TX45 Phase 1b (Part B) PH-HFrEF Data Release Single Dose Hemodynamic Trial O c t o b e r 2025
2 DISCLAIMER Statements contained in this presentation regarding matters that are not historical facts are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, as amended. Words such as anticipates, believes, expects, intends, “plans,” “potential,” projects,” “would” and future or similar expressions are intended to identify forward-looking statements. Each of these forward-looking statements involves substantial risks and uncertainties that could cause actual results to differ significantly from those expressed or implied by such forward- looking statements. Forward-looking statements contained in this presentation include, but are not limited to, statements regarding: the design, objectives, initiation, timing, progress and results of current and future preclinical studies and clinical trials of our product candidates, including the ongoing Phase 2 clinical trial for TX45, in Group 2 Pulmonary Hypertension; the expected timing of program updates and data disclosures; the timing of filing INDs and other regulatory documents; the competitive landscape for and market potential of our product candidates; and the potential properties and benefits of TX45. These forward-looking statements reflect our current beliefs and expectations. Many factors may cause differences between current expectations and actual results, including the early stage of our development efforts; success in preclinical testing and earlier clinical trials does not ensure that later clinical trials will generate the same results or otherwise provide adequate data to demonstrate the efficacy and safety of a product candidates; clinical site activation rates or clinical trial enrollment rates that are lower than expected; changes in expected or existing competition; changes in the regulatory environment; the uncertainties and timing of the regulatory approval process; the impact of macroeconomic conditions, including the conflict in Ukraine and the conflict in the Middle East, heightened inflation and uncertain credit and financial markets, on our business, clinical trials and financial position; and unexpected litigation or other disputes. These and other risks are described more fully in our filings with the Securities and Exchange Commission (“SEC”), including the risks detailed in our Quarterly Report on Form 10-Q filed with the SEC on August 7, 2025, and other documents we subsequently filed with or furnished to the SEC. All forward-looking statements contained in this presentation speak only as of the date on which they were made. Except as required by law, we assume no obligation to update any forward-looking statements contained herein to reflect any change in expectations, even as new information becomes available. This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size and growth and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates. Neither we nor any other person makes any representation as to the accuracy or completeness of such data or undertakes any obligation to update such data after the date of this presentation. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk.
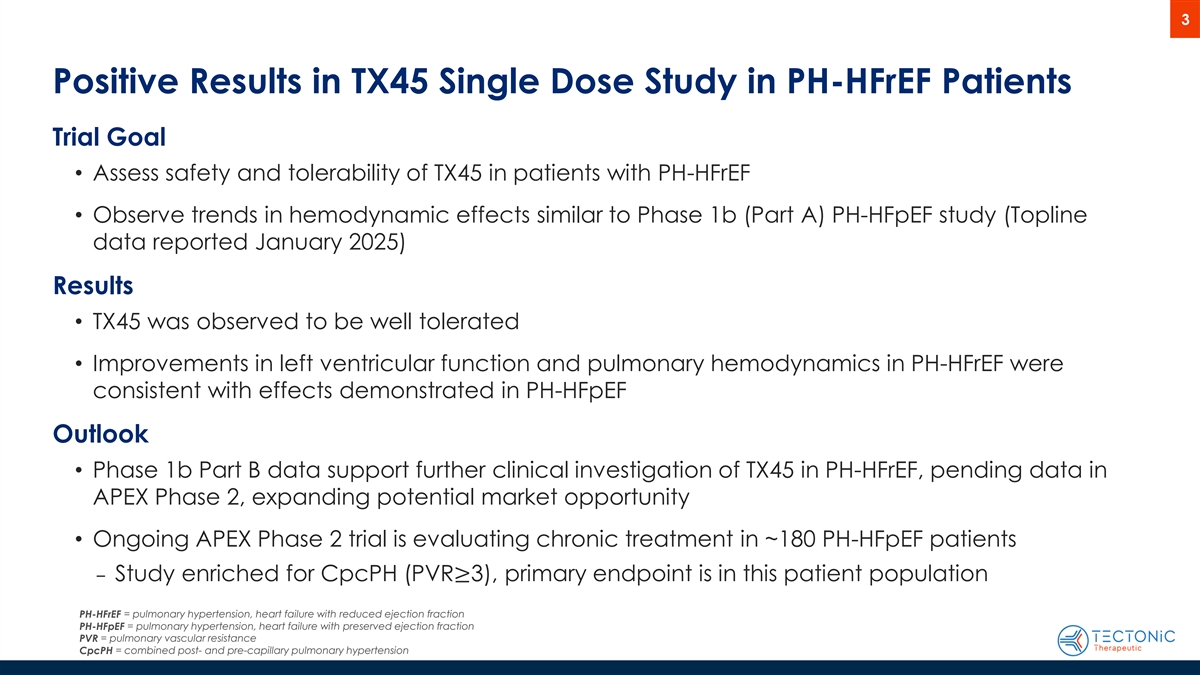
3 Positive Results in TX45 Single Dose Study in PH-HFrEF Patients Trial Goal • Assess safety and tolerability of TX45 in patients with PH-HFrEF • Observe trends in hemodynamic effects similar to Phase 1b (Part A) PH-HFpEF study (Topline data reported January 2025) Results • TX45 was observed to be well tolerated • Improvements in left ventricular function and pulmonary hemodynamics in PH-HFrEF were consistent with effects demonstrated in PH-HFpEF Outlook • Phase 1b Part B data support further clinical investigation of TX45 in PH-HFrEF, pending data in APEX Phase 2, expanding potential market opportunity • Ongoing APEX Phase 2 trial is evaluating chronic treatment in ~180 PH-HFpEF patients ‒ Study enriched for CpcPH (PVR≥3), primary endpoint is in this patient population PH-HFrEF = pulmonary hypertension, heart failure with reduced ejection fraction PH-HFpEF = pulmonary hypertension, heart failure with preserved ejection fraction = pulmonary vascular resistance PVR CpcPH = combined post- and pre-capillary pulmonary hypertension
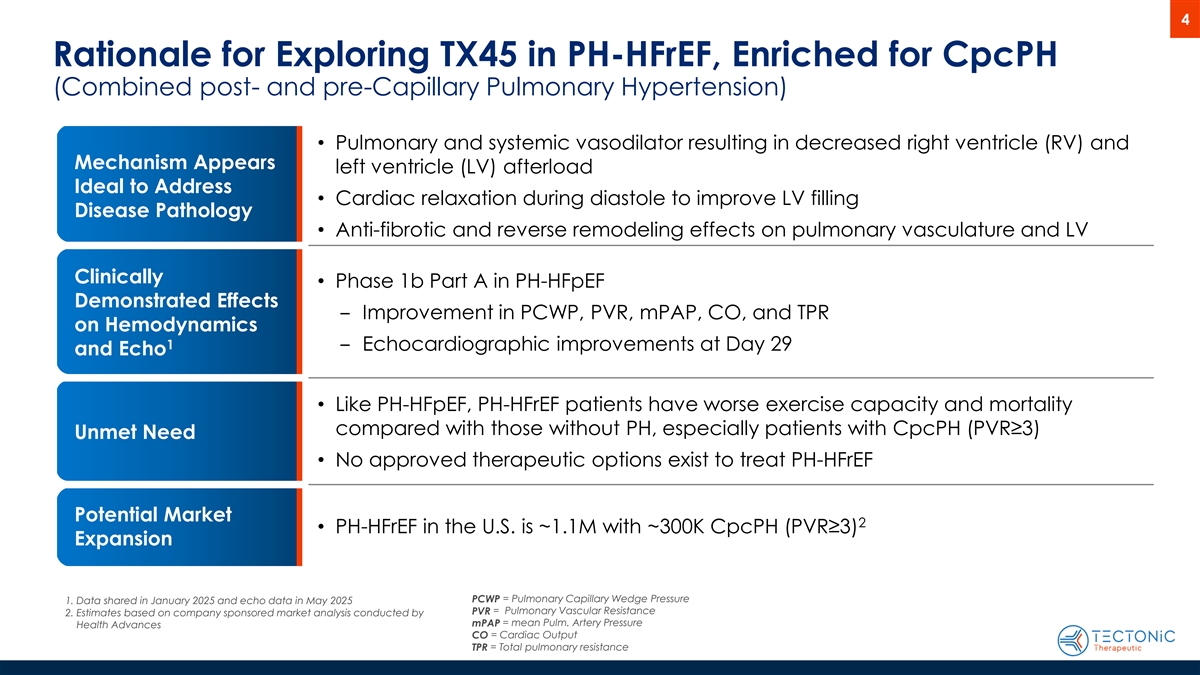
4 Rationale for Exploring TX45 in PH-HFrEF, Enriched for CpcPH (Combined post- and pre-Capillary Pulmonary Hypertension) • Pulmonary and systemic vasodilator resulting in decreased right ventricle (RV) and Mechanism Appears left ventricle (LV) afterload Ideal to Address • Cardiac relaxation during diastole to improve LV filling Disease Pathology • Anti-fibrotic and reverse remodeling effects on pulmonary vasculature and LV Clinically • Phase 1b Part A in PH-HFpEF Demonstrated Effects ‒ Improvement in PCWP, PVR, mPAP, CO, and TPR on Hemodynamics 1 ‒ Echocardiographic improvements at Day 29 and Echo • Like PH-HFpEF, PH-HFrEF patients have worse exercise capacity and mortality compared with those without PH, especially patients with CpcPH (PVR≥3) Unmet Need • No approved therapeutic options exist to treat PH-HFrEF Potential Market 2 • PH-HFrEF in the U.S. is ~1.1M with ~300K CpcPH (PVR≥3) Expansion PCWP = Pulmonary Capillary Wedge Pressure 1. Data shared in January 2025 and echo data in May 2025 PVR = Pulmonary Vascular Resistance 2. Estimates based on company sponsored market analysis conducted by mPAP = mean Pulm. Artery Pressure Health Advances CO = Cardiac Output TPR = Total pulmonary resistance
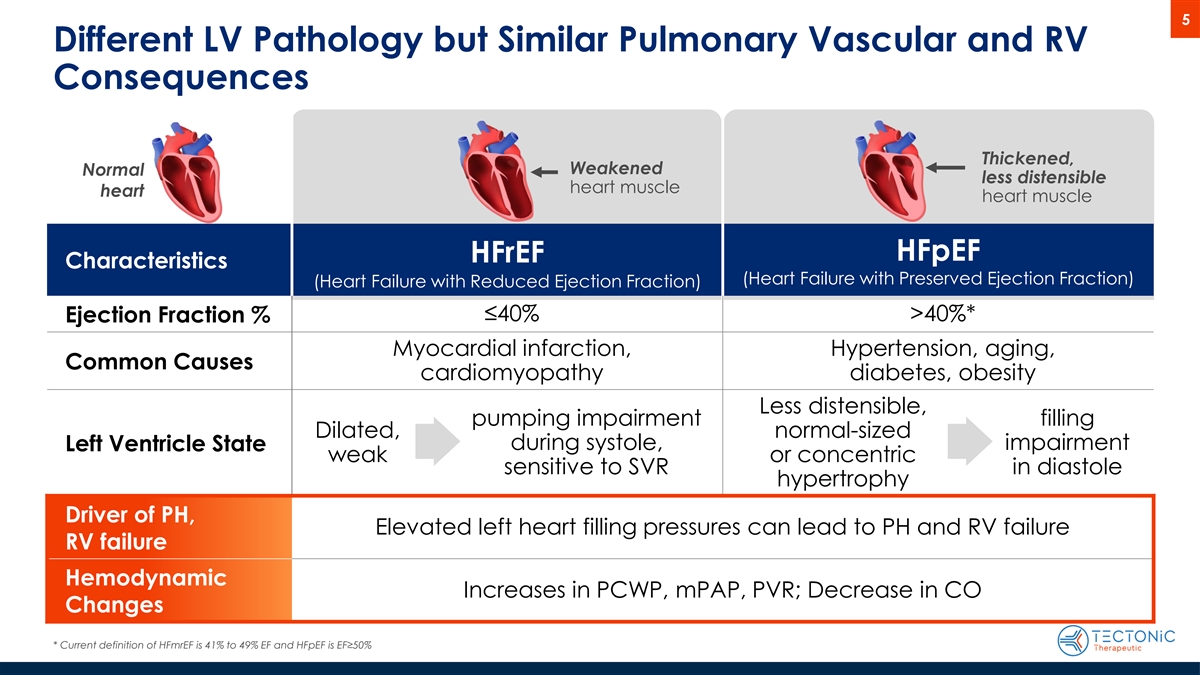
5 Different LV Pathology but Similar Pulmonary Vascular and RV Consequences Thickened, Weakened Normal less distensible heart muscle heart heart muscle HFpEF HFrEF Characteristics (Heart Failure with Preserved Ejection Fraction) (Heart Failure with Reduced Ejection Fraction) ≤40% >40%* Ejection Fraction % Myocardial infarction, Hypertension, aging, Common Causes cardiomyopathy diabetes, obesity Less distensible, pumping impairment filling Dilated, normal-sized during systole, impairment Left Ventricle State weak or concentric sensitive to SVR in diastole hypertrophy Driver of PH, Elevated left heart filling pressures can lead to PH and RV failure RV failure Hemodynamic Increases in PCWP, mPAP, PVR; Decrease in CO Changes * Current definition of HFmrEF is 41% to 49% EF and HFpEF is EF≥50%
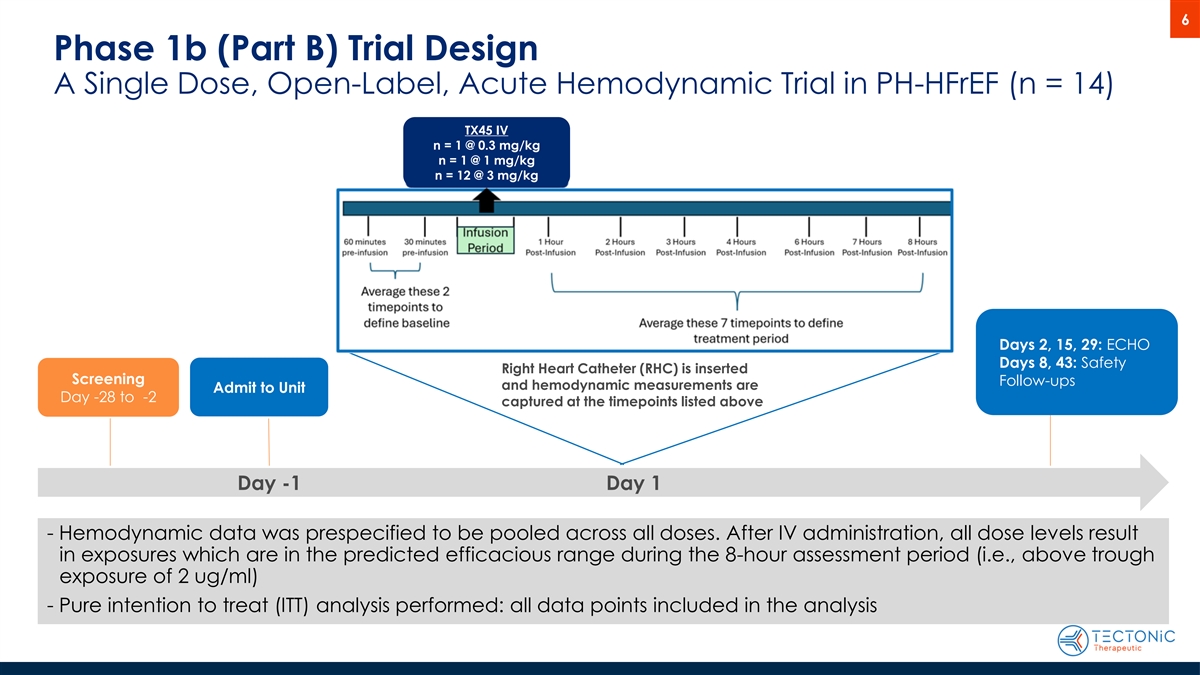
6 Phase 1b (Part B) Trial Design A Single Dose, Open-Label, Acute Hemodynamic Trial in PH-HFrEF (n = 14) TX45 IV n = 1 @ 0.3 mg/kg n = 1 @ 1 mg/kg n = 12 @ 3 mg/kg Days 2, 15, 29: ECHO Days 8, 43: Safety Right Heart Catheter (RHC) is inserted Screening Follow-ups and hemodynamic measurements are Admit to Unit Day -28 to -2 captured at the timepoints listed above Day -1 Day 1 - Hemodynamic data was prespecified to be pooled across all doses. After IV administration, all dose levels result in exposures which are in the predicted efficacious range during the 8-hour assessment period (i.e., above trough exposure of 2 ug/ml) - Pure intention to treat (ITT) analysis performed: all data points included in the analysis
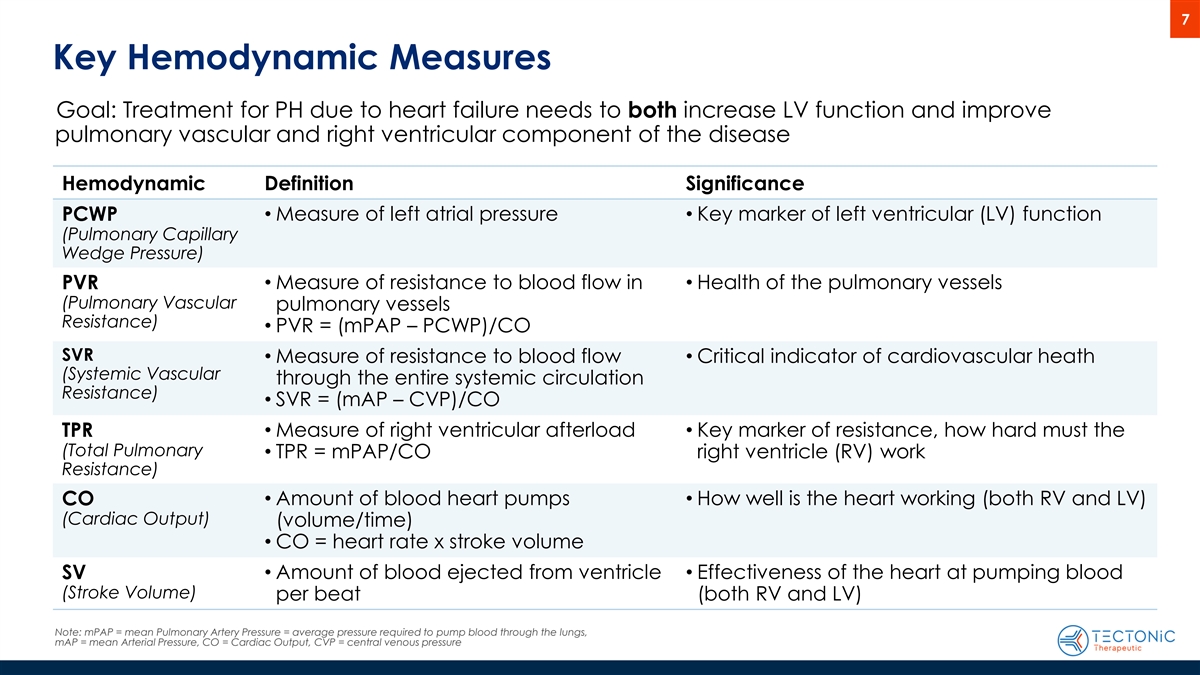
7 Key Hemodynamic Measures Goal: Treatment for PH due to heart failure needs to both increase LV function and improve pulmonary vascular and right ventricular component of the disease Hemodynamic Definition Significance PCWP• Measure of left atrial pressure• Key marker of left ventricular (LV) function (Pulmonary Capillary Wedge Pressure) • Measure of resistance to blood flow in • Health of the pulmonary vessels PVR (Pulmonary Vascular pulmonary vessels Resistance) • PVR = (mPAP – PCWP)/CO SVR • Measure of resistance to blood flow • Critical indicator of cardiovascular heath (Systemic Vascular through the entire systemic circulation Resistance) • SVR = (mAP – CVP)/CO TPR• Measure of right ventricular afterload• Key marker of resistance, how hard must the (Total Pulmonary • TPR = mPAP/CO right ventricle (RV) work Resistance) CO• Amount of blood heart pumps • How well is the heart working (both RV and LV) (Cardiac Output) (volume/time) • CO = heart rate x stroke volume SV• Amount of blood ejected from ventricle • Effectiveness of the heart at pumping blood (Stroke Volume) per beat (both RV and LV) Note: mPAP = mean Pulmonary Artery Pressure = average pressure required to pump blood through the lungs, mAP = mean Arterial Pressure, CO = Cardiac Output, CVP = central venous pressure
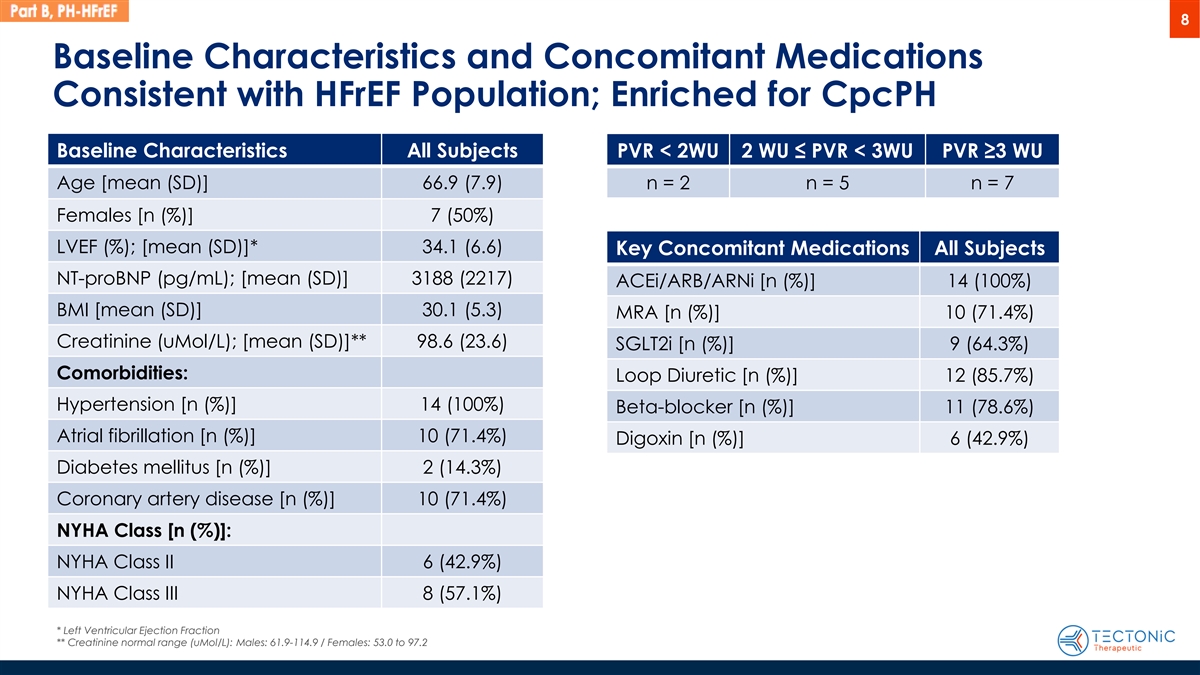
8 Baseline Characteristics and Concomitant Medications Consistent with HFrEF Population; Enriched for CpcPH Baseline Characteristics All Subjects PVR < 2WU 2 WU ≤ PVR < 3WU PVR ≥3 WU Age [mean (SD)] 66.9 (7.9) n = 2 n = 5 n = 7 Females [n (%)] 7 (50%) LVEF (%); [mean (SD)]* 34.1 (6.6) Key Concomitant Medications All Subjects NT-proBNP (pg/mL); [mean (SD)] 3188 (2217) ACEi/ARB/ARNi [n (%)] 14 (100%) BMI [mean (SD)] 30.1 (5.3) MRA [n (%)] 10 (71.4%) Creatinine (uMol/L); [mean (SD)]** 98.6 (23.6) SGLT2i [n (%)] 9 (64.3%) Comorbidities: Loop Diuretic [n (%)] 12 (85.7%) Hypertension [n (%)] 14 (100%) Beta-blocker [n (%)] 11 (78.6%) Atrial fibrillation [n (%)] 10 (71.4%) Digoxin [n (%)] 6 (42.9%) Diabetes mellitus [n (%)] 2 (14.3%) Coronary artery disease [n (%)] 10 (71.4%) NYHA Class [n (%)]: NYHA Class II 6 (42.9%) NYHA Class III 8 (57.1%) * Left Ventricular Ejection Fraction ** Creatinine normal range (uMol/L): Males: 61.9-114.9 / Females: 53.0 to 97.2
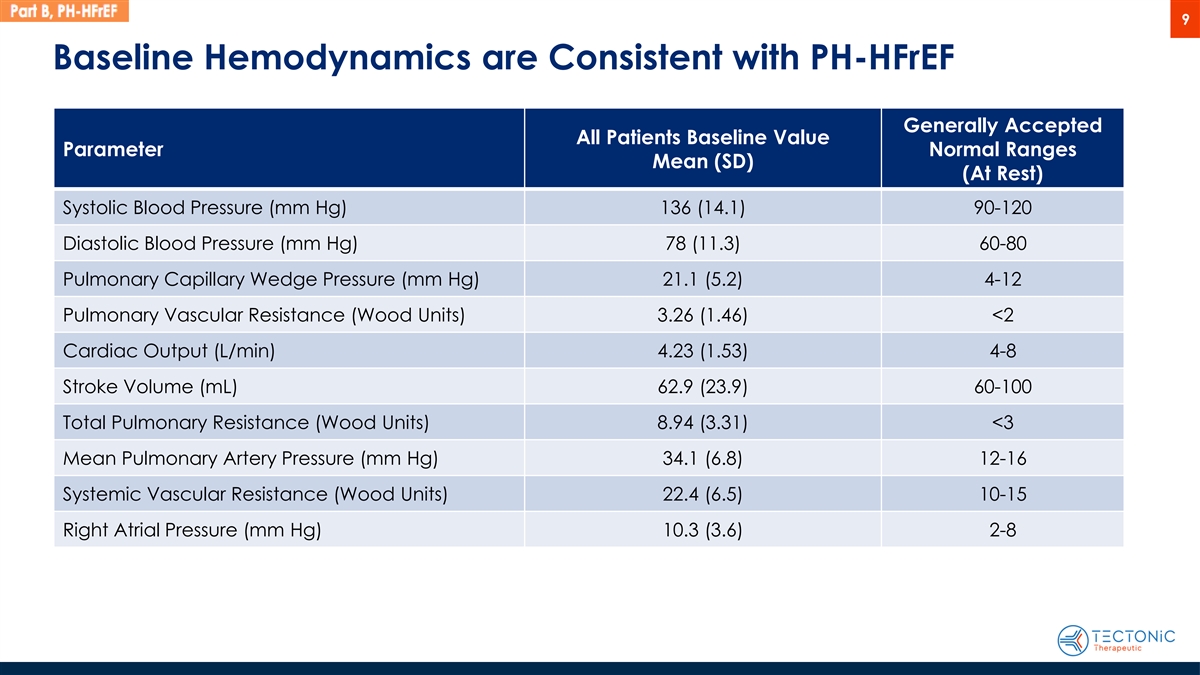
9 Baseline Hemodynamics are Consistent with PH-HFrEF Generally Accepted All Patients Baseline Value Parameter Normal Ranges Mean (SD) (At Rest) Systolic Blood Pressure (mm Hg) 136 (14.1) 90-120 Diastolic Blood Pressure (mm Hg) 78 (11.3) 60-80 Pulmonary Capillary Wedge Pressure (mm Hg) 21.1 (5.2) 4-12 Pulmonary Vascular Resistance (Wood Units) 3.26 (1.46) <2 Cardiac Output (L/min) 4.23 (1.53) 4-8 Stroke Volume (mL) 62.9 (23.9) 60-100 Total Pulmonary Resistance (Wood Units) 8.94 (3.31) <3 Mean Pulmonary Artery Pressure (mm Hg) 34.1 (6.8) 12-16 Systemic Vascular Resistance (Wood Units) 22.4 (6.5) 10-15 Right Atrial Pressure (mm Hg) 10.3 (3.6) 2-8
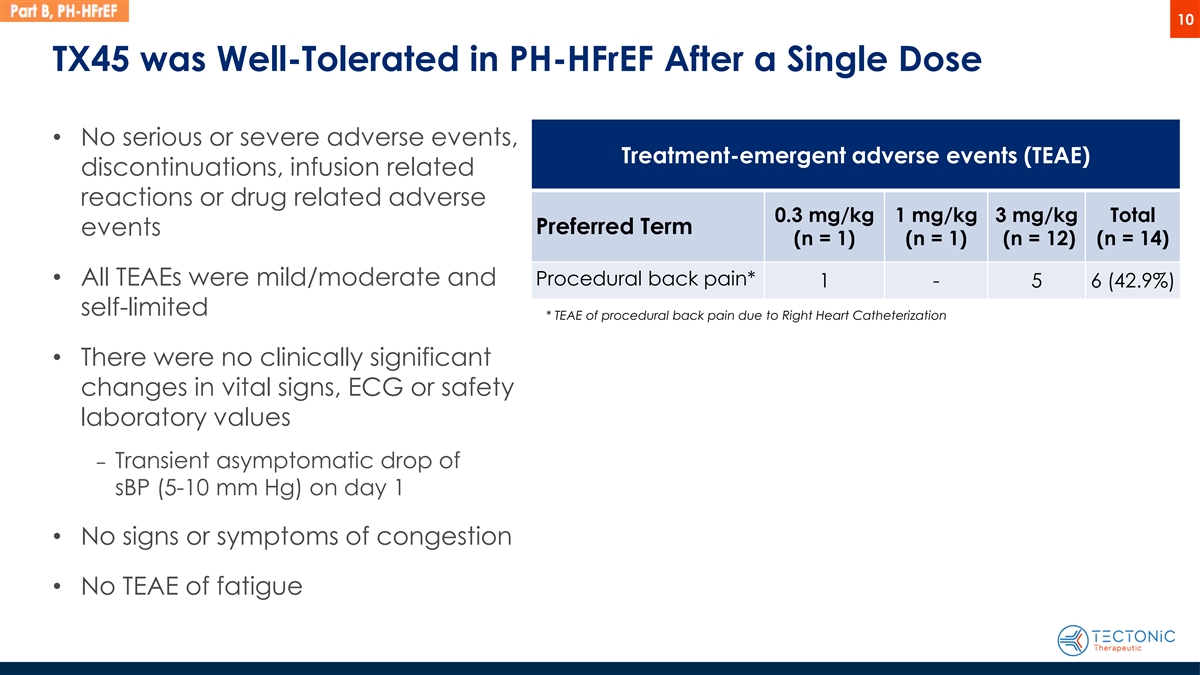
10 TX45 was Well-Tolerated in PH-HFrEF After a Single Dose • No serious or severe adverse events, Treatment-emergent adverse events (TEAE) discontinuations, infusion related reactions or drug related adverse 0.3 mg/kg 1 mg/kg 3 mg/kg Total Preferred Term events (n = 1) (n = 1) (n = 12) (n = 14) • All TEAEs were mild/moderate and Procedural back pain* 1 - 5 6 (42.9%) self-limited * TEAE of procedural back pain due to Right Heart Catheterization • There were no clinically significant changes in vital signs, ECG or safety laboratory values ‒ Transient asymptomatic drop of sBP (5-10 mm Hg) on day 1 • No signs or symptoms of congestion • No TEAE of fatigue
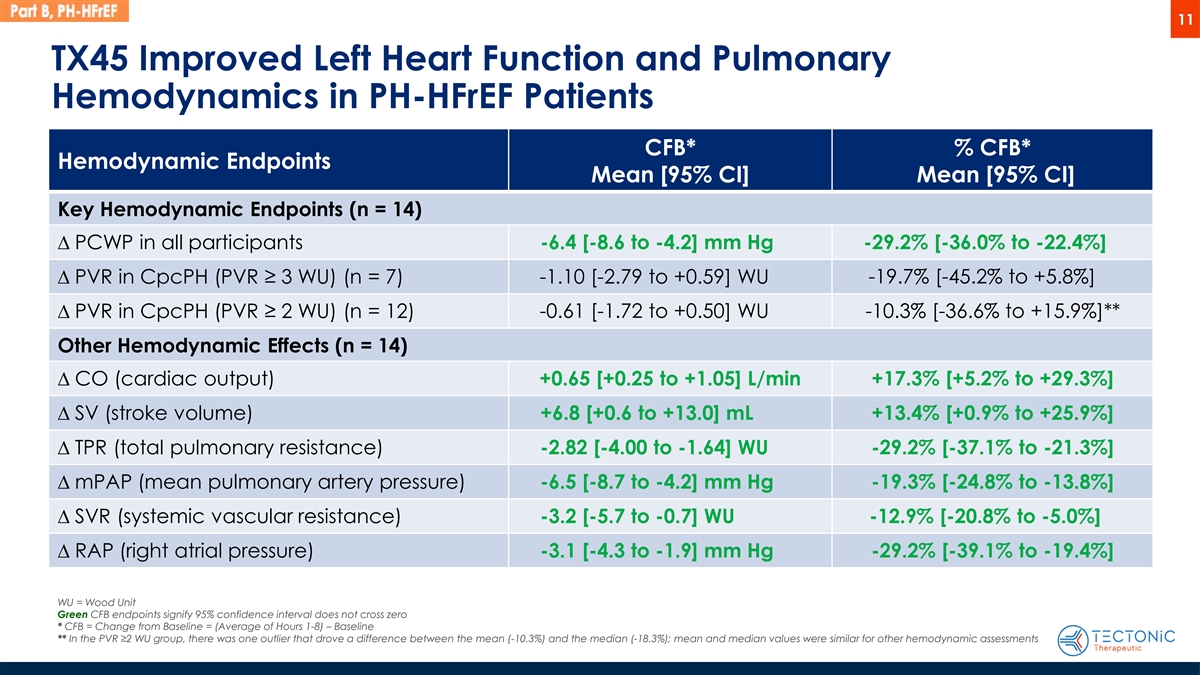
11 TX45 Improved Left Heart Function and Pulmonary Hemodynamics in PH-HFrEF Patients CFB* % CFB* Hemodynamic Endpoints Mean [95% CI] Mean [95% CI] Key Hemodynamic Endpoints (n = 14) D PCWP in all participants -6.4 [-8.6 to -4.2] mm Hg -29.2% [-36.0% to -22.4%] D PVR in CpcPH (PVR ≥ 3 WU) (n = 7) -1.10 [-2.79 to +0.59] WU -19.7% [-45.2% to +5.8%] -0.61 [-1.72 to +0.50] WU -10.3% [-36.6% to +15.9%]** D PVR in CpcPH (PVR ≥ 2 WU) (n = 12) Other Hemodynamic Effects (n = 14) D CO (cardiac output) +0.65 [+0.25 to +1.05] L/min +17.3% [+5.2% to +29.3%] D SV (stroke volume) +6.8 [+0.6 to +13.0] mL +13.4% [+0.9% to +25.9%] D TPR (total pulmonary resistance) -2.82 [-4.00 to -1.64] WU -29.2% [-37.1% to -21.3%] D mPAP (mean pulmonary artery pressure) -6.5 [-8.7 to -4.2] mm Hg -19.3% [-24.8% to -13.8%] D SVR (systemic vascular resistance) -3.2 [-5.7 to -0.7] WU -12.9% [-20.8% to -5.0%] D RAP (right atrial pressure) -3.1 [-4.3 to -1.9] mm Hg -29.2% [-39.1% to -19.4%] WU = Wood Unit Green CFB endpoints signify 95% confidence interval does not cross zero * CFB = Change from Baseline = (Average of Hours 1-8) – Baseline ** In the PVR ≥2 WU group, there was one outlier that drove a difference between the mean (-10.3%) and the median (-18.3%); mean and median values were similar for other hemodynamic assessments
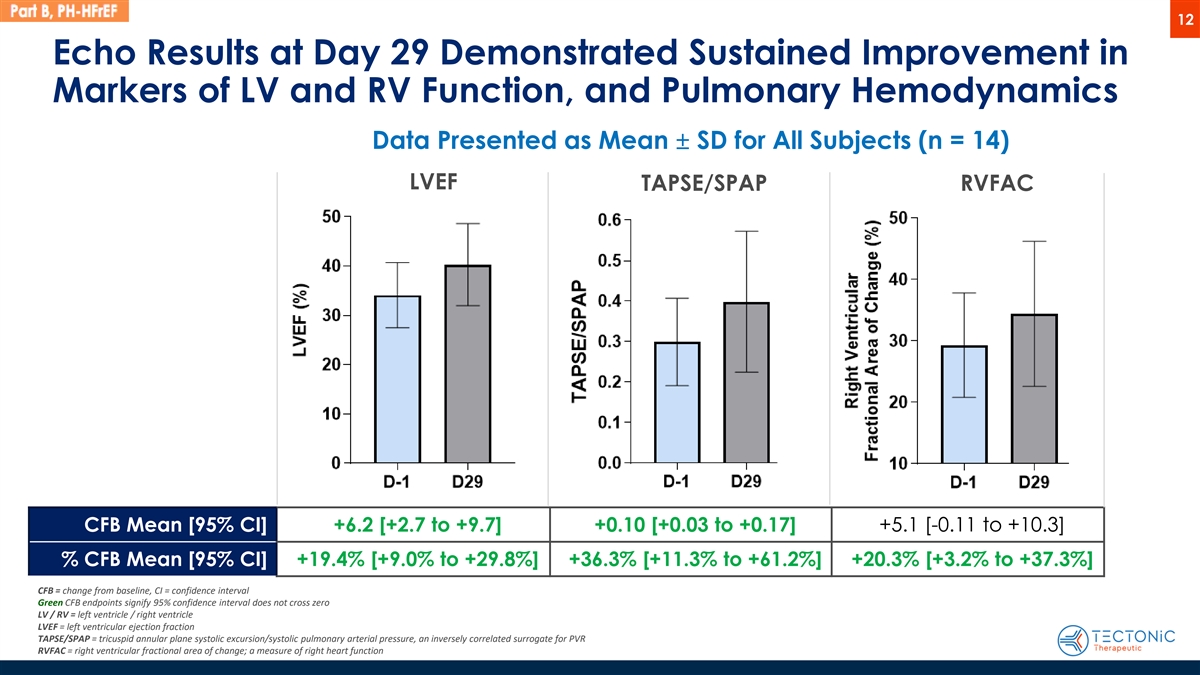
12 Echo Results at Day 29 Demonstrated Sustained Improvement in Markers of LV and RV Function, and Pulmonary Hemodynamics Data Presented as Mean ± SD for All Subjects (n = 14) LVEF TAPSE/SPAP RVFAC CFB Mean [95% CI] +6.2 [+2.7 to +9.7] +0.10 [+0.03 to +0.17] +5.1 [-0.11 to +10.3] % CFB Mean [95% CI] +19.4% [+9.0% to +29.8%] +36.3% [+11.3% to +61.2%] +20.3% [+3.2% to +37.3%] CFB = change from baseline, CI = confidence interval Green CFB endpoints signify 95% confidence interval does not cross zero LV / RV = left ventricle / right ventricle LVEF = left ventricular ejection fraction TAPSE/SPAP = tricuspid annular plane systolic excursion/systolic pulmonary arterial pressure, an inversely correlated surrogate for PVR RVFAC = right ventricular fractional area of change; a measure of right heart function
13 Summary: TX45 Improves Cardiac and Pulmonary Hemodynamics in PH-HFrEF and PH-HFpEF Patients • TX45 was well-tolerated in both patient populations • TX45 demonstrated hemodynamic improvements in both left heart function and in the pulmonary vasculature in PH-HFrEF, consistent with effects in PH-HFpEF ‒ Acute improvement in left ventricular hemodynamics and pulmonary vascular / RV hemodynamics (PCWP, CO, PVR, TPR, mPAP) ‒ Echocardiographic improvements at Day 29 (LVEF, TAPSE/SPAP, RVFAC) ‒ The magnitude of the reduction in PCWP and PVR, demonstrated in our HFpEF and HFrEF 1-3 cohorts, have been associated with meaningful changes in 6MWD in previous studies ‒ Right ventricular afterload, as assessed by TPR, was reduced. Reduced RV afterload has been associated with improved mortality and outcomes in cohort studies of patients with 4 Group 2 PH • Results support future expansion of TX45’s addressable Group 2 PH patient population to PH-HFrEF, pending results of ongoing APEX Phase 2 clinical trial 1. Lewis GD et al. Circ. Heart Failure 2023 2. Lewis GD et al. Circulation 2007 3. Zhang H et al. JACC Cardiovasc. Interv. 2019 4. Tampakakis,, Circ Heart Failure, 2018