| Precision Oncology Through Synthetic Lethality August 2025 |
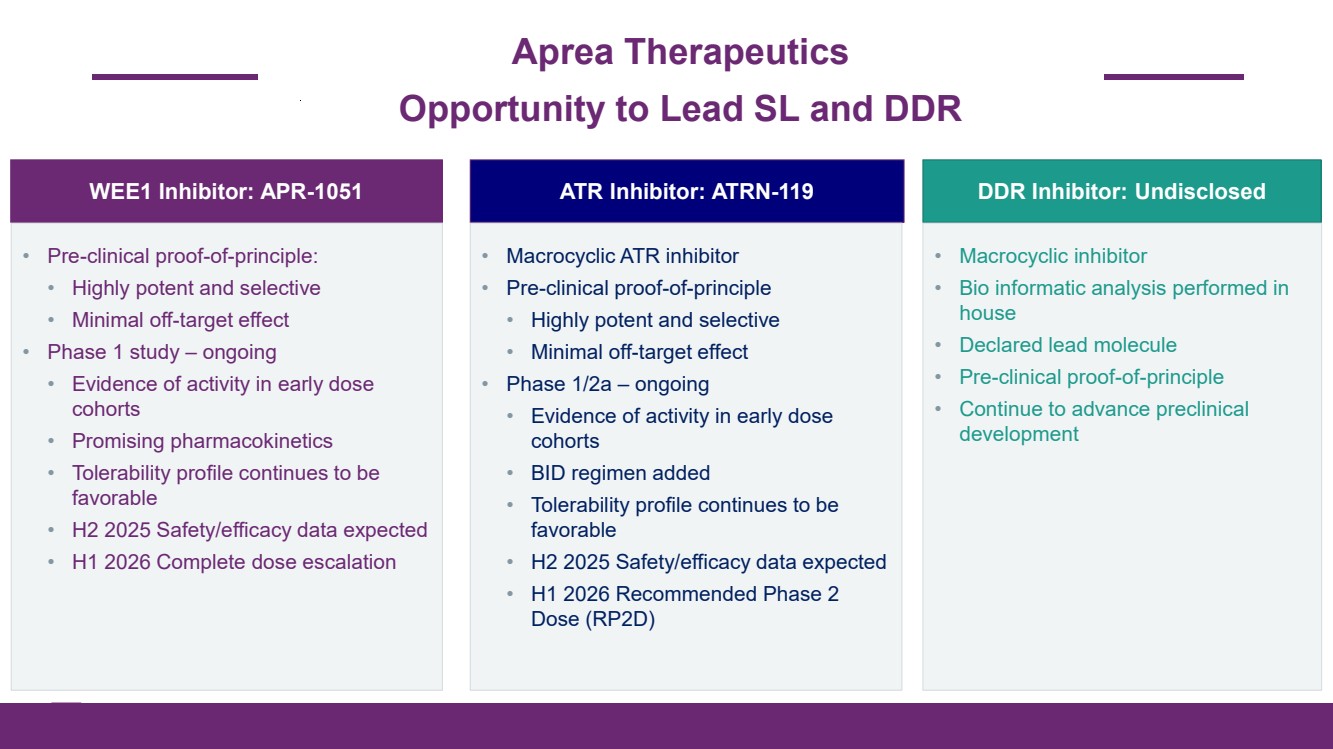
| 2 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Aprea Therapeutics Opportunity to Lead SL and DDR WEE1 Inhibitor: APR-1051 • Pre-clinical proof-of-principle: • Highly potent and selective • Minimal off-target effect • Phase 1 study – ongoing • Evidence of activity in early dose cohorts • Promising pharmacokinetics • Tolerability profile continues to be favorable • H2 2025 Safety/efficacy data expected • H1 2026 Complete dose escalation ATR Inhibitor: ATRN-119 • Macrocyclic ATR inhibitor • Pre-clinical proof-of-principle • Highly potent and selective • Minimal off-target effect • Phase 1/2a – ongoing • Evidence of activity in early dose cohorts • BID regimen added • Tolerability profile continues to be favorable • H2 2025 Safety/efficacy data expected • H1 2026 Recommended Phase 2 Dose (RP2D) DDR Inhibitor: Undisclosed • Macrocyclic inhibitor • Bio informatic analysis performed in house • Declared lead molecule • Pre-clinical proof-of-principle • Continue to advance preclinical development |
| 3 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Forward-Looking Statements Certain information contained in this presentation includes “forward-looking statements”, within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended related to our study analyses, clinical trials, regulatory submissions, and projected cash position. We may, in some cases use terms such as “future,” “predicts,” “believes,” “potential,” “continue,” “anticipates,” “estimates,” “expects,” “plans,” “intends,” “targeting,” “confidence,” “may,” “could,” “might,” “likely,” “will,” “should” or other words that convey uncertainty of the future events or outcomes to identify these forward-looking statements. Our forward-looking statements are based on current beliefs and expectations of our management team and on information currently available to management that involve risks, potential changes in circumstances, assumptions, and uncertainties. All statements contained in this presentation other than statements of historical fact are forward-looking statements, including statements regarding our ability to develop, commercialize, and achieve market acceptance of our current and planned products and services, our research and development efforts, including timing considerations and other matters regarding our business strategies, use of capital, results of operations and financial position, and plans and objectives for future operations. Any or all of the forward-looking statements may turn out to be wrong or be affected by inaccurate assumptions we might make or by known or unknown risks and uncertainties. These forward-looking statements are subject to risks and uncertainties including, without limitation, risks related to the success, timing, and cost of our ongoing clinical trials and anticipated clinical trials for our current product candidates, including statements regarding the timing of initiation, pace of enrollment and completion of the trials (including our ability to fully fund our disclosed clinical trials, which assumes no material changes to our currently projected expenses), futility analyses, presentations at conferences and data reported in an abstract, and receipt of interim or preliminary results (including, without limitation, any preclinical results or data), which are not necessarily indicative of the final results of our ongoing clinical trials, our understanding of product candidates mechanisms of action and interpretation of preclinical and early clinical results from its clinical development programs, our ability to continue as a going concern, and the other risks, uncertainties, and other factors described under “Risk Factors,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in the documents we file with the U.S. Securities and Exchange Commission. For all these reasons, actual results and developments could be materially different from those expressed in or implied by our forward-looking statements. You are cautioned not to place undue reliance on these forward-looking statements, which are made only as of the date of this presentation. We undertake no obligation to update such forward-looking statements for any reason, except as required by law. |
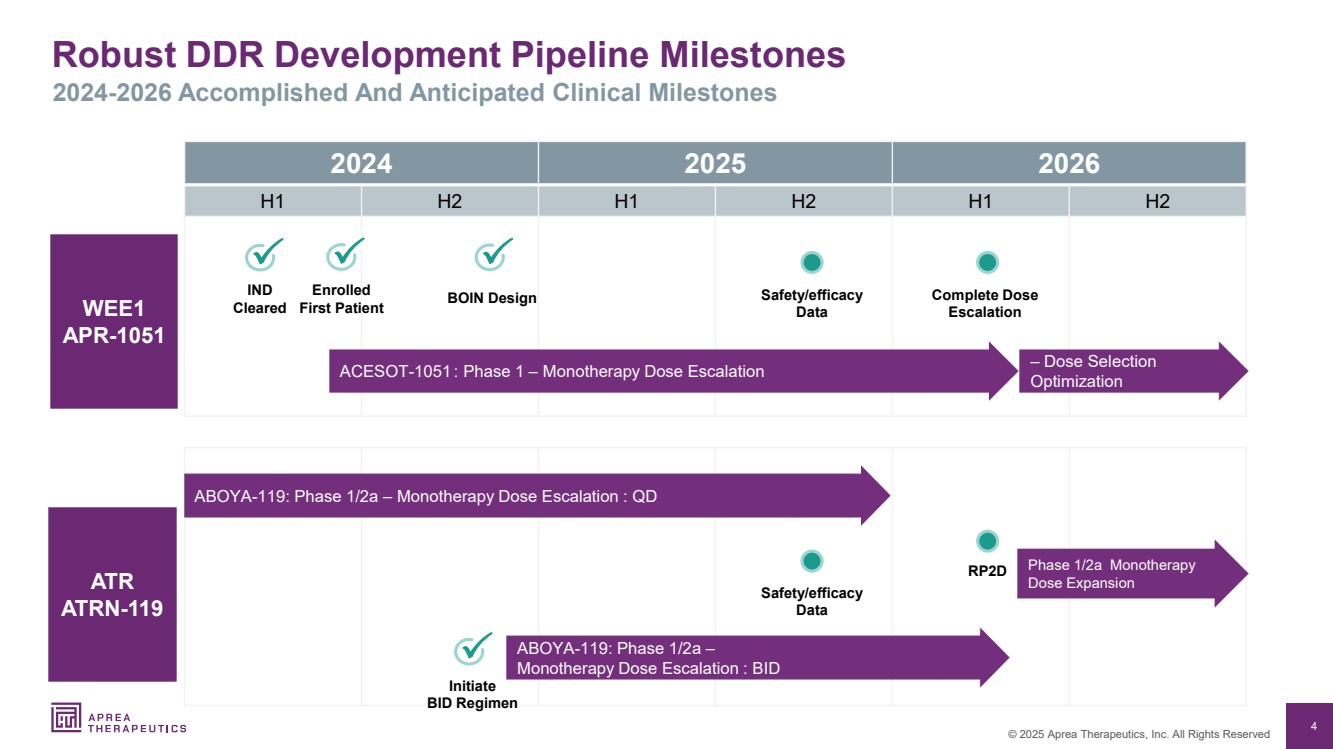
| 4 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Robust DDR Development Pipeline Milestones 2024-2026 Accomplished And Anticipated Clinical Milestones 2024 2025 2026 H1 H2 H1 H2 H1 H2 ATR ATRN-119 WEE1 APR-1051 RP2D ACESOT-1051 : Phase 1 – Monotherapy Dose Escalation Enrolled First Patient Complete Dose Escalation Safety/efficacy Data IND Cleared Phase 1/2a Monotherapy Dose Expansion ABOYA-119: Phase 1/2a – Monotherapy Dose Escalation : QD BOIN Design Initiate BID Regimen – Dose Selection Optimization ABOYA-119: Phase 1/2a – Monotherapy Dose Escalation : BID Safety/efficacy Data |
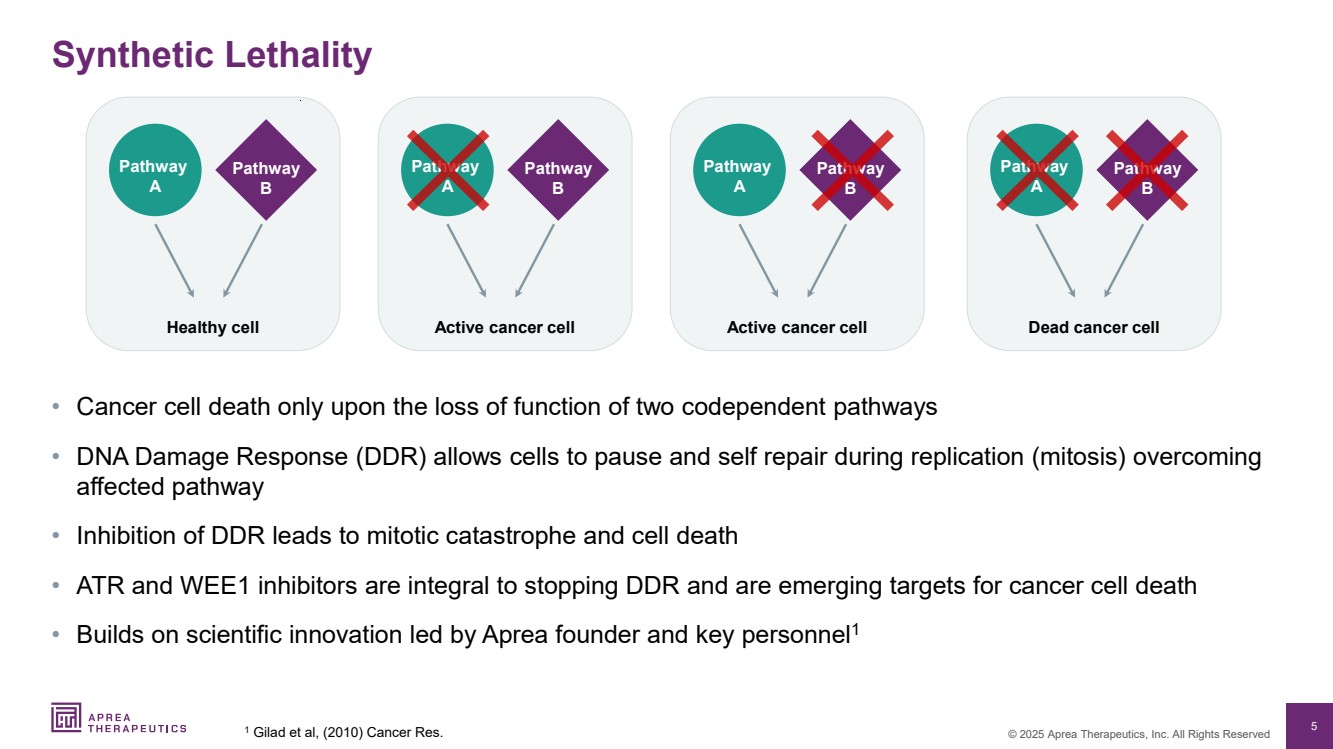
| 5 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Synthetic Lethality • Cancer cell death only upon the loss of function of two codependent pathways • DNA Damage Response (DDR) allows cells to pause and self repair during replication (mitosis) overcoming affected pathway • Inhibition of DDR leads to mitotic catastrophe and cell death • ATR and WEE1 inhibitors are integral to stopping DDR and are emerging targets for cancer cell death • Builds on scientific innovation led by Aprea founder and key personnel1 1 Gilad et al, (2010) Cancer Res. Healthy cell Pathway A Pathway B Active cancer cell Pathway A Pathway B Dead cancer cell Pathway A Pathway B Active cancer cell Pathway A Pathway B |
| 6 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Strong Drug Development and Commercial Expertise Leaders in Synthetic Lethality and Targeted Therapy Management Board of Directors Richard Peters, M.D., Ph.D. Chairman of the Board Oren Gilad, Ph.D. President and CEO Jean-Pierre Bizzari, M.D. Director Marc Duey Director Michael Grissinger Director Gabriela Gruia, M.D. Director John Henneman Director Rifat Pamukcu, M.D. Director Bernd R. Seizinger, M.D., Ph.D. Director Oren Gilad, Ph.D. President and CEO John P. Hamill Sr. Vice President and CFO Philippe Pultar, MD Sr. Medical Advisor Ze’ev Weiss, CPA, B.Sc. Chief Business Advisor Mike Carleton, Ph.D. Translational Medicine Advisor Brian Wiley SVP, Corporate Strategy |
| 7 © 2025 Aprea Therapeutics, Inc. All Rights Reserved WEE1 Inhibitor: APR-1051 |
| 8 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 8 WEE1 Inhibitor: APR-1051 ACESOT-1051: Clinical Proof-Of-Concept |
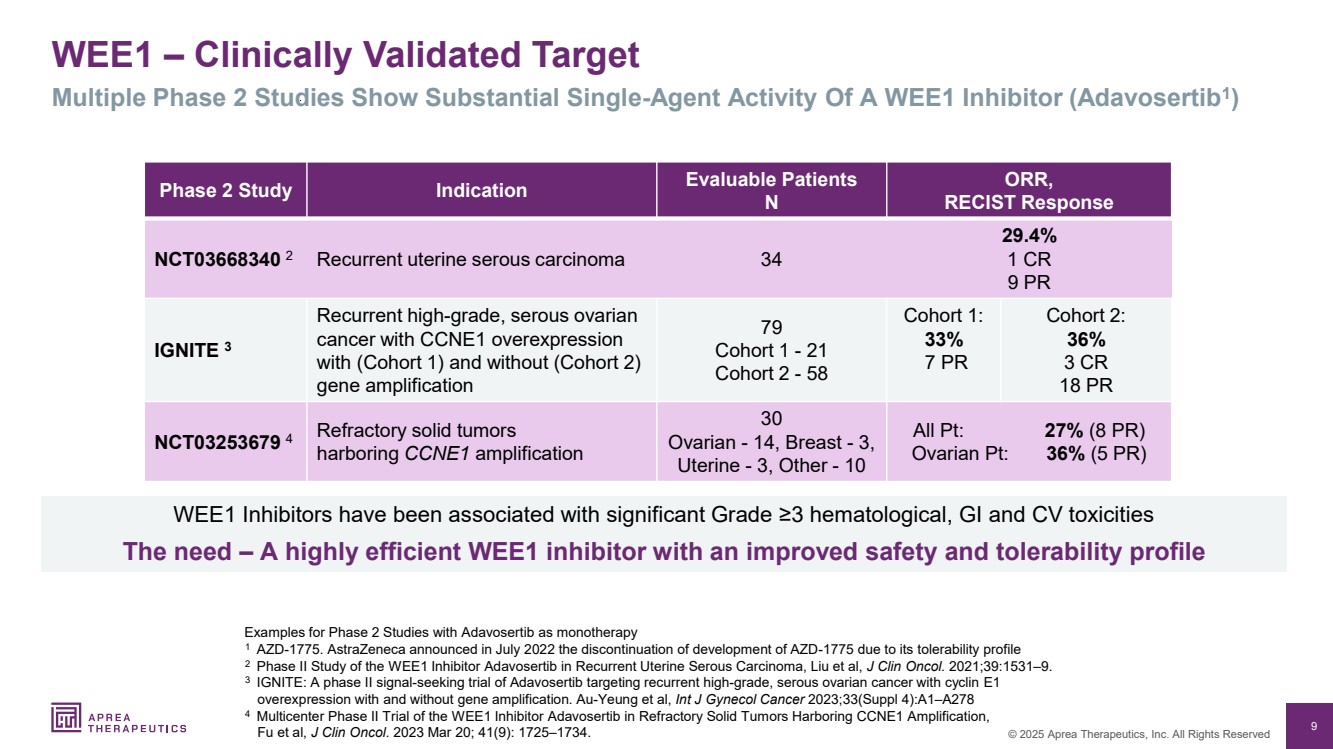
| 9 © 2025 Aprea Therapeutics, Inc. All Rights Reserved WEE1 – Clinically Validated Target Examples for Phase 2 Studies with Adavosertib as monotherapy 1 AZD-1775. AstraZeneca announced in July 2022 the discontinuation of development of AZD-1775 due to its tolerability profile 2 Phase II Study of the WEE1 Inhibitor Adavosertib in Recurrent Uterine Serous Carcinoma, Liu et al, J Clin Oncol. 2021;39:1531–9. 3 IGNITE: A phase II signal-seeking trial of Adavosertib targeting recurrent high-grade, serous ovarian cancer with cyclin E1 overexpression with and without gene amplification. Au-Yeung et al, Int J Gynecol Cancer 2023;33(Suppl 4):A1–A278 4 Multicenter Phase II Trial of the WEE1 Inhibitor Adavosertib in Refractory Solid Tumors Harboring CCNE1 Amplification, Fu et al, J Clin Oncol. 2023 Mar 20; 41(9): 1725–1734. Phase 2 Study Indication Evaluable Patients N ORR, RECIST Response NCT03668340 2 Recurrent uterine serous carcinoma 34 29.4% 1 CR 9 PR IGNITE 3 Recurrent high-grade, serous ovarian cancer with CCNE1 overexpression with (Cohort 1) and without (Cohort 2) gene amplification 79 Cohort 1 - 21 Cohort 2 - 58 Cohort 1: 33% 7 PR Cohort 2: 36% 3 CR 18 PR NCT03253679 4 Refractory solid tumors harboring CCNE1 amplification 30 Ovarian - 14, Breast - 3, Uterine - 3, Other - 10 All Pt: 27% (8 PR) Ovarian Pt: 36% (5 PR) Multiple Phase 2 Studies Show Substantial Single-Agent Activity Of A WEE1 Inhibitor (Adavosertib1 ) WEE1 Inhibitors have been associated with significant Grade ≥3 hematological, GI and CV toxicities The need – A highly efficient WEE1 inhibitor with an improved safety and tolerability profile |
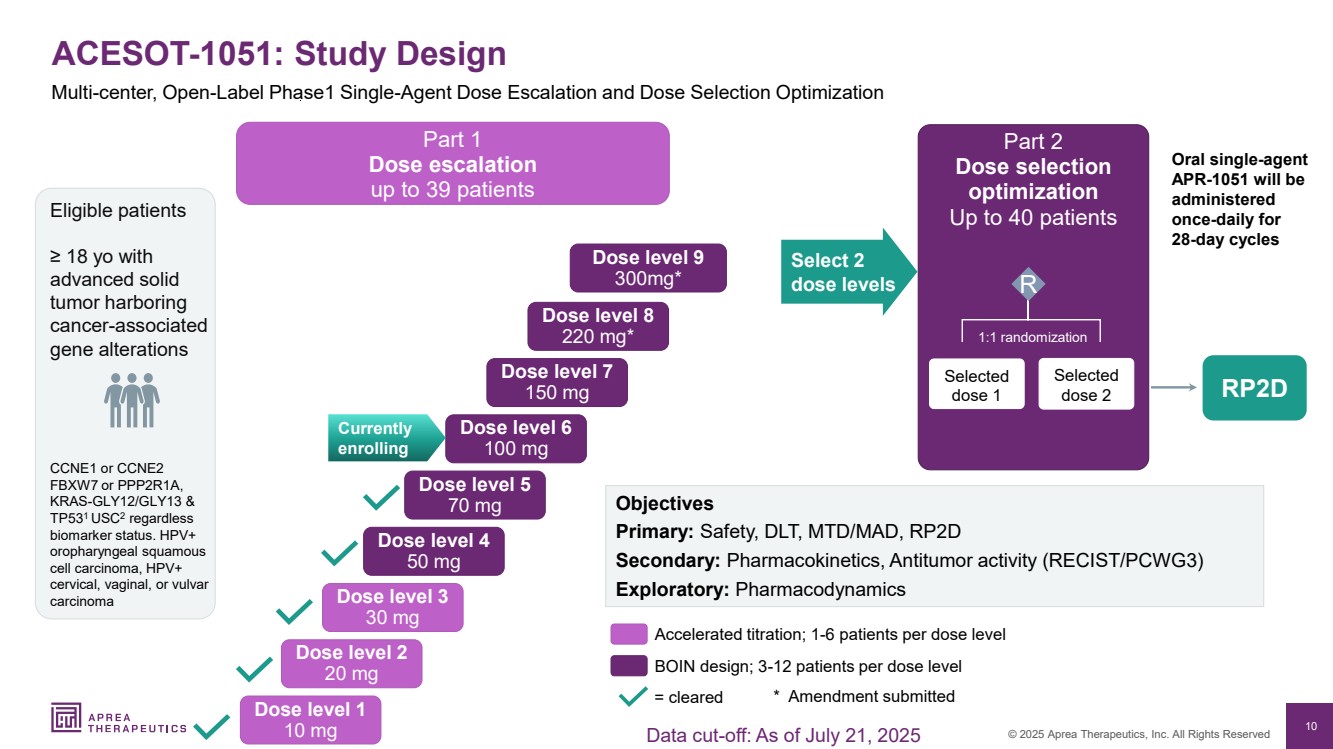
| 10 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Part 2 Dose selection optimization Up to 40 patients Eligible patients ≥ 18 yo with advanced solid tumor harboring cancer-associated gene alterations CCNE1 or CCNE2 FBXW7 or PPP2R1A, KRAS-GLY12/GLY13 & TP531 USC2 regardless biomarker status. HPV+ oropharyngeal squamous cell carcinoma, HPV+ cervical, vaginal, or vulvar carcinoma ACESOT-1051: Study Design Part 1 Dose escalation up to 39 patients Select 2 dose levels RP2D Oral single-agent APR-1051 will be administered once-daily for 28-day cycles Selected dose 1 Selected dose 2 1:1 randomization Objectives Primary: Safety, DLT, MTD/MAD, RP2D Secondary: Pharmacokinetics, Antitumor activity (RECIST/PCWG3) Exploratory: Pharmacodynamics Dose level 1 10 mg Dose level 2 20 mg Dose level 3 30 mg Dose level 4 50 mg Dose level 5 70 mg Dose level 6 100 mg Dose level 7 150 mg Dose level 8 220 mg* = cleared Accelerated titration; 1-6 patients per dose level BOIN design; 3-12 patients per dose level R Currently enrolling Multi-center, Open-Label Phase1 Single-Agent Dose Escalation and Dose Selection Optimization * Amendment submitted Dose level 9 300mg* Data cut-off: As of July 21, 2025 |
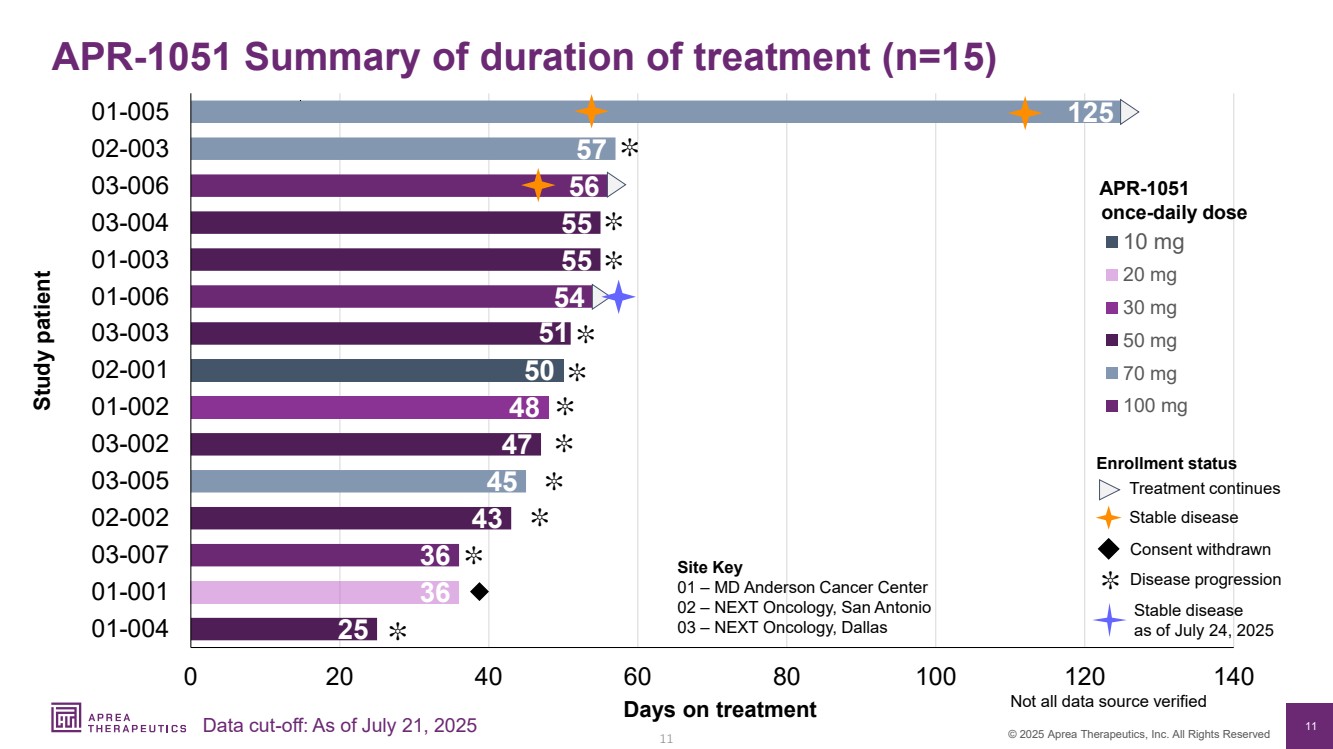
| 11 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 36 54 56 45 57 125 25 43 47 51 55 55 48 36 50 0 20 40 60 80 100 120 140 01-004 01-001 03-007 02-002 03-005 03-002 01-002 02-001 03-003 01-006 01-003 03-004 03-006 02-003 01-005 10 mg 20 mg 30 mg 50 mg 70 mg 100 mg Site Key 01 – MD Anderson Cancer Center 02 – NEXT Oncology, San Antonio 03 – NEXT Oncology, Dallas Days on treatment Enrollment status 11 Consent withdrawn Stable disease Study patient APR-1051 once-daily dose APR-1051 Summary of duration of treatment (n=15) Data cut-off: As of July 21, 2025 Not all data source verified ✼ Disease progression ✼ ✼ ✼ ✼ ✼ ✼ ✼ Treatment continues ✼ ✼ ✼ ✼ Stable disease as of July 24, 2025 |
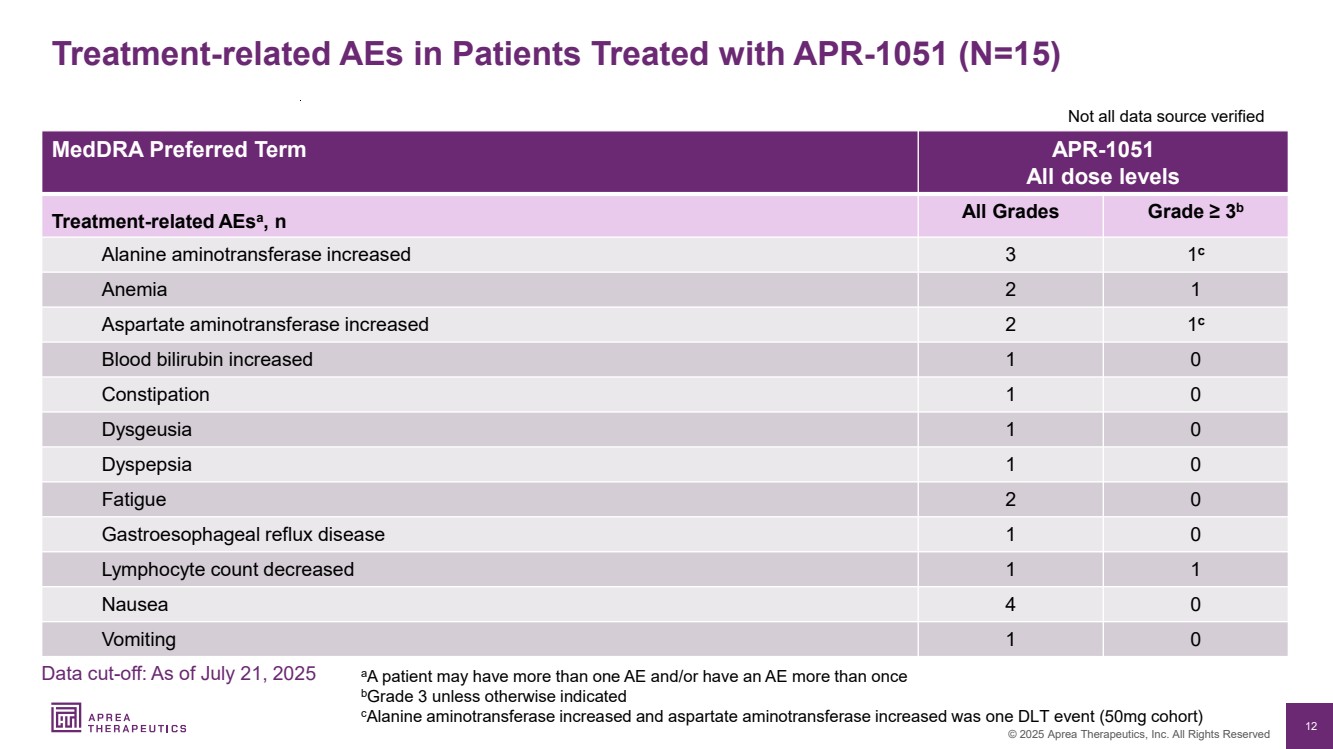
| 12 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Treatment-related AEs in Patients Treated with APR-1051 (N=15) MedDRA Preferred Term APR-1051 All dose levels Treatment-related AEsa , n All Grades Grade ≥ 3b Alanine aminotransferase increased 3 1 c Anemia 2 1 Aspartate aminotransferase increased 2 1 c Blood bilirubin increased 1 0 Constipation 1 0 Dysgeusia 1 0 Dyspepsia 1 0 Fatigue 2 0 Gastroesophageal reflux disease 1 0 Lymphocyte count decreased 1 1 Nausea 4 0 Vomiting 1 0 aA patient may have more than one AE and/or have an AE more than once bGrade 3 unless otherwise indicated cAlanine aminotransferase increased and aspartate aminotransferase increased was one DLT event (50mg cohort) Not all data source verified Data cut-off: As of July 21, 2025 |
| 13 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 13 APR-1051: Potentially Differentiated WEE1 Inhibitor Pre-Clinical |
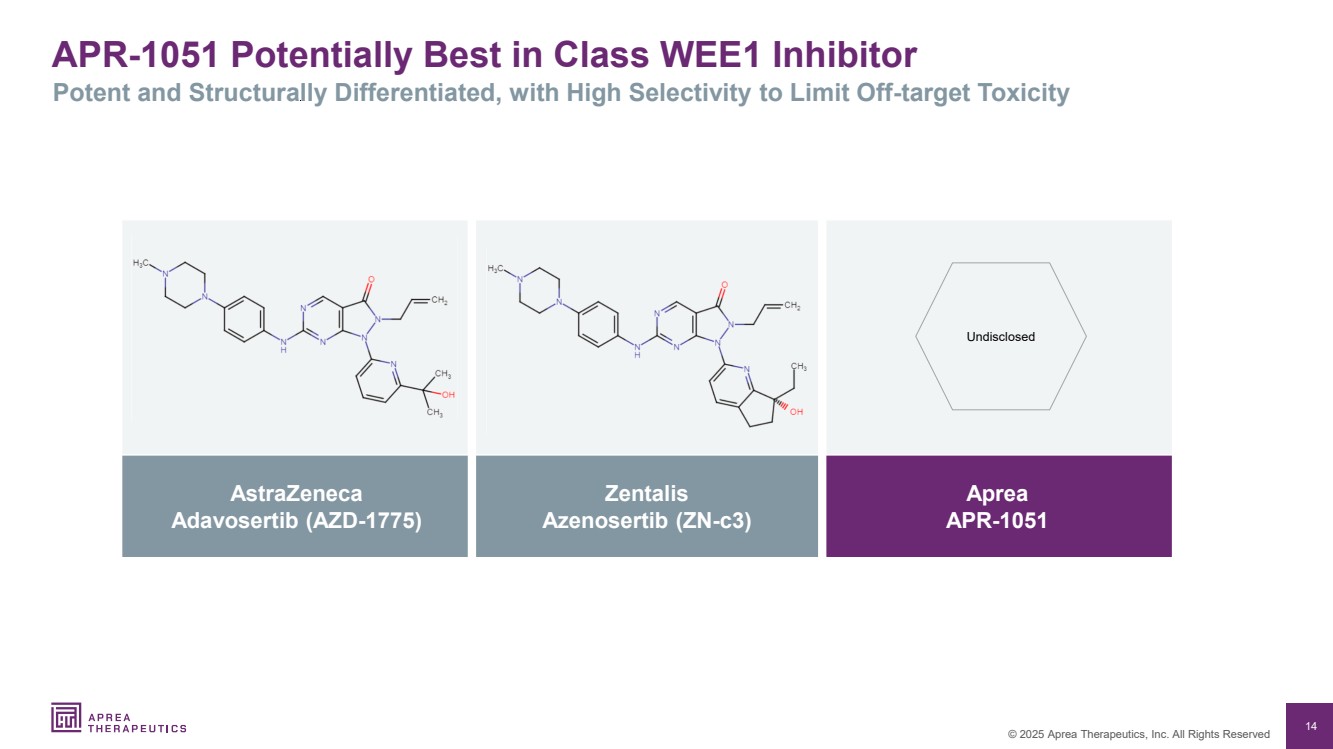
| 14 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051 Potentially Best in Class WEE1 Inhibitor Potent and Structurally Differentiated, with High Selectivity to Limit Off-target Toxicity AstraZeneca Adavosertib (AZD-1775) Zentalis Azenosertib (ZN-c3) Aprea APR-1051 Undisclosed |
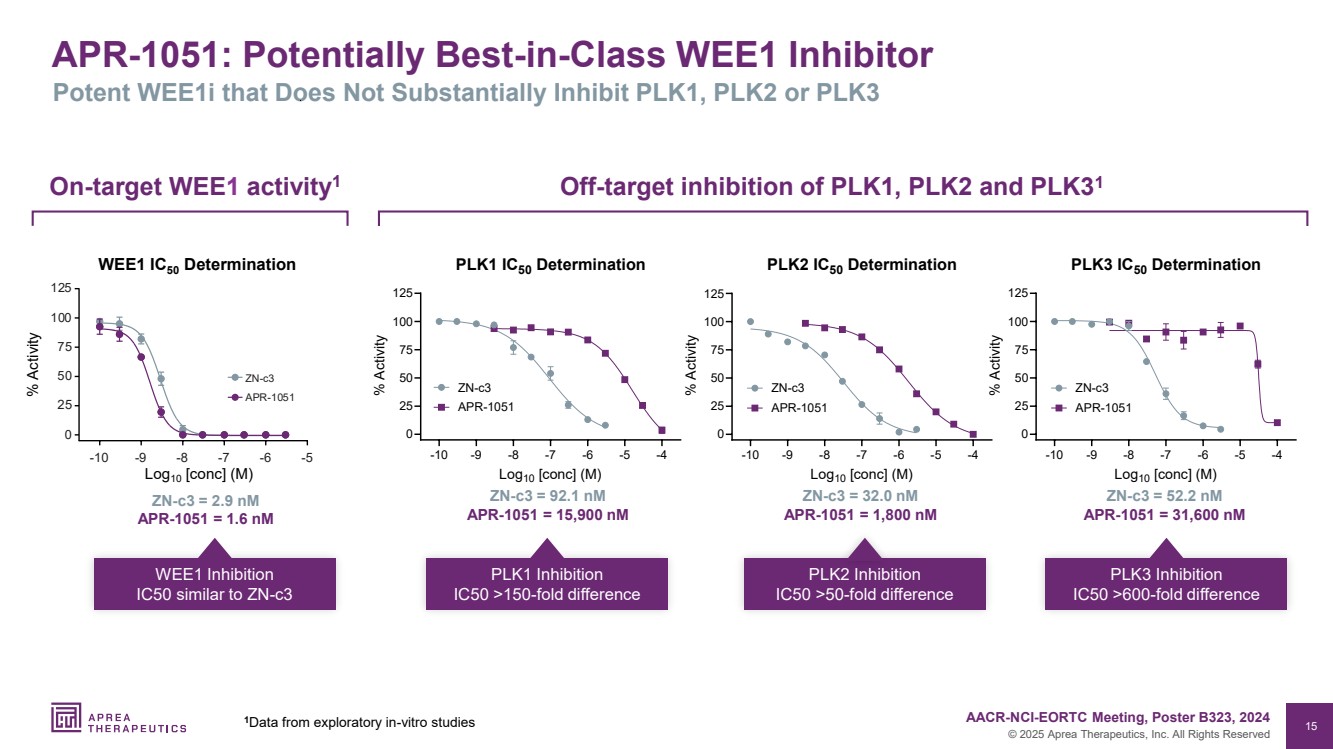
| 15 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051: Potentially Best-in-Class WEE1 Inhibitor Potent WEE1i that Does Not Substantially Inhibit PLK1, PLK2 or PLK3 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK1 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK2 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK3 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 ZN-c3 = 92.1 nM APR-1051 = 15,900 nM PLK1 Inhibition IC50 >150-fold difference ZN-c3 = 32.0 nM APR-1051 = 1,800 nM PLK2 Inhibition IC50 >50-fold difference ZN-c3 = 52.2 nM APR-1051 = 31,600 nM PLK3 Inhibition IC50 >600-fold difference Off-target inhibition of PLK1, PLK2 and PLK3 On 1 -target WEE1 activity1 ZN-c3 = 2.9 nM APR-1051 = 1.6 nM WEE1 Inhibition IC50 similar to ZN-c3 1 1 1 8 1 1 c3 WEE1 IC50 Determination % Activity Log10 [conc] (M) 1 AACR-NCI-EORTC Meeting, Poster B323, 2024 Data from exploratory in-vitro studies |
| 16 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Studies Show PLK1 Suppression is Associated with Sepsis-Induced Loss of Intestinal Barrier Function 1 PLK1 protects against sepsis-induced intestinal barrier dysfunction, Cao et al, Scientific Reports (2018). 2 PLK1 protects intestinal barrier function in sepsis: A translational research, Cao et al, Cytokine (2023). 3 PLK1 protects intestinal barrier function in sepsis: A translational research, Cao et al, Molecular Medicine (2022). 4 LncRNA DANCR improves the dysfunction of the intestinal barrier and alleviates epithelial injury by targeting the miR‐1306‐5p/PLK1 axis in sepsis, Wang et al., Cell Biology International (2021). |
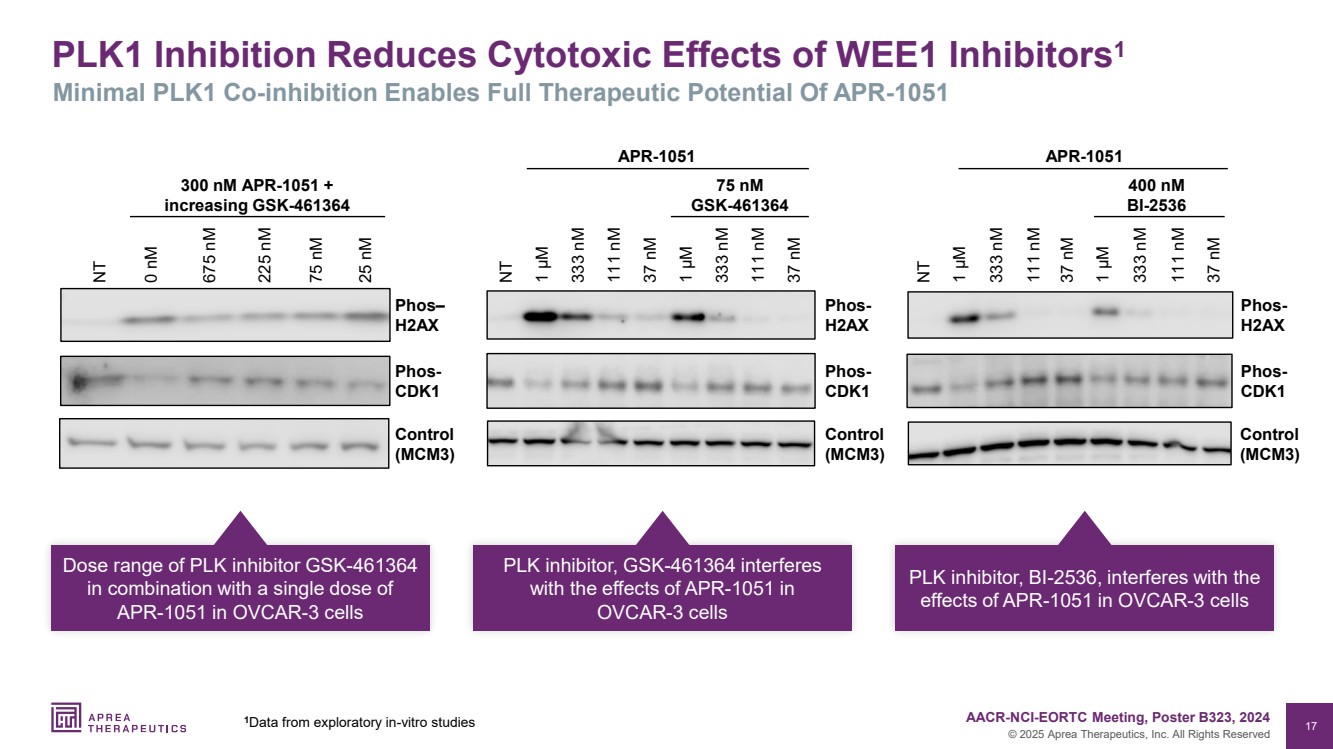
| 17 © 2025 Aprea Therapeutics, Inc. All Rights Reserved PLK1 Inhibition Reduces Cytotoxic Effects of WEE1 Inhibitors1 Minimal PLK1 Co-inhibition Enables Full Therapeutic Potential Of APR-1051 37 nM 111 nM 333 nM 1 µM 37 nM 111 nM 333 nM 1 µM Phos-H2AX Control (MCM3) NT Phos-CDK1 APR-1051 75 nM GSK-461364 0 nM NT 675 nM 25 nM 225 nM 75 nM Phos– H2AX Control (MCM3) Phos-CDK1 300 nM APR-1051 + increasing GSK-461364 Control (MCM3) 37 nM 111 nM 333 nM 1 µM 37 nM 111 nM 333 nM NT 1 µM Phos-H2AX 400 nM BI-2536 APR-1051 Phos-CDK1 Dose range of PLK inhibitor GSK-461364 in combination with a single dose of APR-1051 in OVCAR-3 cells PLK inhibitor, GSK-461364 interferes with the effects of APR-1051 in OVCAR-3 cells PLK inhibitor, BI-2536, interferes with the effects of APR-1051 in OVCAR-3 cells 1 AACR-NCI-EORTC Meeting, Poster B323, 2024 Data from exploratory in-vitro studies |
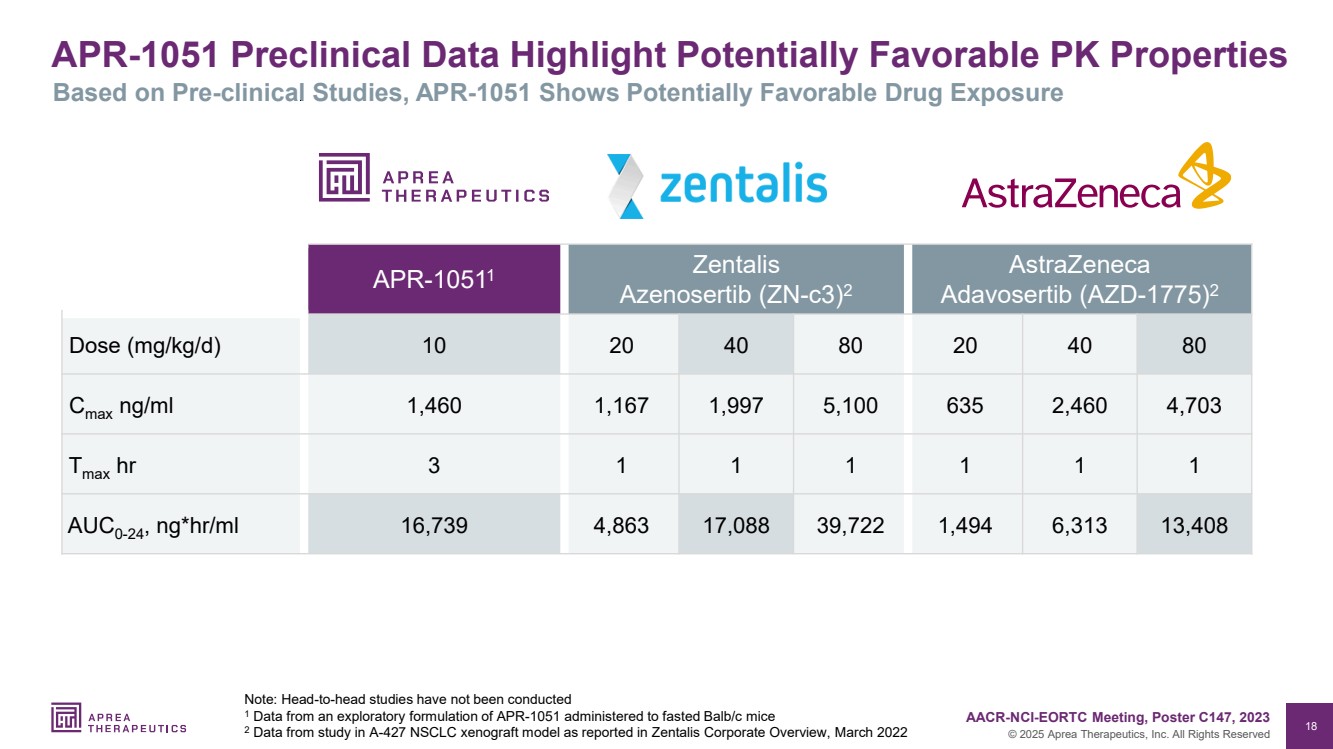
| 18 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051 Preclinical Data Highlight Potentially Favorable PK Properties Note: Head-to-head studies have not been conducted 1 Data from an exploratory formulation of APR-1051 administered to fasted Balb/c mice 2 Data from study in A-427 NSCLC xenograft model as reported in Zentalis Corporate Overview, March 2022 Based on Pre-clinical Studies, APR-1051 Shows Potentially Favorable Drug Exposure APR-10511 Zentalis Azenosertib (ZN-c3)2 AstraZeneca Adavosertib (AZD-1775)2 Dose (mg/kg/d) 10 20 40 80 20 40 80 Cmax ng/ml 1,460 1,167 1,997 5,100 635 2,460 4,703 Tmax hr 3 1 1 1 1 1 1 AUC0-24, ng*hr/ml 16,739 4,863 17,088 39,722 1,494 6,313 13,408 AACR-NCI-EORTC Meeting, Poster C147, 2023 |
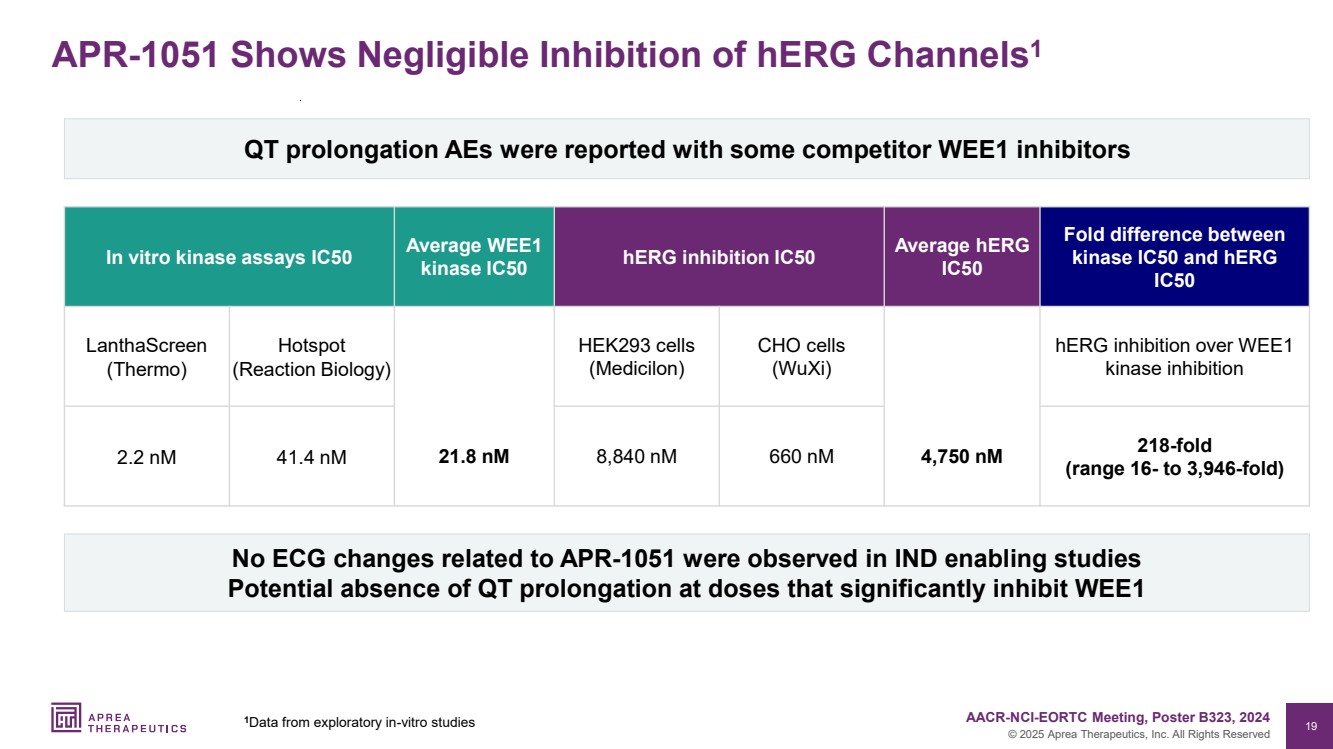
| 19 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051 Shows Negligible Inhibition of hERG Channels1 In vitro kinase assays IC50 Average WEE1 kinase IC50 hERG inhibition IC50 Average hERG IC50 Fold difference between kinase IC50 and hERG IC50 LanthaScreen (Thermo) Hotspot (Reaction Biology) HEK293 cells (Medicilon) CHO cells (WuXi) hERG inhibition over WEE1 kinase inhibition 2.2 nM 41.4 nM 21.8 nM 8,840 nM 660 nM 4,750 nM 218-fold (range 16- to 3,946-fold) QT prolongation AEs were reported with some competitor WEE1 inhibitors No ECG changes related to APR-1051 were observed in IND enabling studies Potential absence of QT prolongation at doses that significantly inhibit WEE1 1 AACR-NCI-EORTC Meeting, Poster B323, 2024 Data from exploratory in-vitro studies |
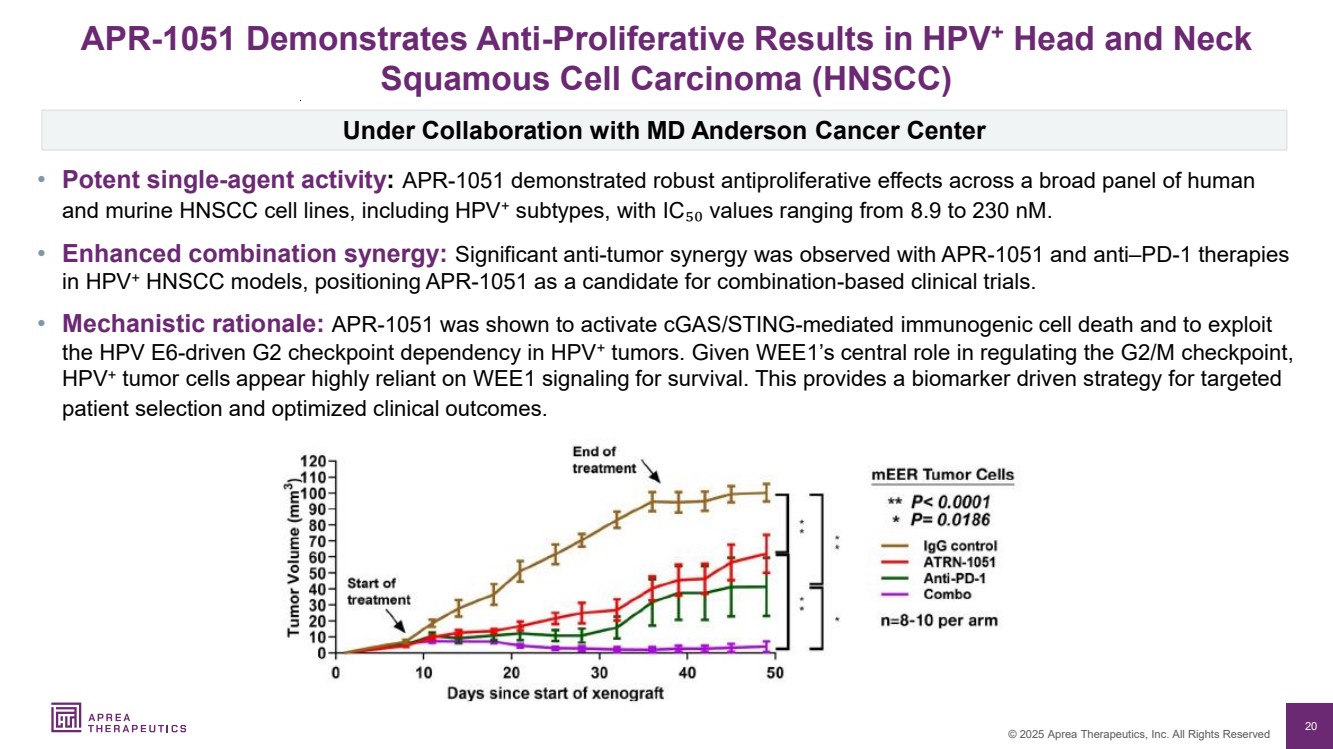
| 20 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051 Demonstrates Anti-Proliferative Results in HPV+ Head and Neck Squamous Cell Carcinoma (HNSCC) Under Collaboration with MD Anderson Cancer Center • Potent single-agent activity: APR-1051 demonstrated robust antiproliferative effects across a broad panel of human and murine HNSCC cell lines, including HPV+ subtypes, with IC₅₀ values ranging from 8.9 to 230 nM. • Enhanced combination synergy: Significant anti-tumor synergy was observed with APR-1051 and anti–PD-1 therapies in HPV+ HNSCC models, positioning APR-1051 as a candidate for combination-based clinical trials. • Mechanistic rationale: APR-1051 was shown to activate cGAS/STING-mediated immunogenic cell death and to exploit the HPV E6-driven G2 checkpoint dependency in HPV+ tumors. Given WEE1’s central role in regulating the G /M checkpoint, HPV+ tumor cells appear highly reliant on WEE1 signaling for survival. This provides a biomarker driven strategy for targeted patient selection and optimized clinical outcomes. |
| 21 © 2025 Aprea Therapeutics, Inc. All Rights Reserved APR-1051: Summary Potential best in class WEE1 inhibitor • High potency for WEE1 inhibition in vitro • Low off-target inhibition of the LK family of kinases • Suppresses growth of CCNE1-amplified HGSOC xenografted tumors and relatively well-tolerated in mice • Significant anti-tumor synergy with APR-1051 plus anti–PD-1 therapies in HPV+ HNSCC mouse models ACESOT-1051: First-In-Human Study (NCT06260514) • Early signs of clinical activity: Three patients achieved stable disease • Accelerated titration dose escalation completed, sixth cohort now enrolling • Biomarker-driven study in patients with advanced/metastatic solid tumors • Targeted gene alterations include CCNE1, CCNE2, FBXW7, PPP2R1A, HPV+, or KRAS-G12/13 with TP53 • Based on encouraging tolerability profile to date → accelerating dose titration schedule • Open label data update H2 2025, complete dose escalation expected H1 2026 • MD Anderson Cancer Center lead study site, with up to 10 sites in U.S. |
| 22 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ATR Inhibitor: ATRN- 119 |

| 23 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 23 ATR Inhibitor: ATRN-119 ABOYA-119: Clinical Proof-Of-Concept |

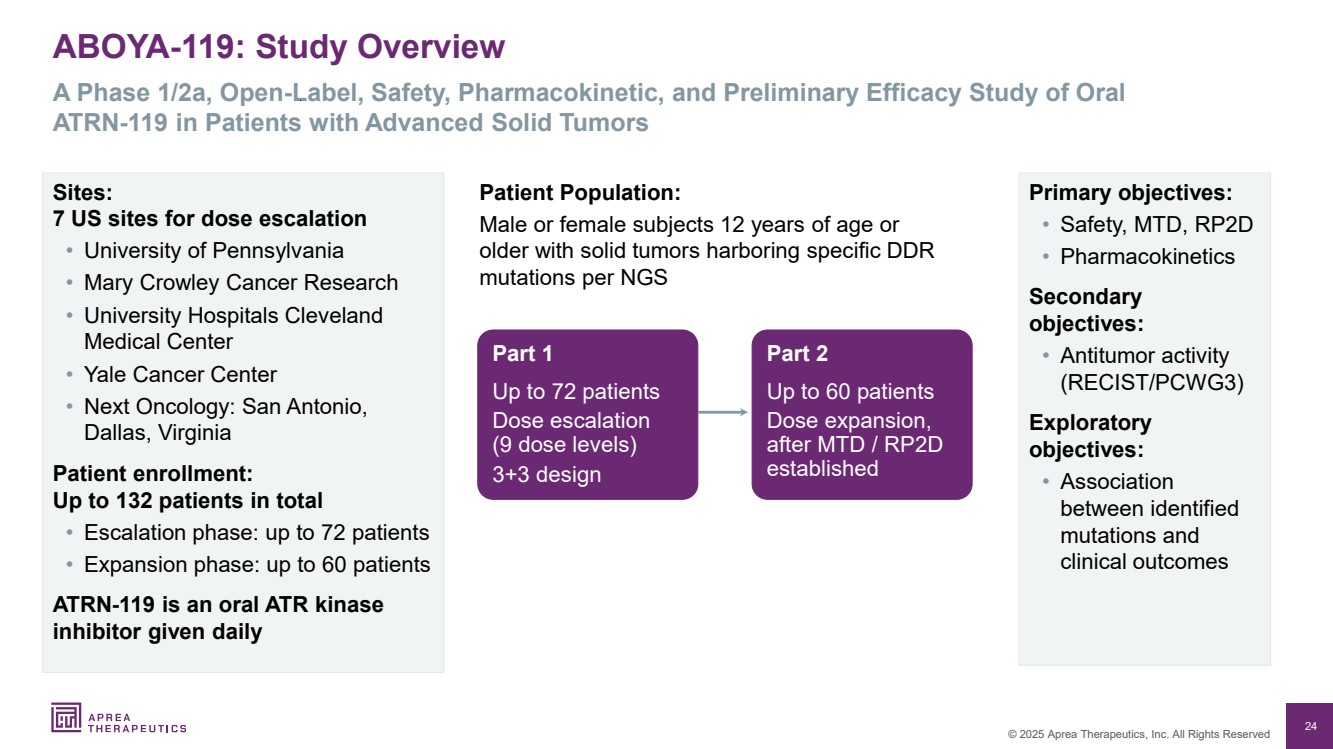
| 24 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ABOYA-119: Study Overview A Phase 1/2a, Open-Label, Safety, Pharmacokinetic, and Preliminary Efficacy Study of Oral ATRN-119 in Patients with Advanced Solid Tumors Part 1 Up to patients Dose escalation ( dose levels) 3+3 design Primary objectives: • Safety, MTD, RP2D • Pharmacokinetics Secondary objectives: • Antitumor activity (RECIST/PCWG3) Exploratory objectives: • Association between identified mutations and clinical outcomes Patient Population: Male or female subjects 12 years of age or older with solid tumors harboring specific DDR mutations per NGS Part 2 Up to 60 patients Dose expansion, after MTD / RP2D established Sites: 7 US sites for dose escalation • University of Pennsylvania • Mary Crowley Cancer Research • University Hospitals Cleveland Medical Center • Yale Cancer Center • Next Oncology: San Antonio, Dallas, Virginia Patient enrollment: Up to 132 patients in total • Escalation phase: up to 72 patients • Expansion phase: up to 60 patients ATRN-119 is an oral ATR kinase inhibitor given daily |
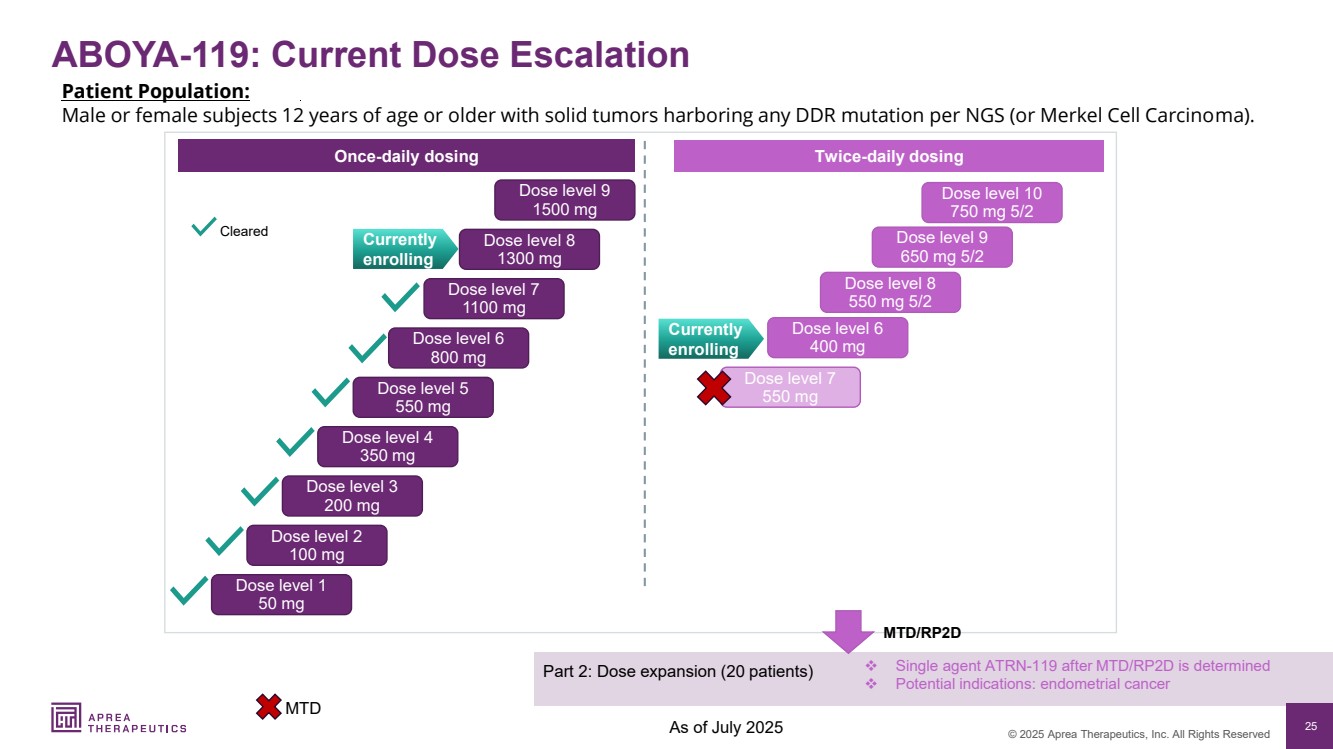
| 25 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ABOYA-119: Current Dose Escalation Patient Population: Male or female subjects 12 years of age or older with solid tumors harboring any DDR mutation per NGS (or Merkel Cell Carcinoma). ❖ Single agent ATRN-119 after MTD/RP2D is determined ❖ Potential indications: endometrial cancer Dose level 1 50 mg Dose level 2 100 mg Dose level 3 200 mg Dose level 4 350 mg Dose level 5 550 mg Dose level 6 800 mg Dose level 7 1100 mg Dose level 8 1300 mg Dose level 9 1500 mg Once-daily dosing Twice-daily dosing Currently enrolling Cleared Currently enrolling Dose level 6 400 mg Part 2: Dose expansion (20 patients) MTD/RP2D Dose level 8 550 mg 5/2 Dose level 9 650 mg 5/2 Dose level 7 550 mg Dose level 10 750 mg 5/2 As of July 2025 MTD |
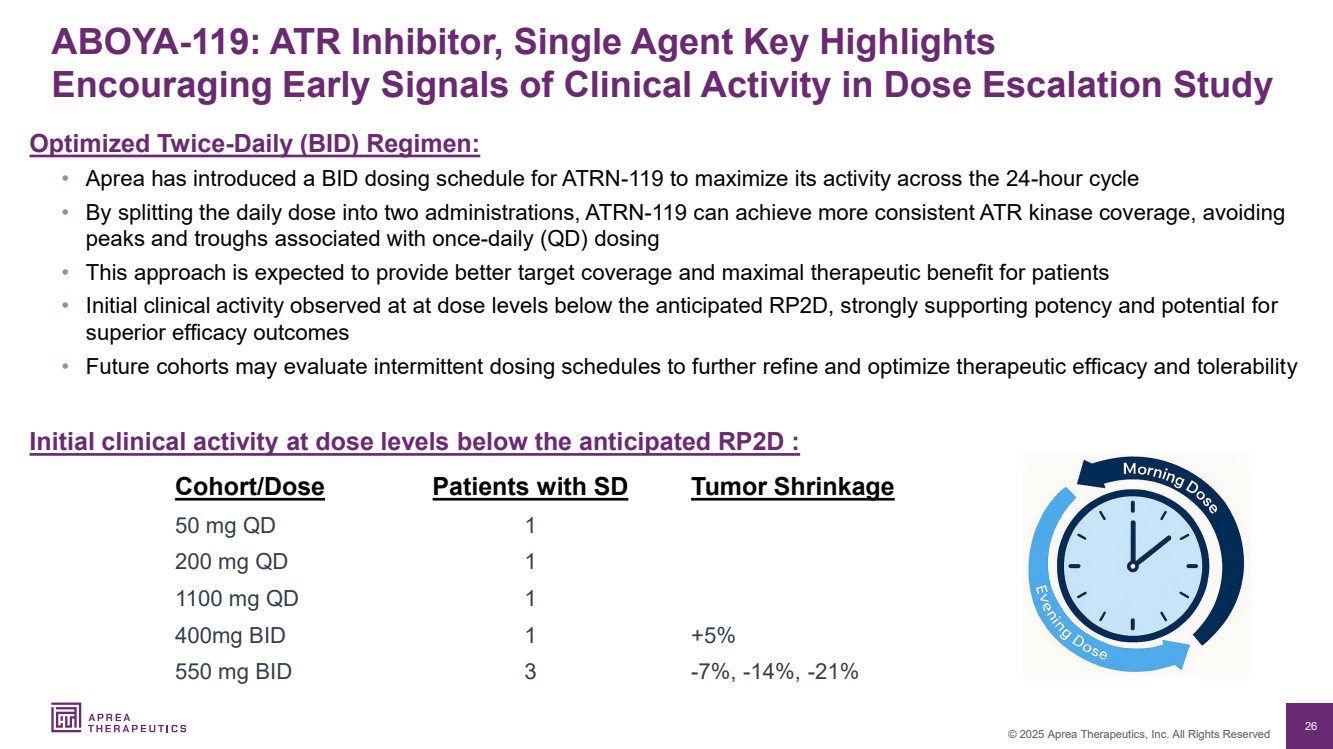
| 26 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ABOYA-119: ATR Inhibitor, Single Agent Key Highlights Encouraging Early Signals of Clinical Activity in Dose Escalation Study Optimized Twice-Daily (BID) Regimen: • Aprea has introduced a BID dosing schedule for ATRN-119 to maximize its activity across the 24-hour cycle • By splitting the daily dose into two administrations, ATRN-119 can achieve more consistent ATR kinase coverage, avoiding peaks and troughs associated with once-daily (QD) dosing • This approach is expected to provide better target coverage and maximal therapeutic benefit for patients • Initial clinical activity observed at at dose levels below the anticipated RP2D, strongly supporting potency and potential for superior efficacy outcomes • Future cohorts may evaluate intermittent dosing schedules to further refine and optimize therapeutic efficacy and tolerability Initial clinical activity at dose levels below the anticipated RP2D : Cohort/Dose Patients with SD Tumor Shrinkage 50 mg QD 1 200 mg QD 1 1100 mg QD 1 400mg BID 1 +5% 550 mg BID 3 -7%, -14%, -21% |
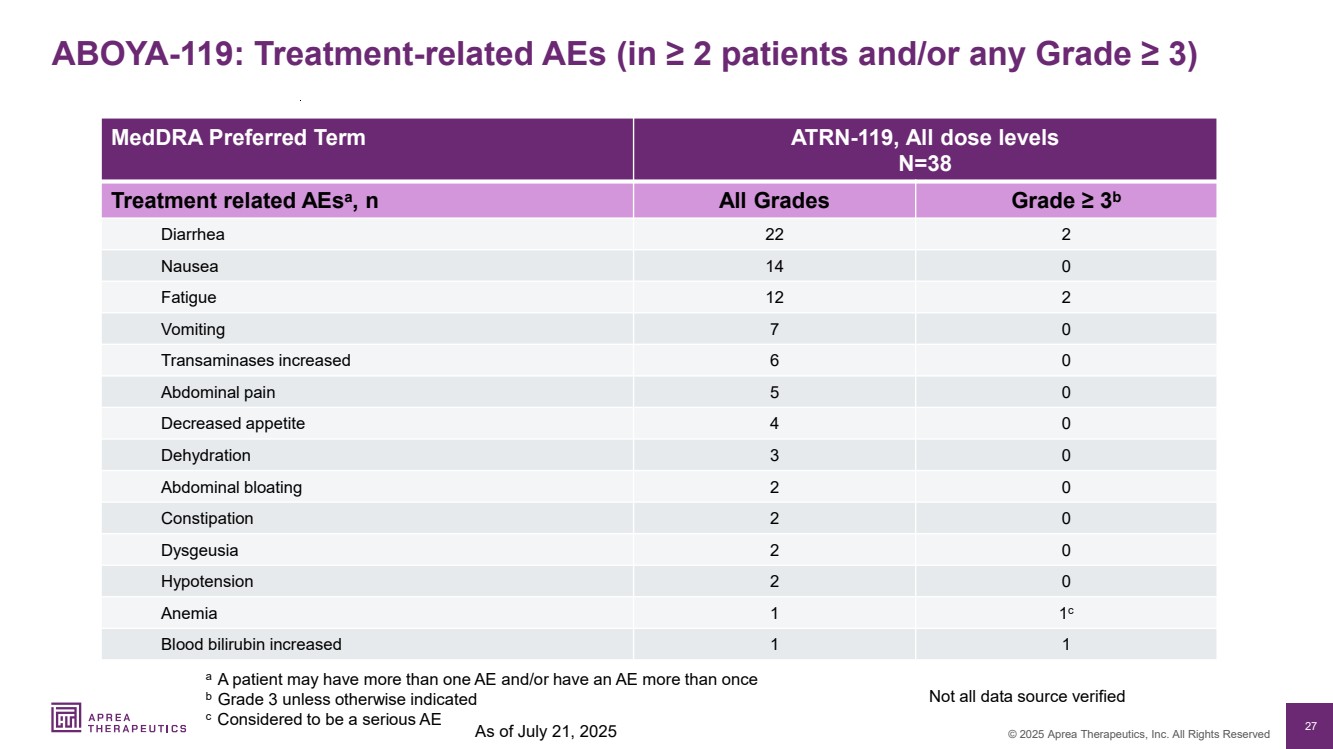
| 27 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ABOYA-119: Treatment-related AEs (in ≥ 2 patients and/or any Grade ≥ 3) MedDRA Preferred Term ATRN-119, All dose levels N=38 Treatment related AEsa , n All Grades Grade ≥ 3b Diarrhea 22 2 Nausea 14 0 Fatigue 12 2 Vomiting 7 0 Transaminases increased 6 0 Abdominal pain 5 0 Decreased appetite 4 0 Dehydration 3 0 Abdominal bloating 2 0 Constipation 2 0 Dysgeusia 2 0 Hypotension 2 0 Anemia 1 1 c Blood bilirubin increased 1 1 a A patient may have more than one AE and/or have an AE more than once b Grade 3 unless otherwise indicated c Considered to be a serious AE Not all data source verified As of July 21, 2025 |
| 28 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 28 ATRN-119: Potentially Differentiated ATR Inhibitor |

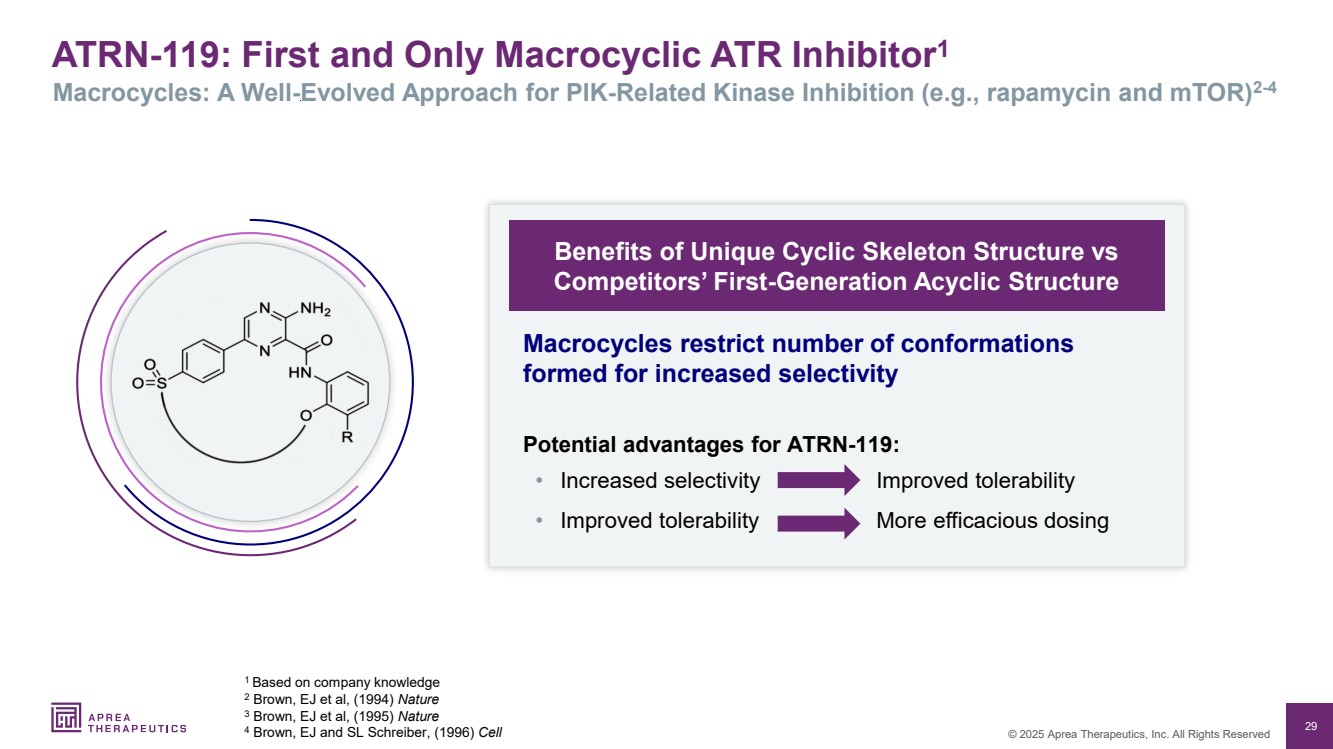
| 29 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ATRN-119: First and Only Macrocyclic ATR Inhibitor1 Macrocycles: A Well-Evolved Approach for PIK-Related Kinase Inhibition (e.g., rapamycin and mTOR)2-4 1 Based on company knowledge 2 Brown, EJ et al, (1994) Nature 3 Brown, EJ et al, (1995) Nature 4 Brown, EJ and SL Schreiber, (1996) Cell Benefits of Unique Cyclic Skeleton Structure vs Competitors’ First-Generation Acyclic Structure • Increased selectivity • Improved tolerability Improved tolerability More efficacious dosing Macrocycles restrict number of conformations formed for increased selectivity Potential advantages for ATRN-119: |
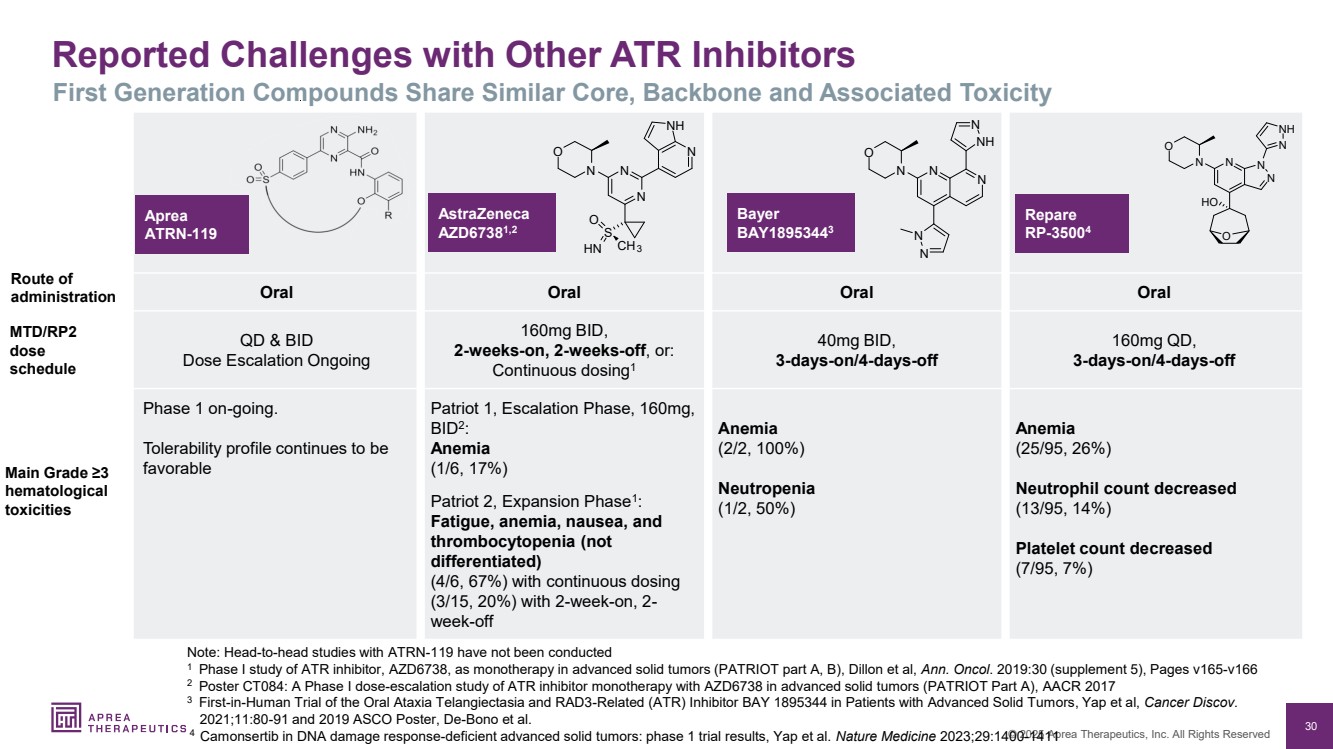
| 30 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Reported Challenges with Other ATR Inhibitors First Generation Compounds Share Similar Core, Backbone and Associated Toxicity Note: Head-to-head studies with ATRN-119 have not been conducted 1 Phase I study of ATR inhibitor, AZD6738, as monotherapy in advanced solid tumors (PATRIOT part A, B), Dillon et al, Ann. Oncol. 2019:30 (supplement 5), Pages v165-v166 2 Poster CT084: A Phase I dose-escalation study of ATR inhibitor monotherapy with AZD6738 in advanced solid tumors (PATRIOT Part A), AACR 2017 3 First-in-Human Trial of the Oral Ataxia Telangiectasia and RAD3-Related (ATR) Inhibitor BAY 1895344 in Patients with Advanced Solid Tumors, Yap et al, Cancer Discov. 2021;11:80-91 and 2019 ASCO Poster, De-Bono et al. 4 Camonsertib in DNA damage response-deficient advanced solid tumors: phase 1 trial results, Yap et al. Nature Medicine 2023;29:1400-1411 Oral Oral Oral Oral QD & BID Dose Escalation Ongoing 160mg BID, 2-weeks-on, 2-weeks-off, or: Continuous dosing1 40mg BID, 3-days-on/4-days-off 160mg QD, 3-days-on/4-days-off Phase 1 on-going. Tolerability profile continues to be favorable Patriot 1, Escalation Phase, 160mg, BID2 : Anemia (1/6, 17%) Patriot 2, Expansion Phase1 : Fatigue, anemia, nausea, and thrombocytopenia (not differentiated) (4/6, 67%) with continuous dosing (3/15, 20%) with 2-week-on, 2- week-off Anemia (2/2, 100%) Neutropenia (1/2, 50%) Anemia (25/95, 26%) Neutrophil count decreased (13/95, 14%) Platelet count decreased (7/95, 7%) AstraZeneca AZD67381,2 Bayer BAY18953443 Repare RP-35004 N N NH N N N N O N N N O S O HN CH3 N NH N N O N N HO O N NH Route of administration MTD/RP2 dose schedule Main Grade ≥3 hematological toxicities Aprea ATRN-119 |
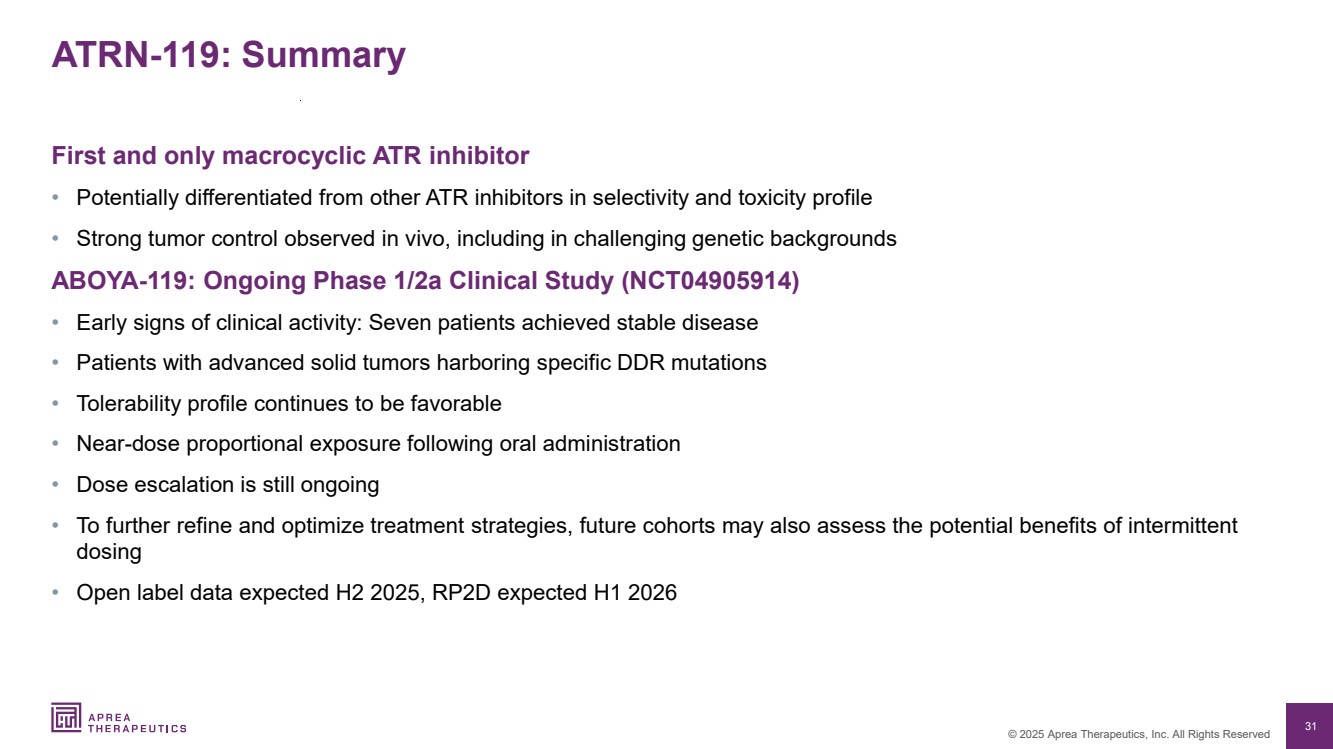
| 31 © 2025 Aprea Therapeutics, Inc. All Rights Reserved ATRN-119: Summary First and only macrocyclic ATR inhibitor • Potentially differentiated from other ATR inhibitors in selectivity and toxicity profile • Strong tumor control observed in vivo, including in challenging genetic backgrounds ABOYA-119: Ongoing Phase 1/2a Clinical Study (NCT04905914) • Early signs of clinical activity: Seven patients achieved stable disease • Patients with advanced solid tumors harboring specific DDR mutations • Tolerability profile continues to be favorable • Near-dose proportional exposure following oral administration • Dose escalation is still ongoing • To further refine and optimize treatment strategies, future cohorts may also assess the potential benefits of intermittent dosing • Open label data expected H2 2025, RP2D expected H1 2026 |
| 32 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Aprea Therapeutics (NASDAQ: APRE) |
| 33 © 2025 Aprea Therapeutics, Inc. All Rights Reserved 33 Intellectual Property Portfolio Financial Summary & Capitalization Investment Highlights |

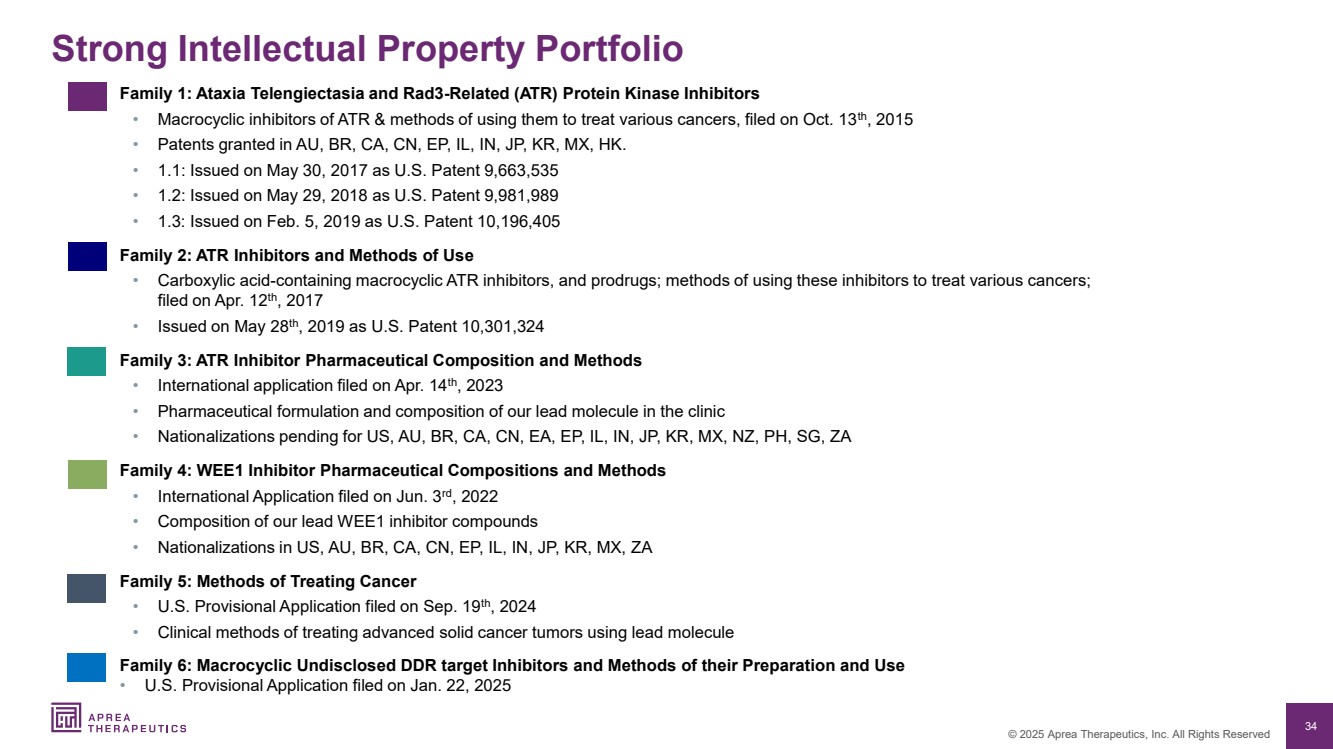
| 34 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Strong Intellectual Property Portfolio Family 1: Ataxia Telengiectasia and Rad3-Related (ATR) Protein Kinase Inhibitors • Macrocyclic inhibitors of ATR & methods of using them to treat various cancers, filed on Oct. 13th, 2015 • Patents granted in AU, BR, CA, CN, EP, IL, IN, JP, KR, MX, HK. • 1.1: Issued on May 30, 2017 as U.S. Patent 9,663,535 • 1.2: Issued on May 29, 2018 as U.S. Patent 9,981,989 • 1.3: Issued on Feb. 5, 2019 as U.S. Patent 10,196,405 Family 2: ATR Inhibitors and Methods of Use • Carboxylic acid-containing macrocyclic ATR inhibitors, and prodrugs; methods of using these inhibitors to treat various cancers; filed on Apr. 12th, 2017 • Issued on May 28th, 2019 as U.S. Patent 10,301,324 Family 3: ATR Inhibitor Pharmaceutical Composition and Methods • International application filed on Apr. 14th, 2023 • Pharmaceutical formulation and composition of our lead molecule in the clinic • Nationalizations pending for US, AU, BR, CA, CN, EA, EP, IL, IN, JP, KR, MX, NZ, PH, SG, ZA Family 4: WEE1 Inhibitor Pharmaceutical Compositions and Methods • International Application filed on Jun. 3rd, 2022 • Composition of our lead WEE1 inhibitor compounds • Nationalizations in US, AU, BR, CA, CN, EP, IL, IN, JP, KR, MX, ZA Family 5: Methods of Treating Cancer • U.S. Provisional Application filed on Sep. 19th, 2024 • Clinical methods of treating advanced solid cancer tumors using lead molecule Family 6: Macrocyclic Undisclosed DDR target Inhibitors and Methods of their Preparation and Use • U.S. Provisional Application filed on Jan. 22, 2025 |
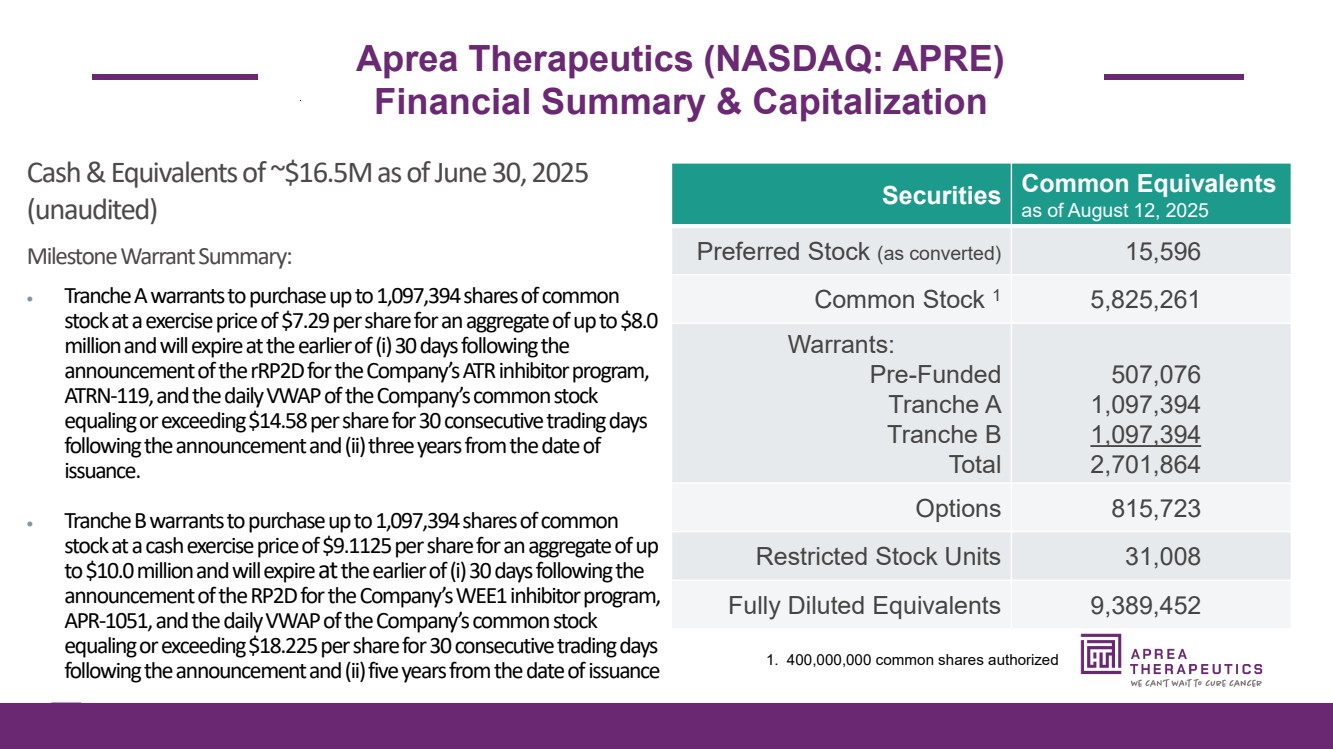
| 35 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Aprea Therapeutics (NASDAQ: APRE) Financial Summary & Capitalization Securities Common Equivalents as of August 12, 2025 Preferred Stock (as converted) 15,596 Common Stock 1 5,825,261 Warrants: Pre-Funded Tranche A Tranche B Total 507,076 1,097,394 1,097,394 2,701,864 Options 815,723 Restricted Stock Units 31,008 Fully Diluted Equivalents 9,389,452 Cash & Equivalents of ~$16.5M as of June 30, 2025 (unaudited) Milestone Warrant Summary: • Tranche A warrants to purchase up to 1,097,394 shares of common stock at a exercise price of$7.29per share for an aggregate of up to$8.0 millionand will expire at the earlier of (i) 30 days following the announcement of the rRP2D for the Company’s ATR inhibitor program, ATRN-119, andthe daily VWAP of the Company’s common stock equaling or exceeding$14.58per share for 30 consecutive trading days following the announcement and (ii) three years from the date of issuance. • Tranche B warrants to purchase up to 1,097,394 shares of common stock at a cash exercise price of$9.1125per share for an aggregate of up to$10.0 millionand will expire atthe earlier of (i) 30 days following the announcement of the RP2D for the Company’s WEE1 inhibitor program, APR-1051, andthe daily VWAP of the Company’s common stock equaling or exceeding$18.225per share for 30 consecutive trading days following the announcement and (ii) five years from the date of issuance 1. 400,000,000 common shares authorized |
| 36 © 2025 Aprea Therapeutics, Inc. All Rights Reserved Financed into Q2 2026 • Achieve short term inflection points and catalysts • Evaluate optimal strategic partnerships Near term catalysts • APR-1051: H2 2025 Safety/efficacy data ; H1 2026 Complete dose escalation • ATRN-119: H2 2025 Safety/efficacy data ; H1 2026 RP2D Diversified portfolio with best in class, de-risked clinical and preclinical programs • Highly potent and selective WEE1 (APR-1051) and ATR (ATRN-119) inhibitors • Opportunities in ovarian, colorectal, prostate, and endometrial cancers • Single agent and combination potential therapies Technology developed by pioneers in synthetic lethality • Management with strong drug development and commercial expertise Investment Highlights |