Exhibit T3A-20
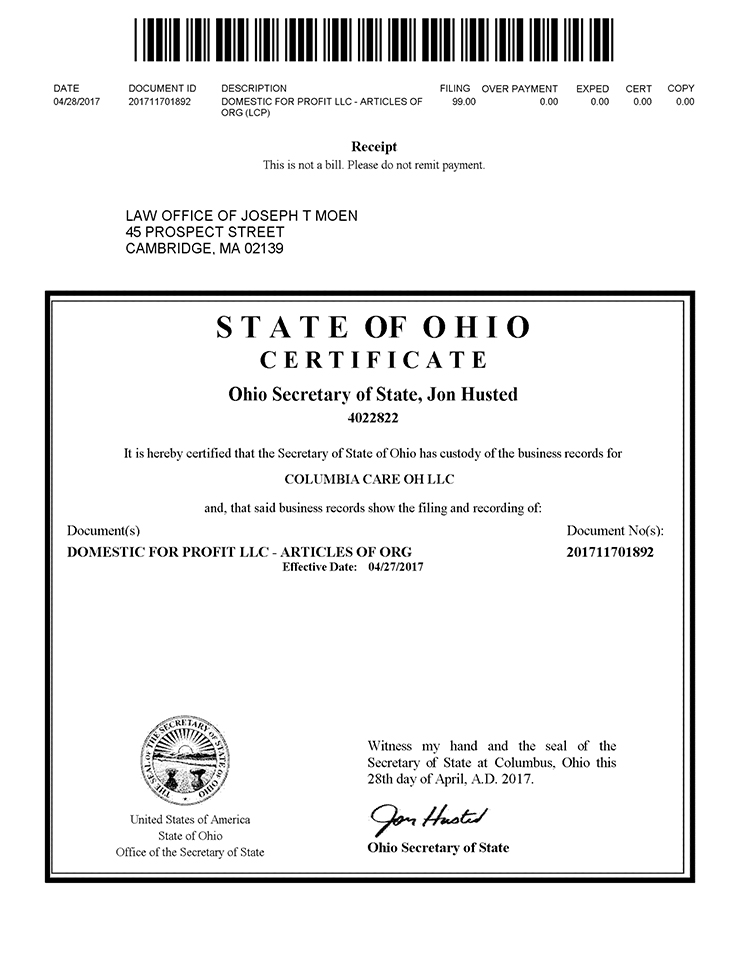
Doc ID -- 201711701892
Doc ID —> 201711701892 DATE DOCUMENT ID DESCRIPTION FILING OVER PAYMENT EXPED CERT COPY 04/28/2017 201711701892 DOMESTIC FOR PROFIT LLC- ARTICLES OF 99.00 0.00 0.00 0.00 0.00 ORG (LCP) Receipt This is not a bill. Please do not remit payment LAW OFFICE OF JOSEPH T MOEN 45 PROSPECT STREET CAMBRIDGE, MA 02139 S T A T E OF 0 HI 0 CERTIFICATE Ohio Secretary of State, Jon Husted 4022822 It is hereby certified that the Secretary of State of Ohio has custody of the business records for COLUMBIA CARE OH LLC and, that said business records show the tlling and recording of: Document( s) DOMESTIC ‘FOR PRUFIT LLC ARTICLES OF’ ORG Effective Date: 04/27/2017 Document No(s): 201711701892 United States of America State of Ohio Office of the Secretary of State Witness my hand and the seal of the Secretary of State at Columbus, Ohio this 28th day of April, A.D. 2017. Ohio Secretary of State
Page 1