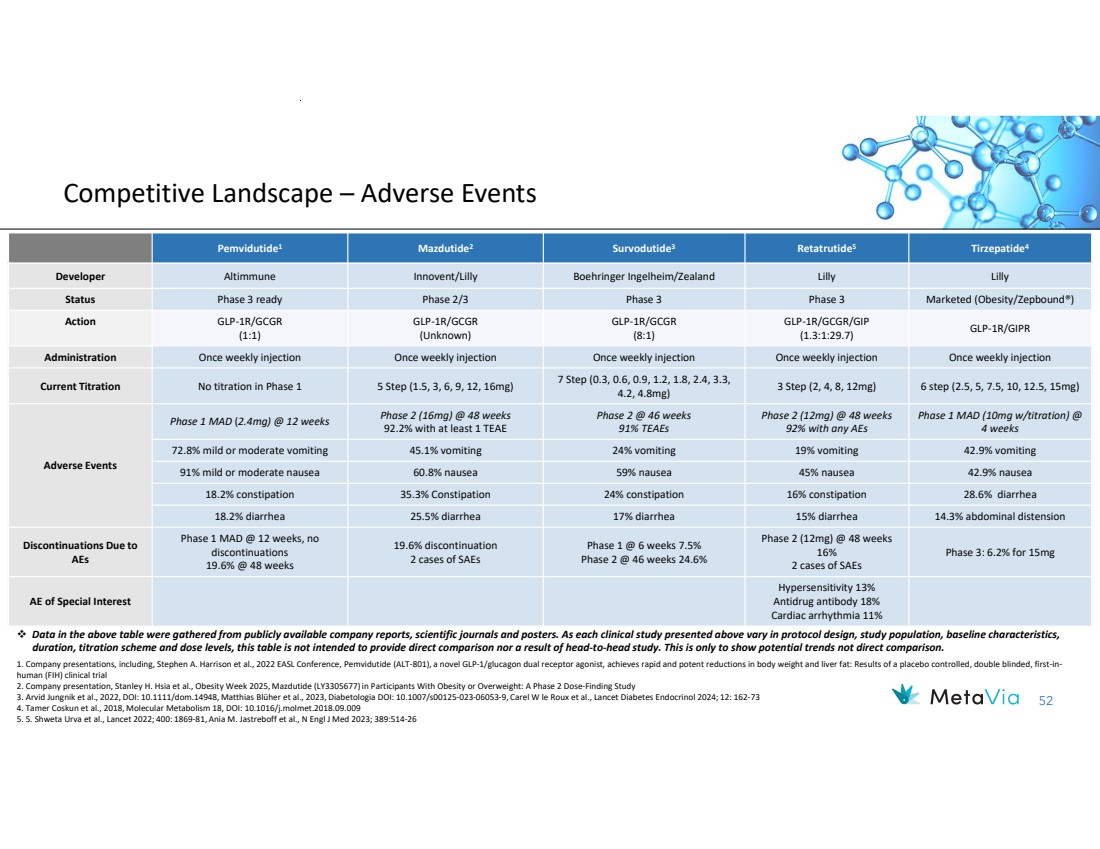
| 52 Competitive Landscape – Adverse Events Tirzepatide4 Retatrutide5 Survodutide Mazdutide2 3 Pemvidutide1 Developer Altimmune Innovent/Lilly Boehringer Ingelheim/Zealand Lilly Lilly Status Phase 3 ready Phase 2/3 Phase 3 Phase 3 Marketed (Obesity/Zepbound®) GLP-1R/GIPR GLP-1R/GCGR/GIP (1.3:1:29.7) GLP-1R/GCGR (8:1) GLP-1R/GCGR (Unknown) GLP-1R/GCGR (1:1) Action Administration Once weekly injection Once weekly injection Once weekly injection Once weekly injection Once weekly injection 3 Step (2, 4, 8, 12mg) 6 step (2.5, 5, 7.5, 10, 12.5, 15mg) 7 Step (0.3, 0.6, 0.9, 1.2, 1.8, 2.4, 3.3, 4.2, 4.8mg) Current Titration No titration in Phase 1 5 Step (1.5, 3, 6, 9, 12, 16mg) Phase 1 MAD (10mg w/titration) @ 4 weeks Phase 2 (12mg) @ 48 weeks 92% with any AEs Phase 2 @ 46 weeks 91% TEAEs Phase 2 (16mg) @ 48 weeks 92.2% with at least 1 TEAE Phase 1 MAD (2.4mg) @ 12 weeks Adverse Events 72.8% mild or moderate vomiting 45.1% vomiting 24% vomiting 19% vomiting 42.9% vomiting 91% mild or moderate nausea 60.8% nausea 59% nausea 45% nausea 42.9% nausea 18.2% constipation 35.3% Constipation 24% constipation 16% constipation 28.6% diarrhea 18.2% diarrhea 25.5% diarrhea 17% diarrhea 15% diarrhea 14.3% abdominal distension Phase 3: 6.2% for 15mg Phase 2 (12mg) @ 48 weeks 16% 2 cases of SAEs Phase 1 @ 6 weeks 7.5% Phase 2 @ 46 weeks 24.6% 19.6% discontinuation 2 cases of SAEs Phase 1 MAD @ 12 weeks, no discontinuations 19.6% @ 48 weeks Discontinuations Due to AEs Hypersensitivity 13% Antidrug antibody 18% Cardiac arrhythmia 11% AE of Special Interest Data in the above table were gathered from publicly available company reports, scientific journals and posters. As each clinical study presented above vary in protocol design, study population, baseline characteristics, duration, titration scheme and dose levels, this table is not intended to provide direct comparison nor a result of head-to-head study. This is only to show potential trends not direct comparison. 1. Company presentations, including, Stephen A. Harrison et al., 2022 EASL Conference, Pemvidutide (ALT-801), a novel GLP-1/glucagon dual receptor agonist, achieves rapid and potent reductions in body weight and liver fat: Results of a placebo controlled, double blinded, first-in-human (FIH) clinical trial 2. Company presentation, Stanley H. Hsia et al., Obesity Week 2025, Mazdutide (LY3305677) in Participants With Obesity or Overweight: A Phase 2 Dose-Finding Study 3. Arvid Jungnik et al., 2022, DOI: 10.1111/dom.14948, Matthias Blüher et al., 2023, Diabetologia DOI: 10.1007/s00125-023-06053-9, Carel W le Roux et al., Lancet Diabetes Endocrinol 2024; 12: 162-73 4. Tamer Coskun et al., 2018, Molecular Metabolism 18, DOI: 10.1016/j.molmet.2018.09.009 5. 5. Shweta Urva et al., Lancet 2022; 400: 1869-81, Ania M. Jastreboff et al., N Engl J Med 2023; 389:514-26 |