
.3
Delivering the Power of T cells to Cancer Patients © Immatics. Not for further reproduction or distribution. Immatics Corporate Presentation October 20, 2025
Forward - Looking Statement This presentation (“Presentation”) is provided by Immatics N . V . (“Immatics” or the “Company”) for informational purposes only . The information contained herein does not purport to be all - inclusive and none of Immatics, any of its affiliates, any of its or their respective control persons, officers, directors, employees or representatives makes any representation or warranty, express or implied, as to the accuracy, completeness or reliability of the information contained in this Presentation . Forward - Looking Statements . Certain statements in this presentation may be considered forward - looking statements . Forward - looking statements generally relate to future events or the Company’s future financial or operating performance . For example, statements concerning timing of data read - outs for product candidates, the timing, outcome and design of clinical trials, the nature of clinical trials (including whether such clinical trials will be registration - enabling), the timing of IND or CTA filing for pre - clinical stage product candidates, the timing of BLA filings for clinical stage product candidates, estimated market opportunities of product candidates, manufacturing timetables, capacity and success rates, the Company’s focus on partnerships to advance its strategy, and other metrics are forward - looking statements . In some cases, you can identify forward - looking statements by terminology such as “may”, “should”, “expect”, “plan”, “target”, “intend”, “will”, “estimate”, “anticipate”, “believe”, “predict”, “potential” or “continue”, or the negatives of these terms or variations of them or similar terminology . Such forward - looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ materially from those expressed or implied by such forward looking statements . These forward - looking statements are based upon estimates and assumptions that, while considered reasonable by Immatics and its management, are inherently uncertain . New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties . Factors that may cause actual results to differ materially from current expectations include, but are not limited to, various factors beyond management's control including general economic conditions and other risks, uncertainties and factors set forth in the Company’s Annual Report on Form 20 - F and other filings with the Securities and Exchange Commission (SEC) . Nothing in this presentation should be regarded as a representation by any person that the forward - looking statements set forth herein will be achieved or that any of the contemplated results of such forward - looking statements will be achieved . You should not place undue reliance on forward - looking statements, which speak only as of the date they are made . The Company undertakes no duty to update these forward - looking statements . No Offer or Solicitation . This communication is for informational purposes only and does not constitute, or form a part of, an offer to sell or the solicitation of an offer to sell or an offer to buy or the solicitation of an offer to buy any securities, and there shall be no sale of securities, in any jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such jurisdiction . No offer of securities shall be made except by means of a prospectus meeting the requirements of Section 10 of the Securities Act of 1933 , as amended, or in an offering exempt from registration . Certain information contained in this Presentation relates to or is based on studies, publications, surveys and the Company’s own internal estimates and research . In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions . Finally, while the Company believes its internal research is reliable, such research has not been verified by any independent source . All the scientific and clinical data presented within this presentation are – by definition prior to completion of the clinical trial and a clinical study report – preliminary in nature and subject to further quality checks including customary source data verification . 2
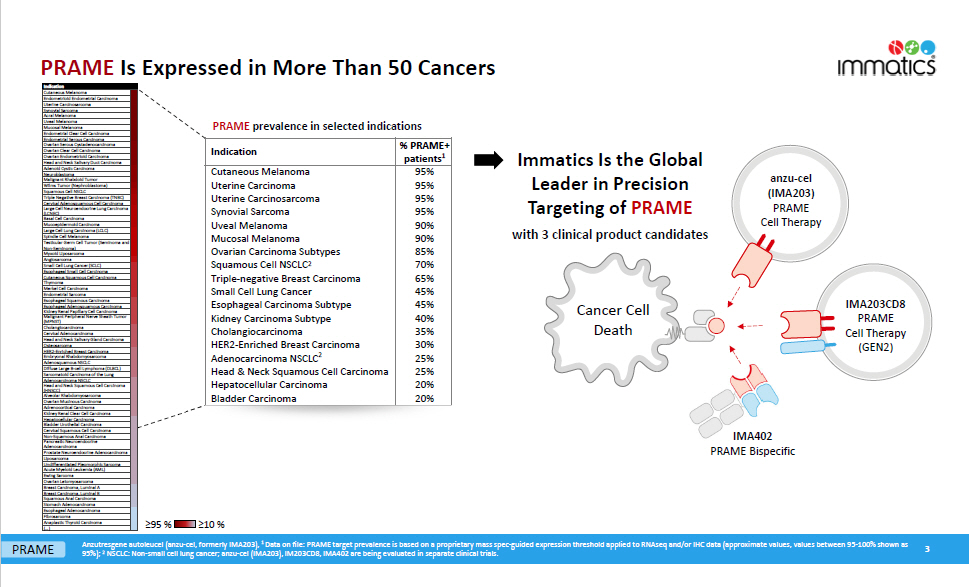
PRAME Is Expressed in More Than 50 Cancers ≥95 % ≥10 % Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Data on file: PRAME target prevalence is based on a proprietary mass spec - guided expression threshold applied to RNAseq and/or IHC data (approximate values, values between 95 - 100% shown as 95%); 2 NSCLC: Non - small cell lung cancer; anzu - cel (IMA203), IM203CD8, IMA402 are being evaluated in separate clinical trials. Cancer Cell Death IMA402 PRAME Bispecific anzu - cel (IMA 203 ) PRAME Cell Therapy IMA203CD8 PRAME Cell Therapy (GEN2) Immatics Is the Global Leader in Precision Targeting of PRAME with 3 clinical product candidates PRAME prevalence in selected indications % PRAME+ patients 1 Indication 95% Cutaneous Melanoma 95% Uterine Carcinoma 95% Uterine Carcinosarcoma 95% Synovial Sarcoma 90% Uveal Melanoma 90% Mucosal Melanoma 85% Ovarian Carcinoma Subtypes 70% Squamous Cell NSCLC 2 65% Triple - negative Breast Carcinoma 45% Small Cell Lung Cancer 45% Esophageal Carcinoma Subtype 40% Kidney Carcinoma Subtype 35% Cholangiocarcinoma 30% HER2 - Enriched Breast Carcinoma 25% Adenocarcinoma NSCLC 2 25% Head & Neck Squamous Cell Carcinoma 20% Hepatocellular Carcinoma 20% Bladder Carcinoma 3 PRAME Cutaneous Melanoma Endometrioid Endometrial Carcinoma Uterine Carcinosarcoma Synovial Sarcoma Acral Melanoma Uveal Melanoma Mucosal Melanoma Endometrial Clear Cell Carcinoma Endometrial Serous Carcinoma Ovarian Serous Cystadenocarcinoma Ovarian Clear Cell Carcinoma Ovarian Endometrioid Carcinoma Head and Neck Salivary Duct Carcinoma Adenoid Cystic Carcinoma Neuroblastoma Malignant Rhabdoid Tumor Wilms Tumor (Nephroblastoma) Squamous Cell NSCLC Triple Negative Breast Carcinoma (TNBC) Cervical Adenosquamous Cell Carcinoma Large Cell Neuroendocrine Lung Carcinoma (LCNEC) Basal Cell Carcinoma Mucoepidermoid Carcinoma Large Cell Lung Carcinoma (LCLC) Spindle Cell Melanoma Testicular Germ Cell Tumor (Seminoma and Non - Seminoma) Myxoid Liposarcoma Angiosarcoma Small Cell Lung Cancer (SCLC) Esophageal Small Cell Carcinoma Cutaneous Squamous Cell Carcinoma Thymoma Merkel Cell Carcinoma Endometrial Sarcoma Esophageal Squamous Carcinoma Esophageal Adenosquamous Carcinoma Kidney Renal Papillary Cell Carcinoma Malignant Peripheral Nerve Sheath Tumor (MPNST) Cholangiocarcinoma Cervical Adenocarcinoma Head and Neck Salivary Gland Carcinoma Osteosarcoma HER2 - Enriched Breast Carcinoma Embryonal Rhabdomyosarcoma Adenosquamous NSCLC Diffuse Large B - cell Lymphoma (DLBCL) Sarcomatoid Carcinoma of the Lung Adenocarcinoma NSCLC Head and Neck Squamous Cell Carcinoma (HNSCC) Alveolar Rhabdomyosarcoma Ovarian Mucinous Carcinoma Adrenocortical Carcinoma Kidney Renal Clear Cell Carcinoma Hepatocellular Carcinoma Bladder Urothelial Carcinoma Cervical Squamous Cell Carcinoma Non - Squamous Anal Carcinoma Pancreatic Neuroendocrine Adenocarcinoma Prostate Neuroendocrine Adenocarcinoma Liposarcoma Undifferentiated Pleomorphic Sarcoma Acute Myeloid Leukemia (AML) Ewing Sarcoma Ovarian Leiomyosarcoma Breast Carcinoma, Luminal A Breast Carcinoma, Luminal B Squamous Anal Carcinoma Stomach Adenocarcinoma Esophageal Adenocarcinoma Fibrosarcoma Anaplastic Thyroid Carcinoma (…) Indication
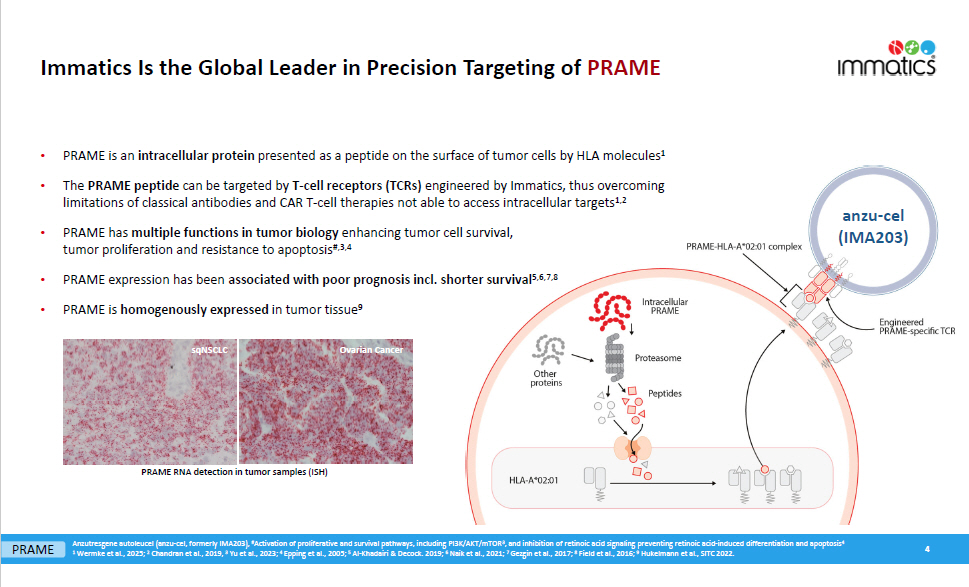
Immatics Is the Global Leader in Precision Targeting of PRAME • PRAME is an intracellular protein presented as a peptide on the surface of tumor cells by HLA molecules 1 • The PRAME peptide can be targeted by T - cell receptors (TCRs) engineered by Immatics, thus overcoming limitations of classical antibodies and CAR T - cell therapies not able to access intracellular targets 1,2 • PRAME has multiple functions in tumor biology enhancing tumor cell survival, tumor proliferation and resistance to apoptosis #,3,4 • PRAME expression has been associated with poor prognosis incl. shorter survival 5,6,7,8 • PRAME is homogenously expressed in tumor tissue 9 4 sqNSCLC Ovarian Cancer PRAME RNA detection in tumor samples (ISH) Anzutresgene autoleucel (anzu - cel, formerly IMA203), # Activation of proliferative and survival pathways, including PI3K/AKT/mTOR 3 , and inhibition of retinoic acid signaling preventing retinoic acid - induced differentiation and apoptosis 4 1 Wermke et al., 2025; 2 Chandran et al., 2019, 3 Yu et al., 2023; 4 Epping et al., 2005; 5 Al - Khadairi & Decock. 2019; 6 Naik et al., 2021; 7 Gezgin et al., 2017; 8 Field et al., 2016; 9 Hukelmann et al., SITC 2022. PRAME anzu - cel (IMA203)
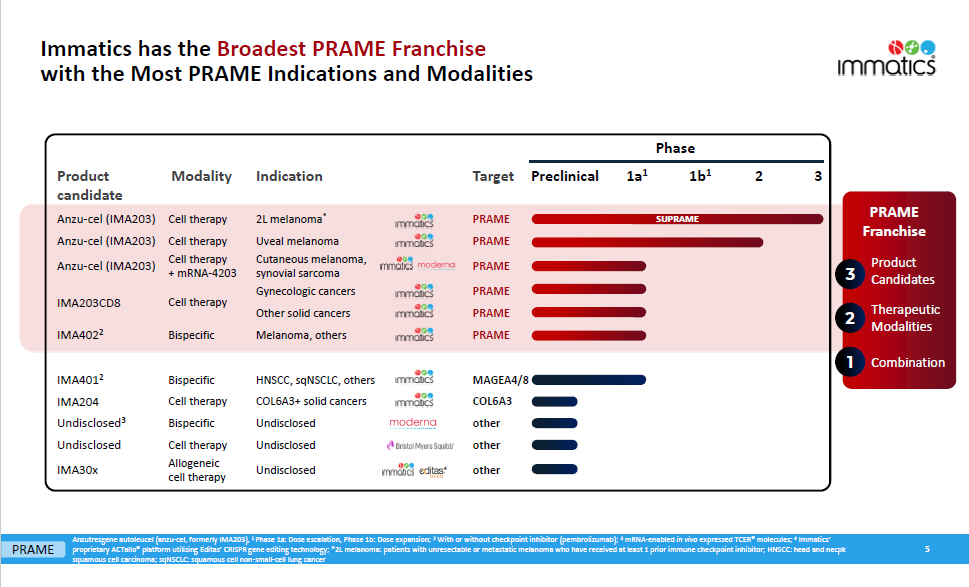
T a r ge t Indication Modality PRAME PRAME Product candid a t e Anzu - cel (IMA203) Anzu - cel (IMA203) PRAME Cell therapy Cell therapy Cell therapy + mRNA - 4203 Anzu - cel (IMA203) Cell therapy IMA203CD8 PRAME PRAME PRAME 2L melanoma * Uveal melanoma Cutaneous melanoma, synovial sarcoma Gynecologic cancers Other solid cancers Melanoma, others Bispecific IMA402 2 M A G E A4/8 COL6A3 other other HNSCC, sqNSCLC, others COL6A3+ solid cancers Undisclosed Undisclosed IMA401 2 IMA204 Undisclose d 3 Undisclosed other Undisclosed Bispecific Cell therapy Bispecific Cell therapy Allogeneic cell therapy IMA30x Preclinical 1a 1 1b 1 2 3 SUPRAME Phase 4 5 Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Phase 1a: Dose escalation, Phase 1b: Dose expansion; 2 With or without checkpoint inhibitor (pembrolizumab); 3 mRNA - enabled in vivo expressed TCER® molecules; 4 Immatics’ proprietary ACTallo® platform utilizing Editas’ CRISPR gene editing technology; *2L melanoma: patients with unresectable or metastatic melanoma who have received at least 1 prior immune checkpoint inhibitor; HNSCC: head and necpk squamous cell carcinoma; sqNSCLC: squamous cell non - small - cell lung cancer Product Candid a t es The r apeutic Modalities 3 2 PRAME Franchise 1 Combination PRAME Immatics has the Broadest PRAME Franchise with the Most PRAME Indications and Modalities
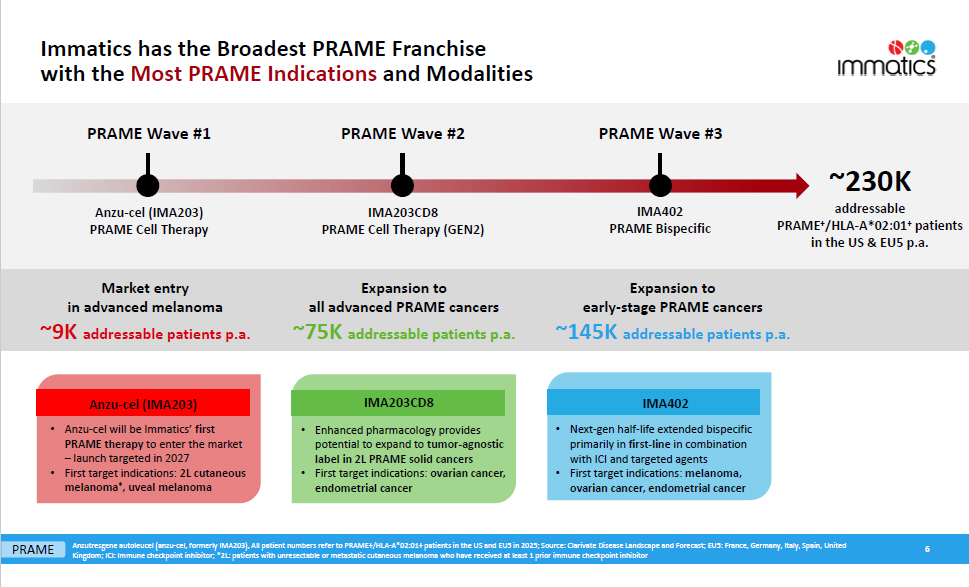
Immatics has the Broadest PRAME Franchise with the Most PRAME Indications and Modalities PRAME Wave #2 PRAME Wave #3 Anzutresgene autoleucel (anzu - cel, formerly IMA203), All patient numbers refer to PRAME+/HLA - A*02:01+ patients in the US and EU5 in 2025; Source: Clarivate Disease Landscape and Forecast; EU5: France, Germany, Italy, Spain, United Kingdom; ICI: Immune checkpoint inhibitor; *2L: patients with unresectable or metastatic cutaneous melanoma who have received at least 1 prior immune checkpoint inhibitor ~230K addressable PRAME + /HLA - A*02:01 + patients in the US & EU5 p.a. IMA203CD8 PRAME Cell Therapy (GEN2) IMA402 PRAME Bispecific Market entry in advanced melanoma ~9K addressable patients p.a. Expansion to all advanced PRAME cancers ~75K addressable patients p.a. Expansion to early - stage PRAME cancers ~145K addressable patients p.a. • Enhanced pharmacology provides potential to expand to tumor - agnostic label in 2L PRAME solid cancers • First target indications: ovarian cancer, endometrial cancer IMA203CD8 • Next - gen half - life extended bispecific primarily in first - line in combination with ICI and targeted agents • First target indications: melanoma, ovarian cancer, endometrial cancer IMA402 • Anzu - cel will be Immatics’ first PRAME therapy to enter the market – launch targeted in 2027 • First target indications: 2L cutaneous melanoma * , uveal melanoma Anzu - cel (IMA203) PRAME Wave #1 Anzu - cel (IMA203) PRAME Cell Therapy 6 PRAME
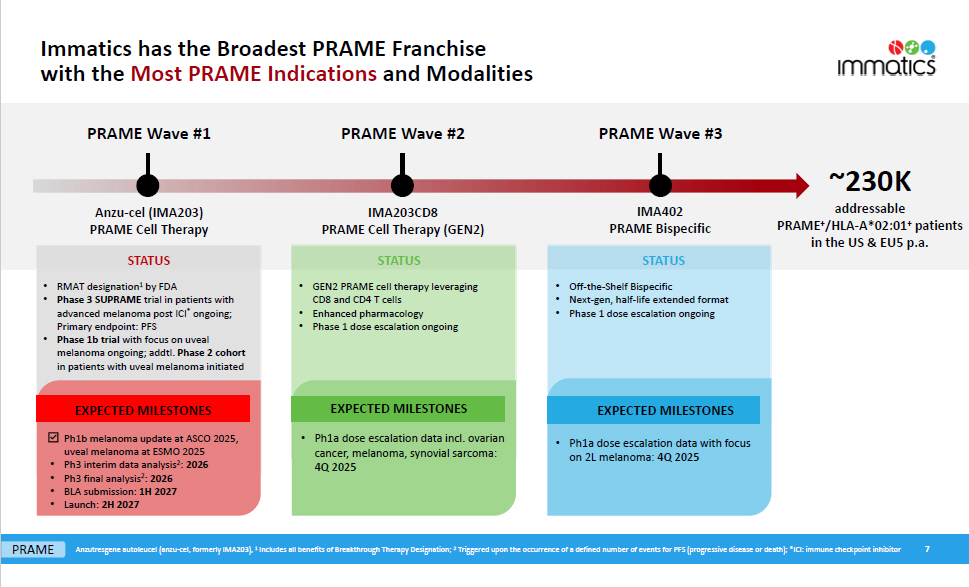
Immatics has the Broadest PRAME Franchise with the Most PRAME Indications and Modalities PRAME Wave #1 PRAME Wave #2 PRAME Wave #3 ~230K addressable PRAME + /HLA - A*02:01 + patients in the US & EU5 p.a. Anzu - cel (IMA203) PRAME Cell Therapy IMA203CD8 PRAME Cell Therapy (GEN2) IMA402 PRAME Bispecific • Ph1a dose escalation data incl. ovarian cancer, melanoma, synovial sarcoma: 4Q 2025 EXPECTED MILESTONES • Ph1a dose escalation data with focus on 2L melanoma: 4Q 2025 EXPECTED MILESTONES Ph1b melanoma update at ASCO 2025, uveal melanoma at ESMO 2025 • Ph3 interim data analysis 2 : 2026 • Ph3 final analysis 2 : 2026 • BLA submission: 1H 2027 • Launch: 2H 2027 EXPECTED MILESTONES S TA T U S S TA T U S S TA T U S • GEN2 PRAME cell therapy leveraging CD8 and CD4 T cells • Enhanced pharmacology • Phase 1 dose escalation ongoing • Off - the - Shelf Bispecific • Next - gen, half - life extended format • Phase 1 dose escalation ongoing • RMAT designation 1 by FDA • Phase 3 SUPRAME trial in patients with advanced melanoma post ICI * ongoing; Primary endpoint: PFS • Phase 1b trial with focus on uveal melanoma ongoing; addtl. Phase 2 cohort in patients with uveal melanoma initiated Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Includes all benefits of Breakthrough Therapy Designation; 2 Triggered upon the occurrence of a defined number of events for PFS (progressive disease or death); *ICI: immune checkpoint inhibitor 7 PRAME
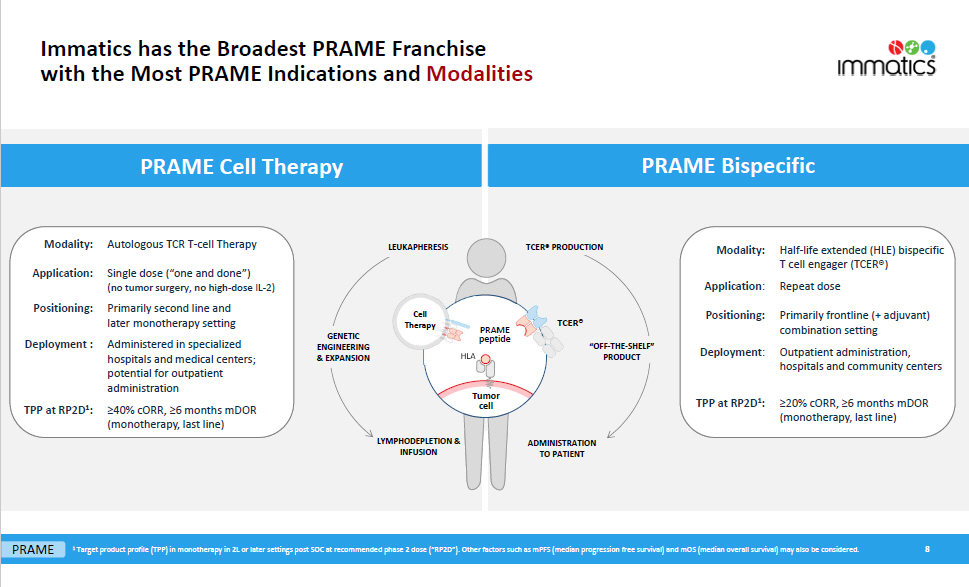
8 PRAME 1 Target product profile (TPP) in monotherapy in 2L or later settings post SOC at recommended phase 2 dose (“RP2D”). Other factors such as mPFS (median progression free survival) and mOS (median overall survival) may also be considered. LYMPHODEPLETION & INFUSION Tumor cell HLA PRAME pep t ide ADMINISTRATION TO PATIENT LEUKAPHERESIS GENETIC E N GI N EE R I NG & EXPANSION TCER® PRODUCTION “OFF - THE - SHELF” PRODUCT PRAME Bispecific Mod ality: Half - life extended (HLE) bispecific T cell engager (TCER®) Repeat dose Application : Positioning: Primarily frontline (+ adjuvant) combination setting Outpatient administration, hospitals and community centers Deployme nt : ≥20% cORR, ≥6 months mDOR (monotherapy, last line) TPP at RP2D 1 : PRAME Cell Therapy Autologous TCR T - cell Therapy Mod ality: Single dose (“one and done”) (no tumor surgery, no high - dose IL - 2) Application: Positioning: Deployment : Primarily second line and later monotherapy setting Administered in specialized hospitals and medical centers; potential for outpatient administration ≥40% cORR, ≥6 months mDOR (monotherapy, last line) TPP at RP2D 1 : Cell T h era py TCER® Immatics has the Broadest PRAME Franchise with the Most PRAME Indications and Modalities
Anzu - cel (IMA203) PRAME Cell Therapy Market Entry in Advanced Melanoma PRAME Wave #1 9 Anzutresgene autoleucel (anzu - cel, formerly IMA203)
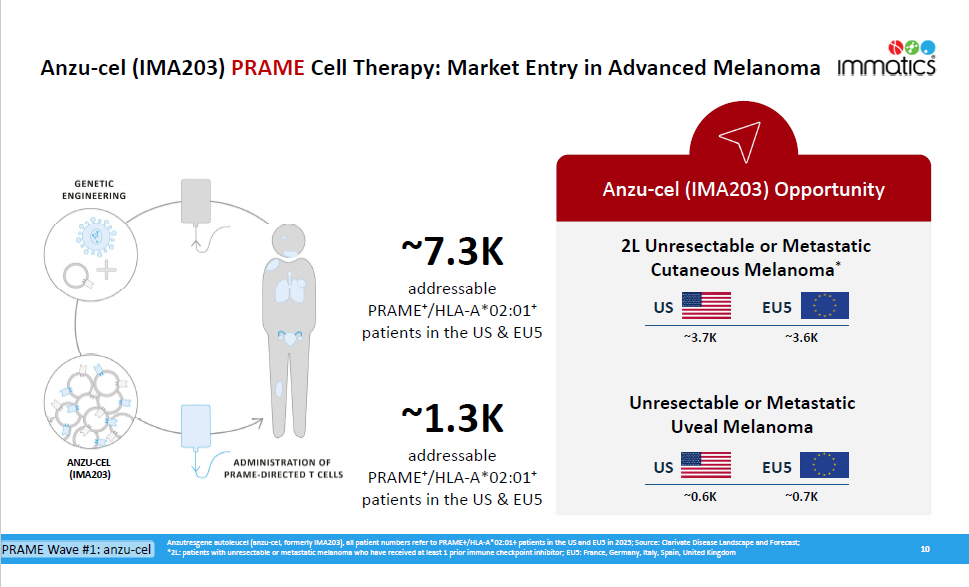
Anzu - cel (IMA203) PRAME Cell Therapy: Market Entry in Advanced Melanoma 10 Anzu - cel (IMA203) Opportunity ~7.3K addressable PRAME + /HLA - A*02:01 + patients in the US & EU5 ~1.3K addressable PRAM E + /HLA - A*02:0 1 + patients in the US & EU5 Anzutresgene autoleucel (anzu - cel, formerly IMA203), all patient numbers refer to PRAME+/HLA - A*02:01+ patients in the US and EU5 in 2025; Source: Clarivate Disease Landscape and Forecast; *2L: patients with unresectable or metastatic melanoma who have received at least 1 prior immune checkpoint inhibitor; EU5: France, Germany, Italy, Spain, United Kingdom PRAME Wave #1: anzu - cel 2L Unresectable or Metastatic Cutaneous Melanoma * US EU5 ~3.7K ~3.6K Unresectable or Metastatic Uveal Melanoma US EU5 ~0.6K ~0.7K ANZU - CEL (IMA203)
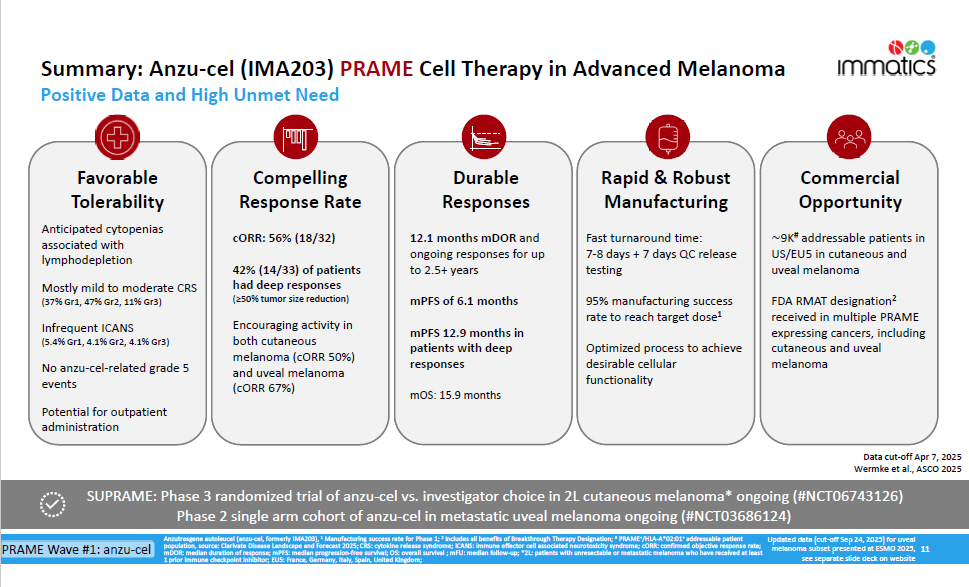
SUPRAME: Phase 3 randomized trial of anzu - cel vs. investigator choice in 2L cutaneous melanoma* ongoing (#NCT06743126) Phase 2 single arm cohort of anzu - cel in metastatic uveal melanoma ongoing (#NCT03686124) mDOR: median duration of response; mPFS: median progression - free survival; OS: overall survival ; mFU: median follow - up; *2L: patients with unresectable or metastatic melanoma who have received at least 1 prior immune checkpoint inhibitor; EU5: France, Germany, Italy, Spain, United Kingdom; Summary: Anzu - cel (IMA203) PRAME Cell Therapy in Advanced Melanoma Positive Data and High Unmet Need Favorable T ole r abili t y Anticipated cytopenias associated with lymphodepletion Mostly mild to moderate CRS (37% Gr1, 47% Gr2, 11% Gr3) Infrequent ICANS (5.4% Gr1, 4.1% Gr2, 4.1% Gr3) No anzu - cel - related grade 5 events Potential for outpatient administration Compelling Response Rate cORR: 56% (18/32) 42% (14/33) of patients had deep responses (≥50% tumor size reduction) Encouraging activity in both cutaneous melanoma (cORR 50%) and uveal melanoma (cORR 67%) Durable R e sponses 12.1 months mDOR and ongoing responses for up to 2.5+ years mPFS of 6.1 months mPFS 12.9 months in patients with deep responses mOS: 15.9 months Rapid & Robust Manufacturing Fast turnaround time: 7 - 8 days + 7 days QC release testing 95% manufacturing success rate to reach target dose 1 Optimized process to achieve desirable cellular functionality Commercial Opportunity ∼ 9K # addressable patients in US/EU5 in cutaneous and uveal melanoma FDA RMAT designation 2 received in multiple PRAME expressing cancers, including cutaneous and uveal melanoma Data cut - off Apr 7, 2025 Wermke et al., ASCO 2025 PRAME Wave #1: anzu - cel Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Manufacturing success rate for Phase 1; 2 Includes all benefits of Breakthrough Therapy Designation; # PRAME + /HLA - A*02:01 + addressable patient Updated data (cut - off Sep 24, 2025) for uveal population, source: Clarivate Disease Landscape and Forecast 2025; CRS: cytokine release syndrome; ICANS: immune effector cell associated neurotoxicity syndrome; cORR: confirmed objective response rate; melanoma subset presented at ESMO 2025, 11 see separate slide deck on website
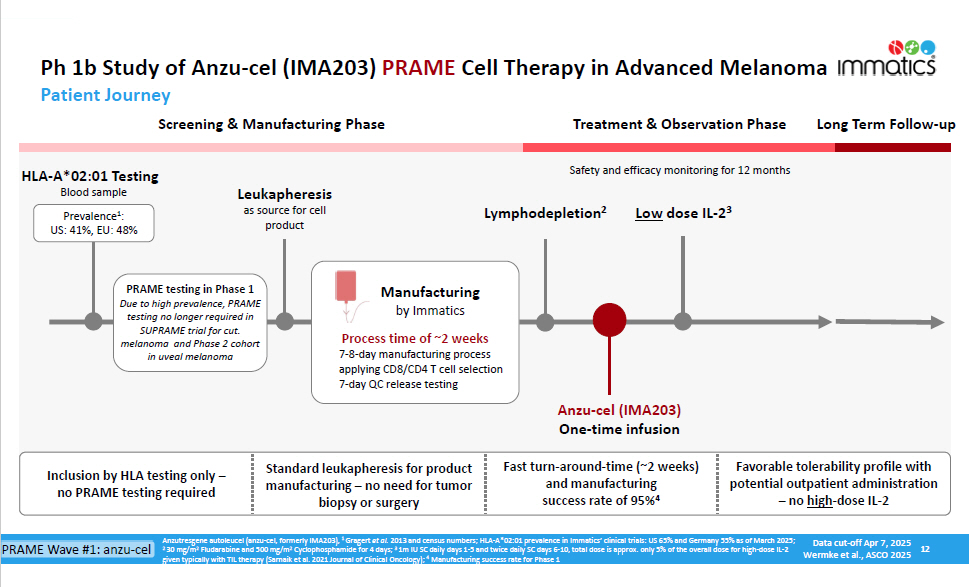
Ph 1b Study of Anzu - cel (IMA203) PRAME Cell Therapy in Advanced Melanoma 12 Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Gragert et al. 2013 and census numbers; HLA - A*02:01 prevalence in Immatics’ clinical trials: US 65% and Germany 55% as of March 2025; 2 30 mg/m 2 Fludarabine and 500 mg/m 2 Cyclophosphamide for 4 days; 3 1m IU SC daily days 1 - 5 and twice daily SC days 6 - 10, total dose is approx. only 5% of the overall dose for high - dose IL - 2 given typically with TIL therapy (Sarnaik et al. 2021 Journal of Clinical Oncology); 4 Manufacturing success rate for Phase 1 HLA - A*02:01 Testing Blood sample Patient Journey Screening & Manufacturing Phase Treatment & Observation Phase Long Term Follow - up Manu f acturing by Immatics Anzu - cel (IMA203) One - time infusion Safety and efficacy monitoring for 12 months Lymphodepletion 2 Low dose IL - 2 3 Leukapheresis as source for cell product Process time of ~2 weeks 7 - 8 - day manufacturing process applying CD8/CD4 T cell selection 7 - day QC release testing PRAME testing in Phase 1 Due to high prevalence, PRAME testing no longer required in SUPRAME trial for cut. melanoma and Phase 2 cohort in uveal melanoma Inclusion by HLA testing only – no PRAME testing required Fast turn - around - time (~2 weeks) and manufacturing success rate of 95% 4 Favorable tolerability profile with potential outpatient administration – no high - dose IL - 2 Standard leukapheresis for product manufacturing – no need for tumor biopsy or surgery Prevalence 1 : US: 41%, EU: 48% Data cut - off Apr 7, 2025 Wermke et al., ASCO 2025 PRAME Wave #1: anzu - cel
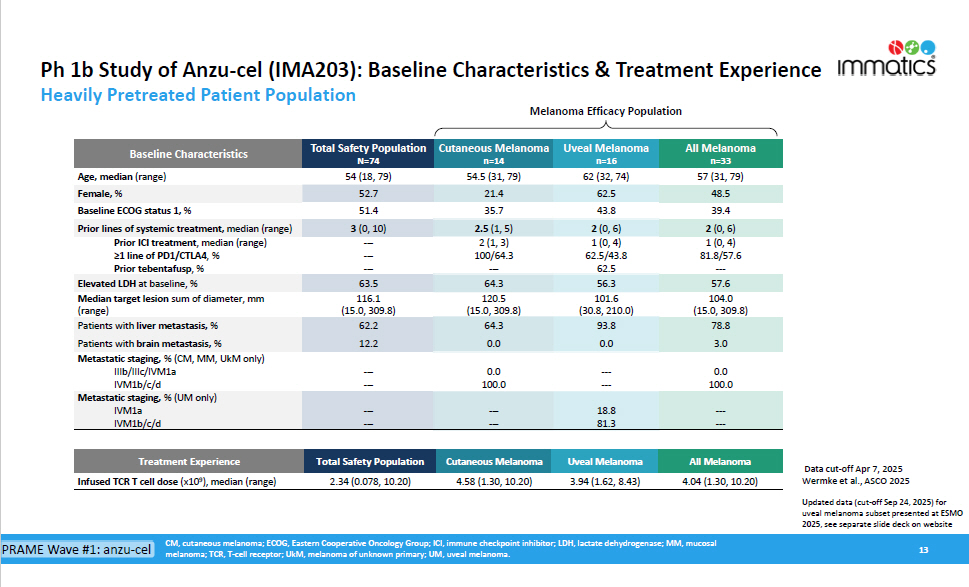
Ph 1b Study of Anzu - cel (IMA203): Baseline Characteristics & Treatment Experience CM, cutaneous melanoma; ECOG, Eastern Cooperative Oncology Group; ICI, immune checkpoint inhibitor; LDH, lactate dehydrogenase; MM, mucosal melanoma; TCR, T - cell receptor; UkM, melanoma of unknown primary; UM, uveal melanoma. 13 n=33 57 (31, 79) n=16 62 (32, 74) n=14 54.5 (31, 79) N=74 54 (18, 79) Age, median (range) 48.5 62.5 21.4 52.7 Female, % 39.4 43.8 35.7 51.4 Baseline ECOG status 1, % 2 (0, 6) 2 (0, 6) 2.5 (1, 5) 3 (0, 10) Prior lines of systemic treatment, median (range) 1 (0, 4) 1 (0, 4) 2 (1, 3) --- Prior ICI treatment , median (range) 81.8/57.6 62.5/43.8 100/64.3 --- ≥1 line of PD1/CTLA4 , % --- 62.5 --- --- Prior tebentafusp , % 57.6 56.3 64.3 63.5 Elevated LDH at baseline, % 104.0 101.6 120.5 116.1 Median target lesion sum of diameter, mm (15.0, 309.8) (30.8, 210.0) (15.0, 309.8) (15.0, 309.8) (range) 78.8 93.8 64.3 62.2 Patients with liver metastasis, % 3.0 0.0 0.0 12.2 Patients with brain metastasis, % 0.0 --- 0.0 --- Metastatic staging, % (CM, MM, UkM only) IIIb/IIIc/IVM1a 100.0 --- 100.0 --- IVM1b/c/d --- --- 18.8 81.3 --- --- --- --- Metastatic staging, % (UM only) IVM1a IVM1b/c/d Uveal Melanoma All Melanoma Cutaneous Melanoma Total Safety Population Baseline Characteristics Heavily Pretreated Patient Population Melanoma Efficacy Population Data cut - off Apr 7, 2025 Wermke et al., ASCO 2025 All Melanoma 4.04 (1.30, 10.20) Uveal Melanoma 3.94 (1.62, 8.43) Cutaneous Melanoma 4.58 (1.30, 10.20) Total Safety Population 2.34 (0.078, 10.20) Treatment Experience Infused TCR T cell dose (x10 9 ), median (range) Updated data (cut - off Sep 24, 2025) for uveal melanoma subset presented at ESMO 2025, see separate slide deck on website PRAME Wave #1: anzu - cel
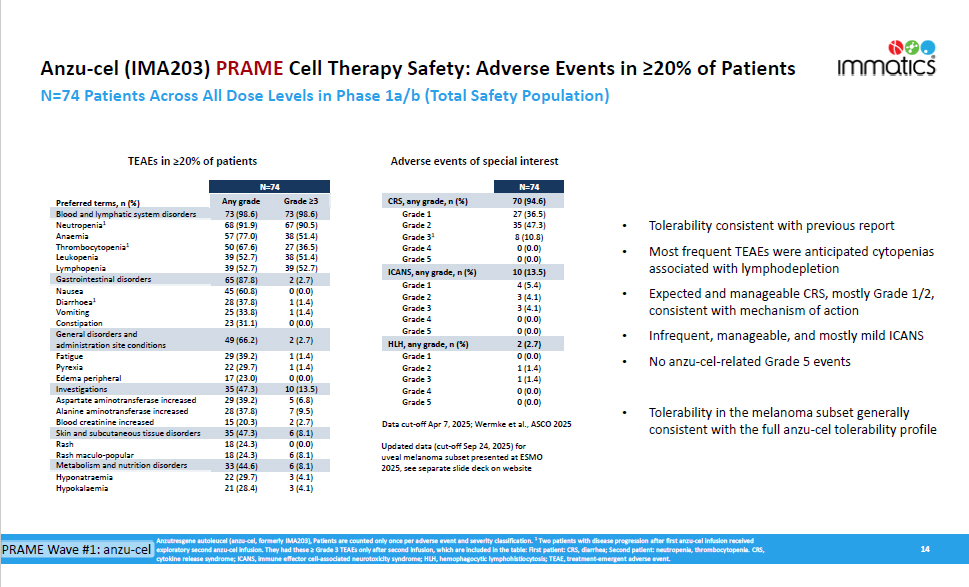
Anzu - cel (IMA203) PRAME Cell Therapy Safety: Adverse Events in ≥20% of Patients N=74 Patients Across All Dose Levels in Phase 1a/b (Total Safety Population) 14 Anzutresgene autoleucel (anzu - cel, formerly IMA203), Patients are counted only once per adverse event and severity classification. 1 Two patients with disease progression after first anzu - cel infusion received cytokine release syndrome; ICANS, immune effector cell - associated neurotoxicity syndrome; HLH, hemophagocytic lymphohistiocytosis; TEAE, treatment - emergent adverse event. N=74 Preferred terms, n (%) Any grade Grade ≥3 Blood and lymphatic system disorders 73 (98.6) 73 (98.6) 2 (2.7) 65 (87.8) Gastrointestinal disorders 0 (0.0) 45 (60.8) Nausea 1 (1.4) 28 (37.8) Diarrhoea 1 1 (1.4) 25 (33.8) Vomiting 0 (0.0) 23 (31.1) Constipation General disorders and N=74 70 (94.6) CRS, any grade, n (%) 27 (36.5) Grade 1 35 (47.3) Grade 2 67 (90.5) 68 (91.9) Neutropenia 1 8 (10.8) Grade 3 1 38 (51.4) 57 (77.0) Anaemia 0 (0.0) Grade 4 27 (36.5) 50 (67.6) Thrombocytopenia 1 0 (0.0) Grade 5 38 (51.4) 39 (52.7) Leukopenia 10 (13.5) ICANS, any grade, n (%) 39 (52.7) 39 (52.7) Lymphopenia 2 (2.7) HLH, any grade, n (%) 2 (2.7) 49 (66.2) administration site conditions 0 (0.0) Grade 1 1 (1.4) 29 (39.2) Fatigue 1 (1.4) Grade 2 1 (1.4) 22 (29.7) Pyrexia 1 (1.4) Grade 3 0 (0.0) 17 (23.0) Edema peripheral 0 (0.0) Grade 4 10 (13.5) 35 (47.3) Investigations 0 (0.0) Grade 5 5 (6.8) 29 (39.2) Aspartate aminotransferase increased 7 (9.5) 28 (37.8) Alanine aminotransferase increased 2 (2.7) 15 (20.3) Blood creatinine increased 6 (8.1) 35 (47.3) Skin and subcutaneous tissue disorders 0 (0.0) 6 (8.1) 18 (24.3) 18 (24.3) Rash Rash maculo - popular 6 (8.1) 33 (44.6) Metabolism and nutrition disorders 3 (4.1) 3 (4.1) 22 (29.7) 21 (28.4) Hyponatraemia Hypokalaemia • Tolerability consistent with previous report • Most frequent TEAEs were anticipated cytopenias associated with lymphodepletion • Expected and manageable CRS, mostly Grade 1/2, consistent with mechanism of action • Infrequent, manageable, and mostly mild ICANS • No anzu - cel - related Grade 5 events • Tolerability in the melanoma subset generally consistent with the full anzu - cel tolerability profile Adverse events of special interest TEAEs in ≥20% of patients 4 (5.4) 3 (4.1) 3 (4.1) 0 (0.0) 0 (0.0) Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 PRAME Wave #1: anzu - cel exploratory second anzu - cel infusion. They had these ≥ Grade 3 TEAEs only after second infusion, which are included in the table: First patient: CRS, diarrhea; Second patient: neutropenia, thrombocytopenia. CRS, Data cut - off Apr 7, 2025; Wermke et al., ASCO 2025 Updated data (cut - off Sep 24, 2025) for uveal melanoma subset presented at ESMO 2025, see separate slide deck on website
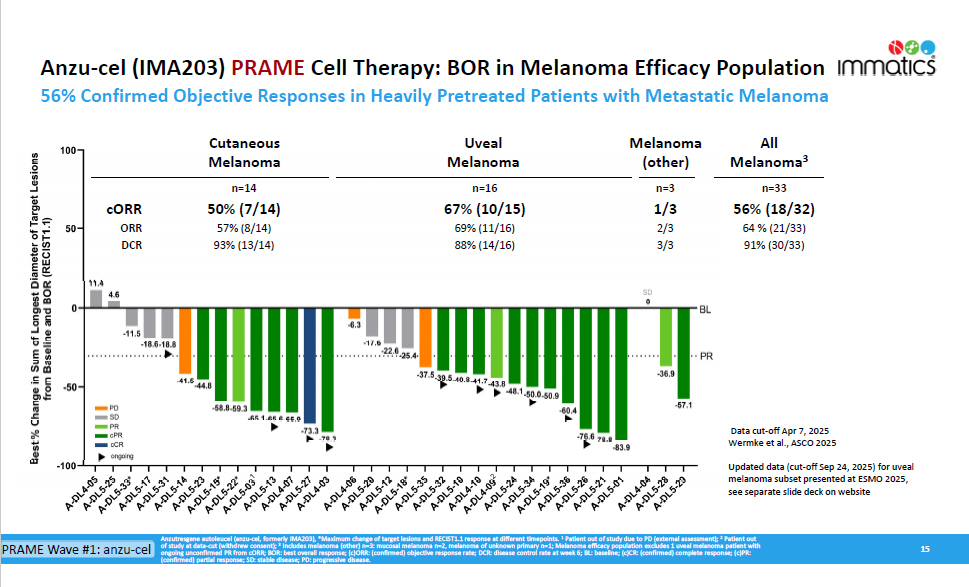
Anzu - cel (IMA203) PRAME Cell Therapy: BOR in Melanoma Efficacy Population 56% Confirmed Objective Responses in Heavily Pretreated Patients with Metastatic Melanoma 15 Anzutresgene autoleucel (anzu - cel, formerly IMA203), *Maximum change of target lesions and RECIST1.1 response at different timepoints. 1 Patient out of study due to PD (external assessment); 2 Patient out of study at data - cut (withdrew consent); 3 Includes melanoma (other) n=3: mucosal melanoma n=2, melanoma of unknown primary n=1; Melanoma efficacy population excludes 1 uveal melanoma patient with ongoing unconfirmed PR from cORR; BOR: best overall response; (c)ORR: (confirmed) objective response rate; DCR: disease control rate at week 6; BL: baseline; (c)CR: (confirmed) complete response; (c)PR: (confirmed) partial response; SD: stable disease; PD: progressive disease. n=33 56% (18/32) n=3 1/3 n=16 67% (10/15) n=14 50% (7/14) cORR 64 % (21/33) 2/3 69% (11/16) 57% (8/14) ORR 91% (30/33) 3/3 88% (14/16) 93% (13/14) DCR Cu t aneous Melanoma Uveal Melanoma Melanoma (other) All Melanoma 3 PRAME Wave #1: anzu - cel Data cut - off Apr 7, 2025 Wermke et al., ASCO 2025 Updated data (cut - off Sep 24, 2025) for uveal melanoma subset presented at ESMO 2025, see separate slide deck on website
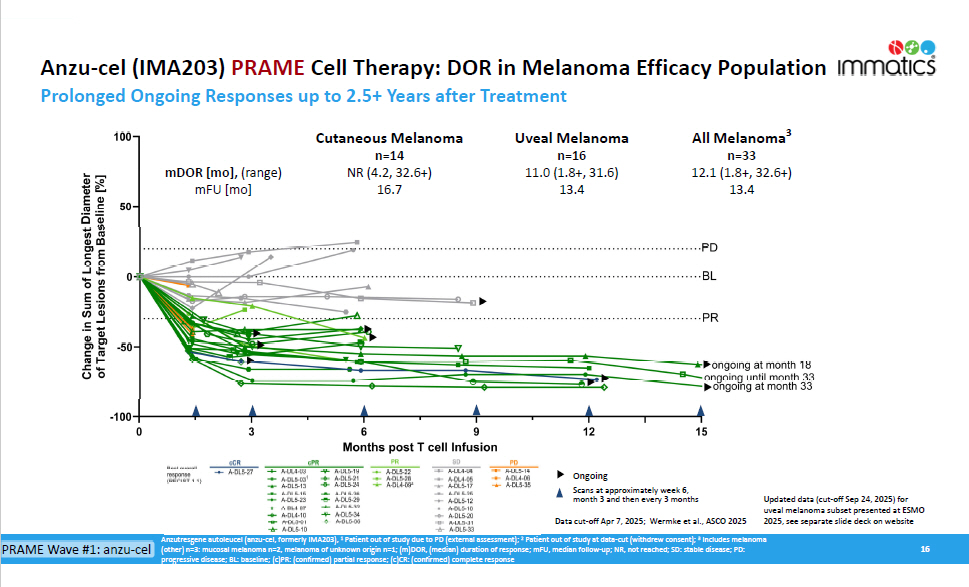
Anzu - cel (IMA203) PRAME Cell Therapy: DOR in Melanoma Efficacy Population Prolonged Ongoing Responses up to 2.5+ Years after Treatment 16 Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Patient out of study due to PD (external assessment); 2 Patient out of study at data - cut (withdrew consent); 3 Includes melanoma (other) n=3: mucosal melanoma n=2, melanoma of unknown origin n=1; (m)DOR, (median) duration of response; mFU, median follow - up; NR, not reached; SD: stable disease; PD: progressive disease; BL: baseline; (c)PR: (confirmed) partial response; (c)CR: (confirmed) complete response Ongoing Scans at approximately week 6, month 3 and then every 3 months All Melanoma 3 Uveal Melanoma Cutaneous Melanoma n=33 n=16 n=14 12.1 (1.8+, 32.6+) 11.0 (1.8+, 31.6) NR (4.2, 32.6+) mDOR [mo], (range) 13.4 13.4 16.7 mFU [mo] PRAME Wave #1: anzu - cel Data cut - off Apr 7, 2025; Wermke et al., ASCO 2025 Updated data (cut - off Sep 24, 2025) for uveal melanoma subset presented at ESMO 2025, see separate slide deck on website
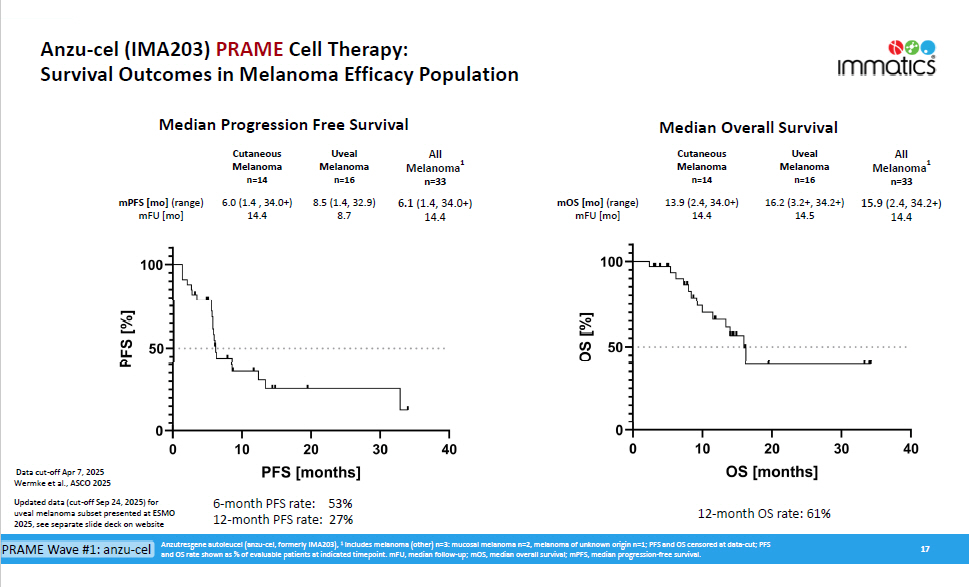
Anzu - cel (IMA203) PRAME Cell Therapy: Survival Outcomes in Melanoma Efficacy Population 17 All 1 Melanoma Melanoma Melanoma 1 Melanoma Melanoma Melanoma n=33 n=16 n=14 n=33 n=16 n=14 15.9 (2.4, 34.2+) 16.2 (3.2+, 34.2+) 13.9 (2.4, 34.0+) mOS [mo] (range) 6.1 (1.4, 34.0+) 8.5 (1.4, 32.9) 6.0 (1.4 , 34.0+) mPFS [mo] (range) 14.4 14.5 14.4 mFU [mo] 14.4 8.7 14.4 mFU [mo] Median Progression Free Survival Cutaneous Uveal All Median Overall Survival Cutaneous Uveal 12 - month OS rate: 61% Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Includes melanoma (other) n=3: mucosal melanoma n=2, melanoma of unknown origin n=1; PFS and OS censored at data - cut; PFS and OS rate shown as % of evaluable patients at indicated timepoint. mFU, median follow - up; mOS, median overall survival; mPFS, median progression - free survival. Data cut - off Apr 7, 2025 Wermke et al., ASCO 2025 53% 6 - month PFS rate: Updated data (cut - off Sep 24, 2025) for 27% 12 - month PFS rate: uveal melanoma subset presented at ESMO 2025, see separate slide deck on website PRAME Wave #1: anzu - cel
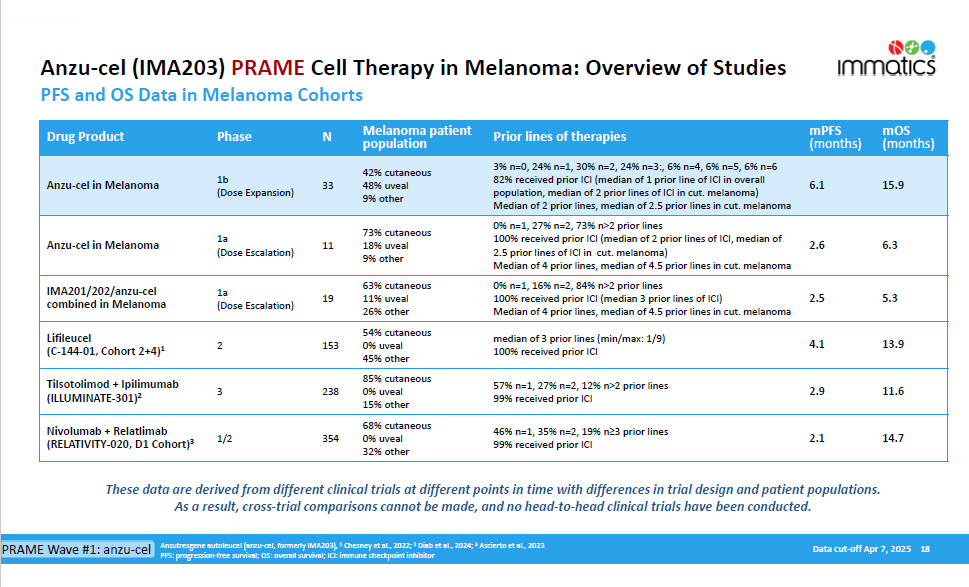
Anzu - cel (IMA203) PRAME Cell Therapy in Melanoma: Overview of Studies PFS and OS Data in Melanoma Cohorts mOS (months) mPFS (months) Prior lines of therapies Melanoma patient population N Phase Drug Product 15.9 6.1 3% n=0, 24% n=1, 30% n=2, 24% n=3:, 6% n=4, 6% n=5, 6% n=6 82% received prior ICI (median of 1 prior line of ICI in overall population, median of 2 prior lines of ICI in cut. melanoma) Median of 2 prior lines, median of 2.5 prior lines in cut. melanoma 42% cutaneous 48% uveal 9% other 33 1b (Dose Expansion) Anzu - cel in Melanoma 6.3 2.6 0% n=1, 27% n=2, 73% n>2 prior lines 100% received prior ICI (median of 2 prior lines of ICI, median of 2.5 prior lines of ICI in cut. melanoma) Median of 4 prior lines, median of 4.5 prior lines in cut. melanoma 73% cutaneous 18% uveal 9% other 11 1a (Dose Escalation) Anzu - cel in Melanoma 5.3 2.5 0% n=1, 16% n=2, 84% n>2 prior lines 100% received prior ICI (median 3 prior lines of ICI) Median of 4 prior lines, median of 4.5 prior lines in cut. melanoma 63% cutaneous 11% uveal 26% other 19 1a (Dose Escalation) IMA201/202/anzu - cel combined in Melanoma 13.9 4.1 median of 3 prior lines (min/max: 1/9) 100% received prior ICI 54% cutaneous 0% uveal 45% other 153 2 Lifileucel (C - 144 - 01, Cohort 2+4) 1 11.6 2.9 57% n=1, 27% n=2, 12% n>2 prior lines 99% received prior ICI 85% cutaneous 0% uveal 15% other 238 3 Tilsotolimod + Ipilimumab (ILLUMINATE - 301) 2 14.7 2.1 46% n=1, 35% n=2, 19% n≥3 prior lines 99% received prior ICI 68% cutaneous 0% uveal 32% other 354 1/2 Nivolumab + Relatlimab (RELATIVITY - 020, D1 Cohort) 3 Data cut - off Apr 7, 2025 18 Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Chesney et al., 2022; 2 Diab et al., 2024; 3 Ascierto et al., 2023 PFS: progression - free survival; OS: overall survival; ICI: immune checkpoint inhibitor These data are derived from different clinical trials at different points in time with differences in trial design and patient populations. As a result, cross - trial comparisons cannot be made, and no head - to - head clinical trials have been conducted. PRAME Wave #1: anzu - cel
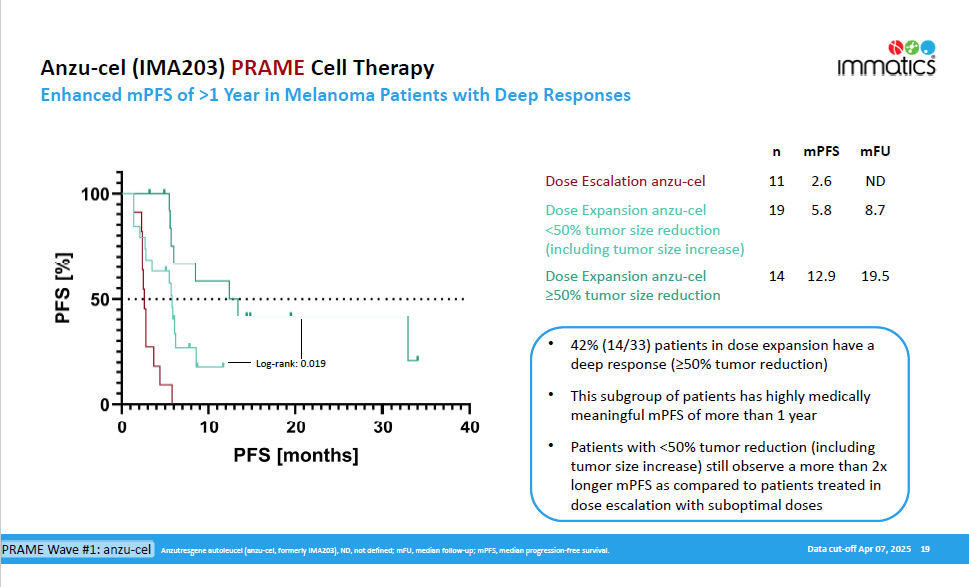
Anzu - cel (IMA203) PRAME Cell Therapy Enhanced mPFS of >1 Year in Melanoma Patients with Deep Responses Data cut - off Apr 07, 2025 19 • 42% (14/33) patients in dose expansion have a deep response (≥50% tumor reduction) • This subgroup of patients has highly medically meaningful mPFS of more than 1 year • Patients with <50% tumor reduction (including tumor size increase) still observe a more than 2x longer mPFS as compared to patients treated in dose escalation with suboptimal doses mFU mPFS n ND 2.6 11 Dose Escalation anzu - cel 8.7 5.8 19 Dose Expansion anzu - cel <50% tumor size reduction (including tumor size increase) 19.5 12.9 14 Dose Expansion anzu - cel ≥50% tumor size reduction Log - rank: 0.019 Anzutresgene autoleucel (anzu - cel, formerly IMA203), ND, not defined; mFU, median follow - up; mPFS, median progression - free survival. PRAME Wave #1: anzu - cel
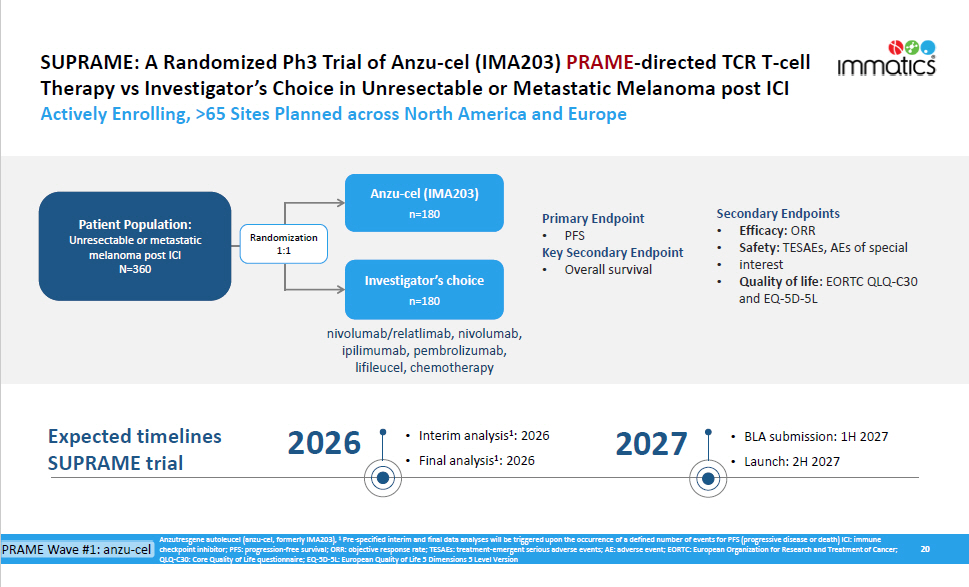
SUPRAME: A Randomized Ph3 Trial of Anzu - cel (IMA203) PRAME - directed TCR T - cell Therapy vs Investigator’s Choice in Unresectable or Metastatic Melanoma post ICI Actively Enrolling, >65 Sites Planned across North America and Europe 20 Anzu - cel (IMA203) n=180 Investigator’s choice n=180 Primary Endpoint • P F S Key Secondary Endpoint • Overall survival Randomization 1:1 Patient Population: Unresectable or metastatic melanoma post ICI N=360 nivolumab/relatlimab, nivolumab, ipilimumab, pembrolizumab, lifileucel, chemotherapy Secondary Endpoints • Efficacy: ORR • Safety: TESAEs, AEs of special • interest • Quality of life: EORTC QLQ - C30 and EQ - 5D - 5L Expected timelines SUPRAME trial • Interim analysis 1 : 2026 • Final analysis 1 : 2026 2026 • BLA submission: 1H 2027 • Launch: 2H 2027 2027 Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Pre - specified interim and final data analyses will be triggered upon the occurrence of a defined number of events for PFS (progressive disease or death) ICI: immune PRAME Wave #1: anzu - cel checkpoint inhibitor; PFS: progression - free survival; ORR: objective response rate; TESAEs: treatment - emergent serious adverse events; AE: adverse event; EORTC: European Organization for Research and Treatment of Cancer; QLQ - C30: Core Quality of Life questionnaire; EQ - 5D - 5L: European Quality of Life 5 Dimensions 5 Level Version
Cell Therapy Manufacturing Facility To Support Anzu - cel BLA and Commercialization 21 • ~100,000 sq ft state - of - the - art research & GMP manufacturing facility • Modular design for efficient and cost - effective scalability - total of 8 manufacturing suites, plus further expansion space • Capacity sufficient to serve early - stage and registration - directed clinical trials as well as planned commercial supply • In - house manufacturing and QC allows full control of process, product and costs • Located in the Houston Metropolitan Area, Texas, offering economic labor and operating costs and talent pool highly qualified in cell therapy manufacturing & QC Anzutresgene autoleucel (anzu - cel, formerly IMA203); BLA: Biologics License Application PRAME Wave #1: anzu - cel

IMA203CD8 PRAME Cell Therapy (GEN2) Expansion to all Advanced PRAME Cancers PRAME Wave #2 22
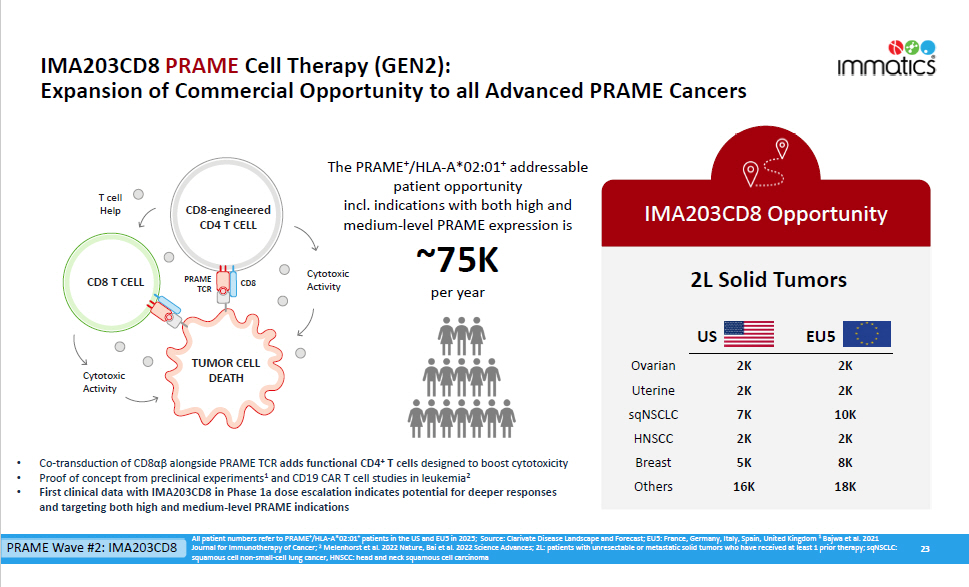
IMA203CD8 PRAME Cell Therapy (GEN2): Expansion of Commercial Opportunity to all Advanced PRAME Cancers 23 IMA203CD8 Opportunity All patient numbers refer to PRAME + /HLA - A*02:01 + patients in the US and EU5 in 2025; Source: Clarivate Disease Landscape and Forecast; EU5: France, Germany, Italy, Spain, United Kingdom 1 Bajwa et al. 2021 Journal for Immunotherapy of Cancer; 2 Melenhorst et al. 2022 Nature, Bai et al. 2022 Science Advances; 2L: patients with unresectable or metastatic solid tumors who have received at least 1 prior therapy; sqNSCLC: squamous cell non - small - cell lung cancer, HNSCC: head and neck squamous cell carcinoma The PRAME + /HLA - A*02:01 + addressable patient opportunity incl. indications with both high and medium - level PRAME expression is ~75K per year • Co - transduction of CD8αβ alongside PRAME TCR adds functional CD4 + T cells designed to boost cytotoxicity • Proof of concept from preclinical experiments 1 and CD19 CAR T cell studies in leukemia 2 • First clinical data with IMA203CD8 in Phase 1a dose escalation indicates potential for deeper responses and targeting both high and medium - level PRAME indications 2K 2K O v arian 2K 2K Uterine 10K 7K sqNSC L C 2K 2K HNSCC 8K 5K Breast 18K 16K Others 2L Solid Tumors US EU5 TUMOR CELL DEATH CD8 - enginee r ed CD4 T CELL C y tot ox ic Activity CD8 T CELL T cell Help C y tot ox ic Activity CD8 PRAME TCR PRAME Wave #2: IMA203CD8
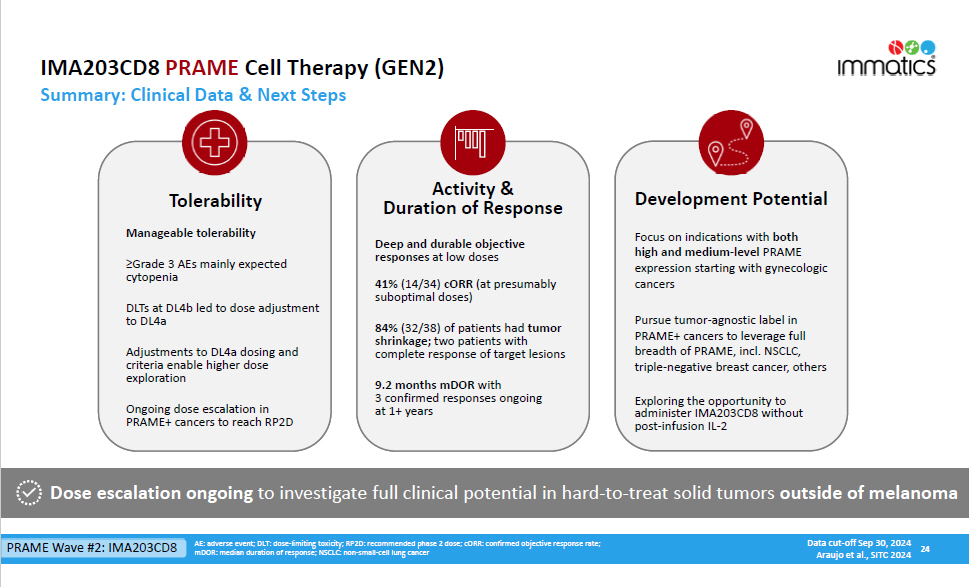
24 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024 Dose escalation ongoing to investigate full clinical potential in hard - to - treat solid tumors outside of melanoma Tolerability Manageable tolerability ≥Grade 3 AEs mainly expected cytopenia DLTs at DL4b led to dose adjustment to DL4a Adjustments to DL4a dosing and criteria enable higher dose exploration Ongoing dose escalation in PRAME+ cancers to reach RP2D Deep and durable objective responses at low doses 41% (14/34) cORR (at presumably suboptimal doses) 84% (32/38) of patients had tumor shrinkage; two patients with complete response of target lesions 9.2 months mDOR with 3 confirmed responses ongoing at 1+ years Activity & Duration of Response Development Potential Focus on indications with both high and medium - level PRAME expression startin CD g 8 with gynecologic cancers Pursue tumor - agnostic label in PRAME+ cancers to leverage full breadth of PRAME, incl. NSCLC, triple - negative breast cancer, others Exploring the opportunity to administer IMA203CD8 without post - infusion IL - 2 AE: adverse event; DLT: dose - limiting toxicity; RP2D: recommended phase 2 dose; cORR: confirmed objective response rate; mDOR: median duration of response; NSCLC: non - small - cell lung cancer IMA203CD8 PRAME Cell Therapy (GEN2) Summary: Clinical Data & Next Steps PRAME Wave #2: IMA203CD8
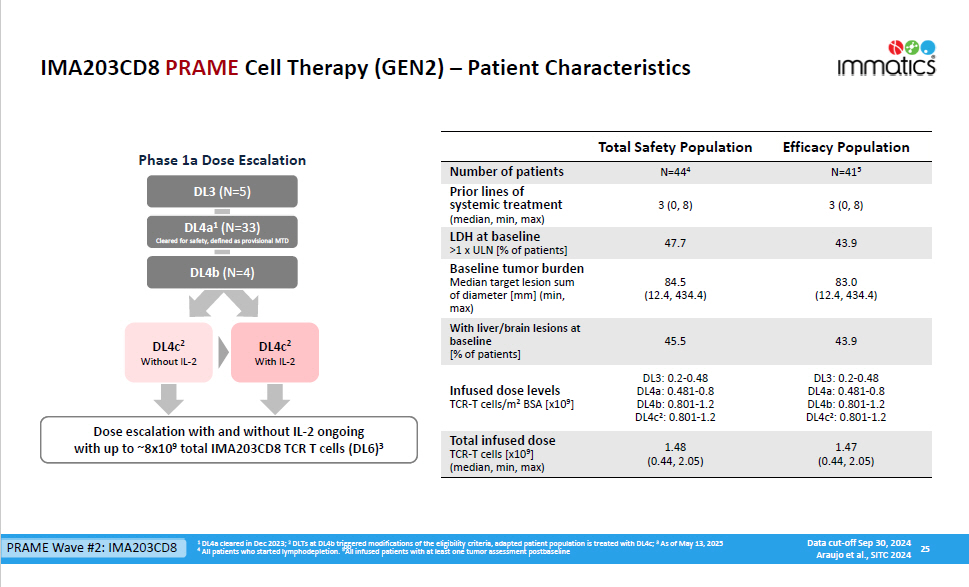
IMA203CD8 PRAME Cell Therapy (GEN2) – Patient Characteristics 25 1 DL4a cleared in Dec 2023; 2 DLTs at DL4b triggered modifications of the eligibility criteria, adapted patient population is treated with DL4c; 3 As of May 13, 2025 4 All patients who started lymphodepletion. 5 All infused patients with at least one tumor assessment postbaseline DL3 (N=5) DL4a 1 (N=33) Cleared for safety, defined as provisional MTD Dose escalation with and without IL - 2 ongoing with up to ~8x10 9 total IMA203CD8 TCR T cells (DL6) 3 DL4b (N=4) Phase 1a Dose Escalation 43.9 47.7 LDH at baseline >1 x ULN [% of patients] Baseline tumor burden 83.0 84.5 Median target lesion sum (12.4, 434.4) (12.4, 434.4) of diameter [mm] (min, max) With liver/brain lesions at 43.9 45.5 baseline [% of patients] DL3: 0.2 - 0.48 DL4a: 0.481 - 0.8 DL3: 0.2 - 0.48 DL4a: 0.481 - 0.8 Infused dose levels DL4b: 0.801 - 1.2 DL4b: 0.801 - 1.2 TCR - T cells/m 2 BSA [x10 9 ] DL4c 2 : 0.801 - 1.2 DL4c 2 : 0.801 - 1.2 Efficacy Population Total Safety Population N=41 5 N=44 4 Number of patients 3 (0, 8) 3 (0, 8) Prior lines of systemic treatment (median, min, max) 1.47 (0.44, 2.05) 1.48 (0.44, 2.05) Total infused dose TCR - T cells [x10 9 ] (median, min, max) PRAME Wave #2: IMA203CD8 DL4c 2 Without IL - 2 DL4c 2 With IL - 2 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024
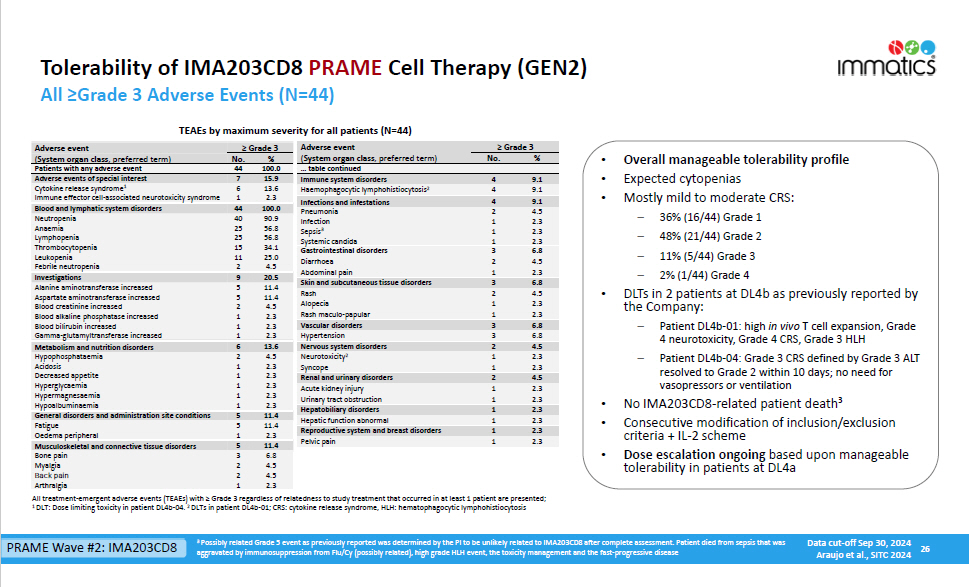
Tolerability of IMA203CD8 PRAME Cell Therapy (GEN2) 26 All ≥Grade 3 Adverse Events (N=44) 11 . 4 5 Musculoskeletal and connective tissue disorders 6.8 4.5 4.5 2.3 3 2 2 1 Bone pain Myalgia Back pain Arthralgia TEAEs by maximum severity for all patients (N=44) ≥ Grade 3 No. % Adverse event ( System organ class , preferred term) ≥ Grade 3 No. % Adverse event ( System organ class , preferred term) … table continued 100 . 0 44 Patients with any adverse event 9 . 1 4 Immune system disorders 15 . 9 7 Adverse events of special interest 9.1 4 Haemophagocytic lymphohistiocytosis 2 13.6 2.3 6 1 Cytokine release syndrome 1 Immune effector cell - associated neurotoxicity syndrome 9 . 1 4 4.5 2.3 2.3 2.3 6.8 4.5 2.3 2 1 1 1 3 2 1 Pneumonia Infection Sepsis 3 Systemic candida Gastrointestinal disorders Diarrhoea Abdominal pain 100.0 90.9 56.8 56.8 34.1 25.0 4.5 20.5 11.4 11.4 4.5 2.3 2.3 2.3 13.6 4.5 2.3 2.3 2.3 2.3 2.3 11.4 44 40 25 25 15 11 2 9 5 5 2 1 1 1 6 2 1 1 1 1 1 5 Blood and lymphatic system disorders Neutropenia Anaemia Lymphopenia Thrombocytopenia Leukopenia Febrile neutropenia Investigations Alanine aminotransferase increased Aspartate aminotransferase increased Blood creatinine increased Blood alkaline phosphatase increased Blood bilirubin increased Gamma - glutamyltransferase increased Metabolism and nutrition disorders Hypophosphataemia Acidosis Decreased appetite Hyperglycaemia Hype r magnesaemia Hypoalbuminaemia General disorders and administration site conditions 6 . 8 3 Skin and subcutaneous tissue disorders 4.5 2.3 2.3 2 1 1 Rash Alopecia Rash maculo - papular 6 . 8 3 Vascular disorders 6.8 3 Hypertension 4 . 5 2 Nervous system disorders 2.3 2.3 1 1 Neurotoxicity 2 Syncope 4 . 5 2 Renal and urinary disorders 2.3 2.3 1 1 Acute kidney injury Urinary tract obstruction 2 . 3 1 Hepatobiliary disorders 2.3 1 Hepatic function abnormal 2 . 3 1 Reproductive system and breast disorders 2.3 1 Oedema peripheral 2.3 1 Pelvic pain All treatment - emergent adverse events (TEAEs) with ≥ Grade 3 regardless of relatedness to study treatment that occurred in at least 1 patient are presented; 1 DLT: Dose limiting toxicity in patient DL4b - 04. 2 DLTs in patient DL4b - 01; CRS: cytokine release syndrome, HLH: hematophagocytic lymphohistiocytosis • Overall manageable tolerability profile • Expected cytopenias • Mostly mild to moderate CRS: 36% (16/44) Grade 1 48% (21/44) Grade 2 11% (5/44) Grade 3 2% (1/44) Grade 4 • DLTs in 2 patients at DL4b as previously reported by the Company: Patient DL4b - 01: high in vivo T cell expansion, Grade 4 neurotoxicity, Grade 4 CRS, Grade 3 HLH Patient DL4b - 04: Grade 3 CRS defined by Grade 3 ALT resolved to Grade 2 within 10 days; no need for vasopressors or ventilation 3 • No IMA203CD8 - related patient death • Consecutive modification of inclusion/exclusion criteria + IL - 2 scheme • Dose escalation ongoing based upon manageable tolerability in patients at DL4a 3 Possibly related Grade 5 event as previously reported was determined by the PI to be unlikely related to IMA203CD8 after complete assessment. Patient died from sepsis that was aggravated by immunosuppression from Flu/Cy (possibly related), high grade HLH event, the toxicity management and the fast - progressive disease PRAME Wave #2: IMA203CD8 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024
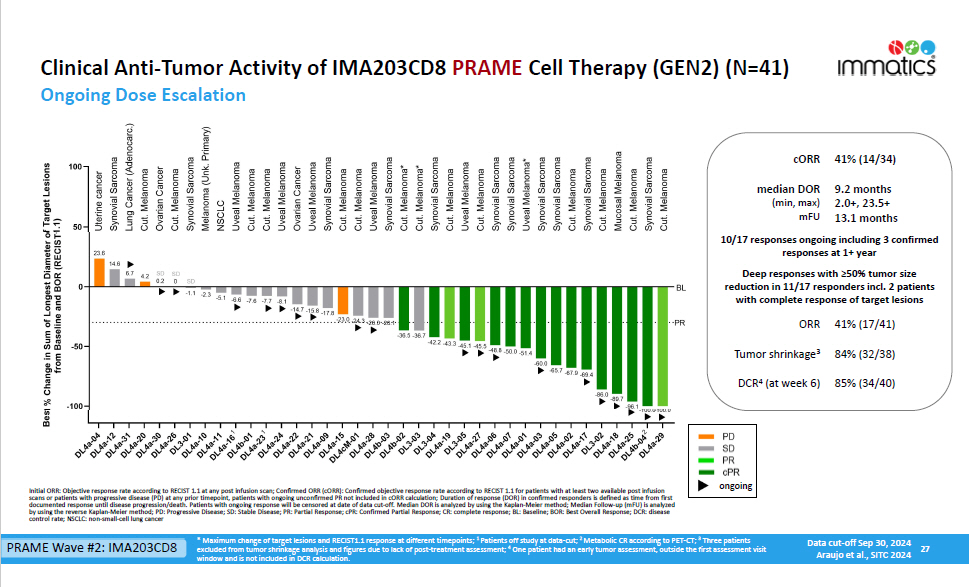
Clinical Anti - Tumor Activity of IMA203CD8 PRAME Cell Therapy (GEN2) (N=41) Ongoing Dose Escalation 27 41% (14/34) cORR 9.2 months 2.0+, 23.5+ 13.1 months median DOR (min, max) mFU 10/17 responses ongoing including 3 confirmed responses at 1+ year Deep responses with ≥50% tumor size reduction in 11/17 responders incl. 2 patients with complete response of target lesions 41% (17/41) ORR 84% (32/38) Tumor shrinkage 3 85% (34/40) DCR 4 (at week 6) ongoing * Maximum change of target lesions and RECIST1.1 response at different timepoints; 1 Patients off study at data - cut; 2 Metabolic CR according to PET - CT; 3 Three patients excluded from tumor shrinkage analysis and figures due to lack of post - treatment assessment; 4 One patient had an early tumor assessment, outside the first assessment visit window and is not included in DCR calculation. Initial ORR: Objective response rate according to RECIST 1.1 at any post infusion scan; Confirmed ORR (cORR): Confirmed objective response rate according to RECIST 1.1 for patients with at least two available post infusion scans or patients with progressive disease (PD) at any prior timepoint, patients with ongoing unconfirmed PR not included in cORR calculation; Duration of response (DOR) in confirmed responders is defined as time from first documented response until disease progression/death. Patients with ongoing response will be censored at date of data cut - off. Median DOR is analyzed by using the Kaplan - Meier method; Median Follow - up (mFU) is analyzed by using the reverse Kaplan - Meier method; PD: Progressive Disease; SD: Stable Disease; PR: Partial Response; cPR: Confirmed Partial Response; CR: complete response; BL: Baseline; BOR: Best Overall Response; DCR: disease control rate; NSCLC: non - small - cell lung cancer PRAME Wave #2: IMA203CD8 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024
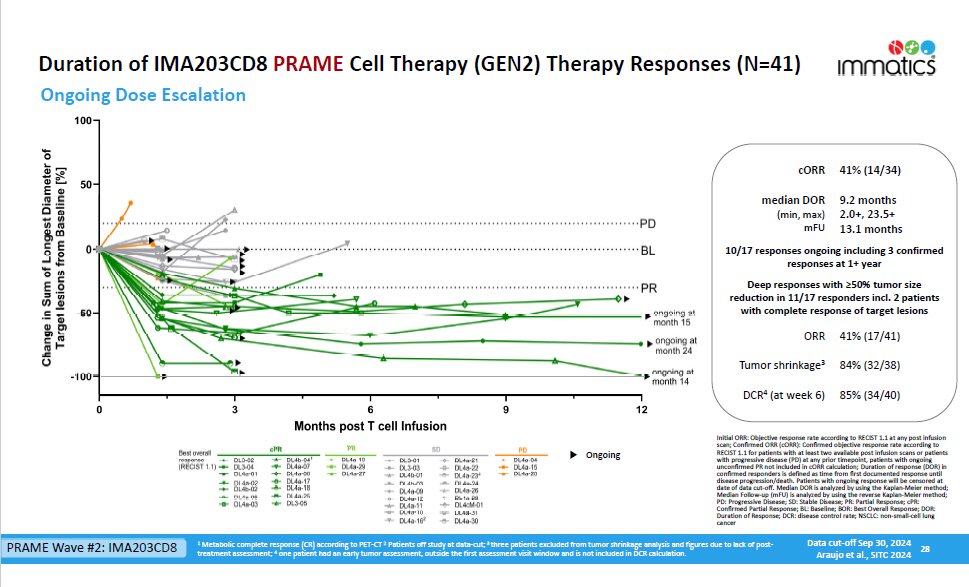
Duration of IMA203CD8 PRAME Cell Therapy (GEN2) Therapy Responses (N=41) Ongoing Dose Escalation 28 1 Metabolic complete response (CR) according to PET - CT 2 Patients off study at data - cut; 3 three patients excluded from tumor shrinkage analysis and figures due to lack of post - treatment assessment; 4 one patient had an early tumor assessment, outside the first assessment visit window and is not included in DCR calculation. 41% (14/34) cORR 9.2 months 2.0+, 23.5+ 13.1 months median DOR (min, max) mFU 10/17 responses ongoing including 3 confirmed responses at 1+ year Deep responses with ≥50% tumor size reduction in 11/17 responders incl. 2 patients with complete response of target lesions 41% (17/41) ORR 84% (32/38) Tumor shrinkage 3 85% (34/40) DCR 4 (at week 6) Initial ORR: Objective response rate according to RECIST 1.1 at any post infusion scan; Confirmed ORR (cORR): Confirmed objective response rate according to RECIST 1.1 for patients with at least two available post infusion scans or patients with progressive disease (PD) at any prior timepoint, patients with ongoing unconfirmed PR not included in cORR calculation; Duration of response (DOR) in confirmed responders is defined as time from first documented response until disease progression/death. Patients with ongoing response will be censored at date of data cut - off. Median DOR is analyzed by using the Kaplan - Meier method; Median Follow - up (mFU) is analyzed by using the reverse Kaplan - Meier method; PD: Progressive Disease; SD: Stable Disease; PR: Partial Response; cPR: Confirmed Partial Response; BL: Baseline; BOR: Best Overall Response; DOR: Duration of Response; DCR: disease control rate; NSCLC: non - small - cell lung cancer On go ing PRAME Wave #2: IMA203CD8 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024
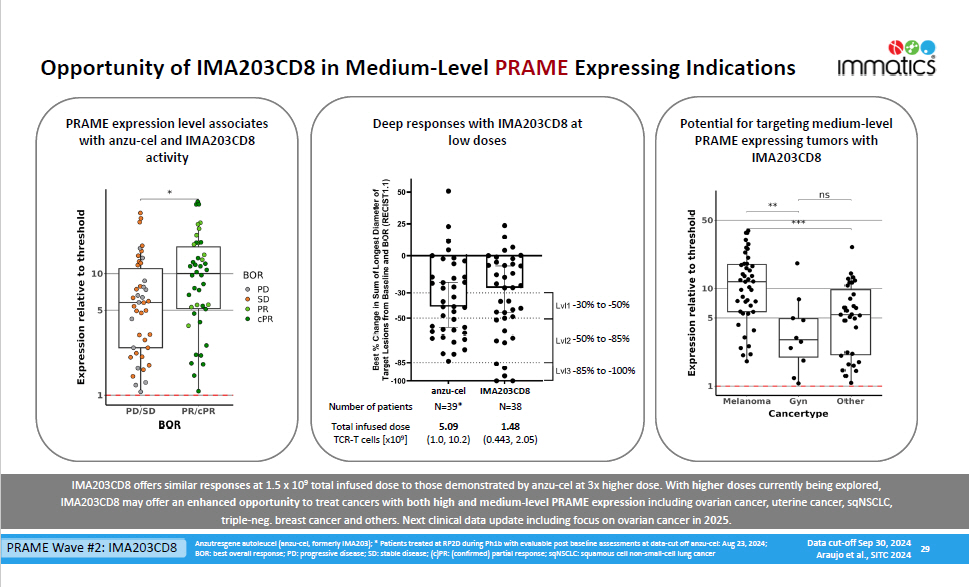
Opportunity of IMA203CD8 in Medium - Level PRAME Expressing Indications 29 Anzutresgene autoleucel (anzu - cel, formerly IMA203); * Patients treated at RP2D during Ph1b with evaluable post baseline assessments at data - cut off anzu - cel: Aug 23, 2024; BOR: best overall response; PD: progressive disease; SD: stable disease; (c)PR: (confirmed) partial response; sqNSCLC: squamous cell non - small - cell lung cancer N=38 N=39* Number of patients 1.48 (0.443, 2.05) 5.09 (1.0, 10.2) Total infused dose TCR - T cells [x10 9 ] Deep responses with IMA203CD8 at low doses - 30% to - 50% - 50% to - 85% - 85% to - 100% PRAME expression level associates with anzu - cel and IMA203CD8 activity Potential for targeting medium - level PRAME expressing tumors with IMA203CD8 IMA203CD8 offers similar responses at 1.5 x 10 9 total infused dose to those demonstrated by anzu - cel at 3x higher dose. With higher doses currently being explored, IMA203CD8 may offer an enhanced opportunity to treat cancers with both high and medium - level PRAME expression including ovarian cancer, uterine cancer, sqNSCLC, triple - neg. breast cancer and others. Next clinical data update including focus on ovarian cancer in 2025 . PRAME Wave #2: IMA203CD8 Data cut - off Sep 30, 2024 Araujo et al., SITC 2024 anzu - cel IMA203C D 8
IMA402 PRAME Bispecific Expansion to Early - Stage PRAME Cancers PRAME Wave #3
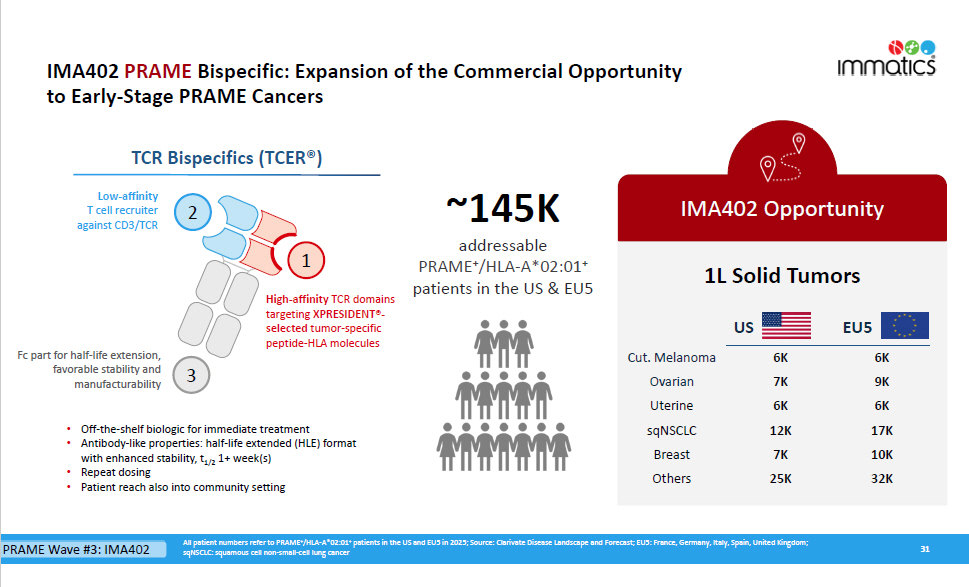
31 IMA402 Opportunity All patient numbers refer to PRAME + /HLA - A*02:01 + patients in the US and EU5 in 2025; Source: Clarivate Disease Landscape and Forecast; EU5: France, Germany, Italy, Spain, United Kingdom; sqNSCLC: squamous cell non - small - cell lung cancer ~145K addressable PRAM E + /HLA - A*02:0 1 + patients in the US & EU5 • Off - the - shelf biologic for immediate treatment • Antibody - like properties: half - life extended (HLE) format with enhanced stability, t 1/2 1+ week(s) • Repeat dosing • Patient reach also into community setting IMA402 PRAME Bispecific: Expansion of the Commercial Opportunity to Early - Stage PRAME Cancers TCR Bispecifics (TCER®) 2 1 3 Low - a ffinity T cell recruiter against CD3/TCR Fc part for half - life extension, favorable stability and manu f actu r ability High - affinity TCR domains targeting XPRESIDENT® - selected tumor - specific peptide - HLA molecules PRAME Wave #3: IMA402 1L Solid Tumors US EU5 6K 9K 6K 17K 10K 32K 6K 7K 6K 12K 7K 25K Cut. Melanoma Ovarian Uterine sqNSCLC B r ea s t Othe r s
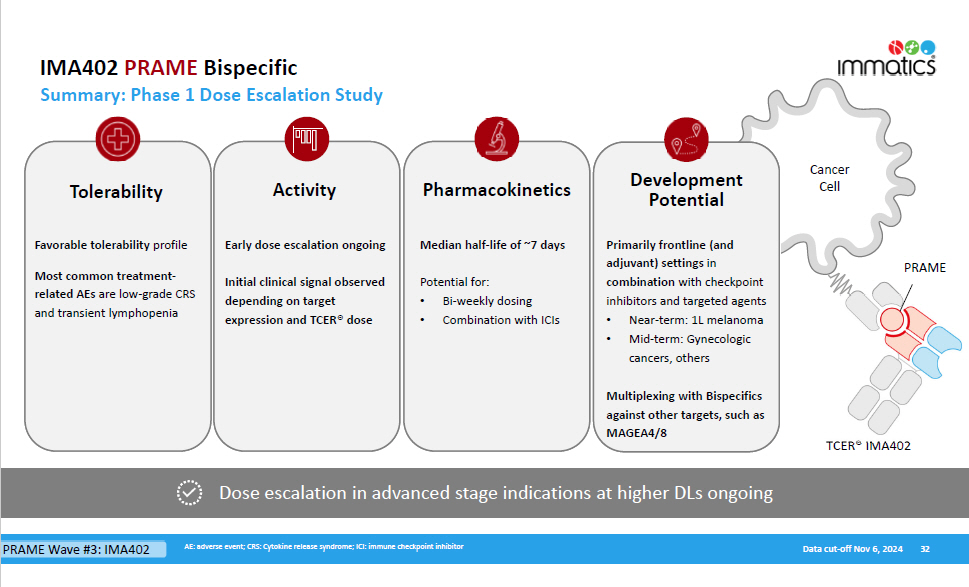
Cancer Cell IMA402 PRAME Bispecific Summary: Phase 1 Dose Escalation Study 32 Dose escalation in advanced stage indications at higher DLs ongoing Tolerability Favorable tolerability profile Most common treatment - related AEs are low - grade CRS and transient lymphopenia Early dose escalation ongoing Initial clinical signal observed depending on target expression and TCER® dose Pharmacokinetics Median half - life of ~7 days Potential for: • Bi - weekly dosing • Combination with ICIs Activity De v elopme n t Potential Primarily frontline (and adjuvant) settings in combination with checkpoint inhibitors and targeted agents • Near - term: 1L melanoma • Mid - term: Gynecologic AE: adverse event; CRS: Cytokine release syndrome; ICI: immune checkpoint inhibitor Data cut - off Nov 6, 2024 PRAME cancers, others Multiplexing with Bispecifics against other targets, such as MAGEA 4 / 8 TCER® IMA 402 PRAME Wave #3: IMA402
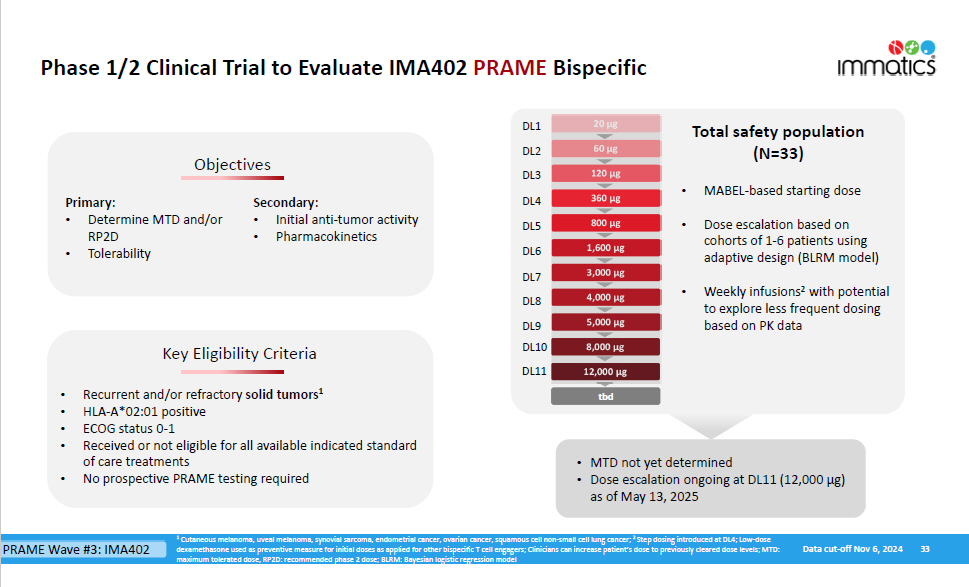
Phase 1/2 Clinical Trial to Evaluate IMA402 PRAME Bispecific 360 µg 800 µg 3,000 µg 5,000 µg 120 µg 1,600 µg 60 µg 20 µg D L 1 D L 2 D L 3 D L 4 D L 5 D L 7 D L 9 D L 6 8,000 µg 4,000 µg D L 8 Key Eligibility Criteria Objecti v es Primary: • Determine MTD and/or RP2D • Tolerability Secondary: • Initial anti - tumor activity • Pharmacokinetics • Recurrent and/or refractory solid tumors 1 • HLA - A*02:01 positive • ECOG status 0 - 1 • Received or not eligible for all available indicated standard of care treatments • No prospective PRAME testing required Total safety population (N=33) • MTD not yet determined • Dose escalation ongoing at DL11 (12,000 µg) as of May 13, 2025 33 1 Cutaneous melanoma, uveal melanoma, synovial sarcoma, endometrial cancer, ovarian cancer, squamous cell non - small cell lung cancer; 2 Step dosing introduced at DL4; Low - dose dexamethasone used as preventive measure for initial doses as applied for other bispecific T cell engagers; Clinicians can increase patient ’s dose to previously cleared dose levels; MTD: maximum tolerated dose, RP2D: recommended phase 2 dose; BLRM: Bayesian logistic regression model PRAME Wave #3: IMA402 Data cut - off Nov 6, 2024 • MABEL - based starting dose • Dose escalation based on cohorts of 1 - 6 patients using adaptive design (BLRM model) • Weekly infusions 2 with potential to explore less frequent dosing based on PK data D L 10 12,000 µg 20 µg 60 µg 120 µg 360 µg 800 µg 1,600 µg 3,000 µg 4,000 µg 5,000 µg 8,000 µg 12,000 µg D L 11 tbd tbd
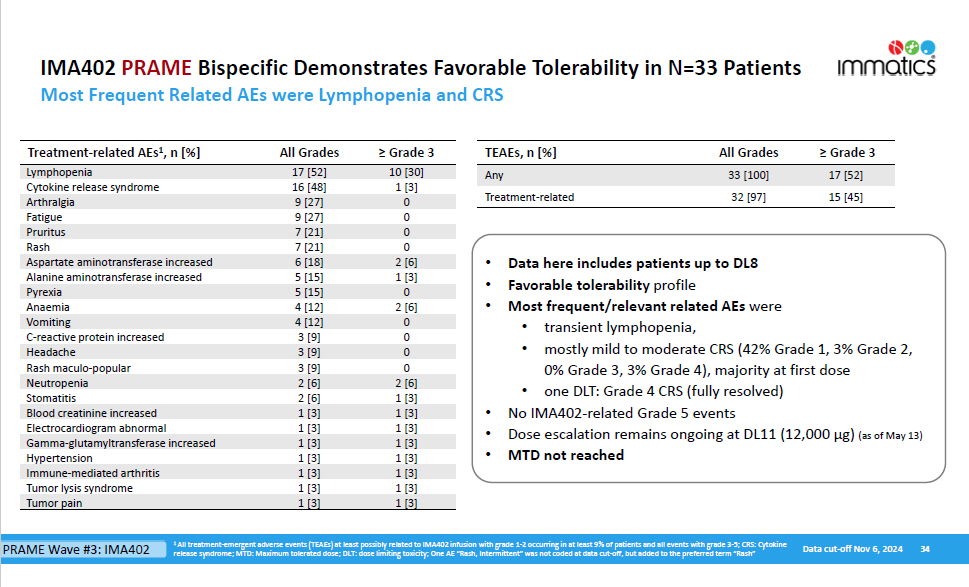
34 IMA402 PRAME Bispecific Demonstrates Favorable Tolerability in N=33 Patients Most Frequent Related AEs were Lymphopenia and CRS Grade 3 ≥ All Grades TEAEs, n [%] 17 [52] 33 [100] Any 15 [45] 32 [97] Treatment - related Grade 3 ≥ All Grades Treatment - related AEs 1 , n [%] 10 [30] 17 [52] Lymphopenia 1 [3] 16 [48] Cytokine release syndrome 0 9 [27] Arthralgia 0 9 [27] Fatigue 0 7 [21] Pruritus 0 7 [21] Rash 2 [6] 6 [18] Aspartate aminotransferase increased 1 [3] 5 [15] Alanine aminotransferase increased 0 5 [15] Pyrexia 2 [6] 4 [12] Anaemia 0 4 [12] Vomiting 0 3 [9] C - reactive protein increased 0 3 [9] Headache 0 3 [9] Rash maculo - popular 2 [6] 2 [6] Neutropenia 1 [3] 2 [6] Stomatitis 1 [3] 1 [3] Blood creatinine increased 1 [3] 1 [3] Electrocardiogram abnormal 1 [3] 1 [3] Gamma - glutamyltransferase increased 1 [3] 1 [3] Hypertension 1 [3] 1 [3] Immune - mediated arthritis 1 [3] 1 [3] Tumor lysis syndrome 1 [3] 1 [3] Tumor pain • Data here includes patients up to DL8 • Favorable tolerability profile • Most frequent/relevant related AEs were • transient lymphopenia, • mostly mild to moderate CRS (42% Grade 1, 3% Grade 2, 0% Grade 3, 3% Grade 4), majority at first dose • one DLT: Grade 4 CRS (fully resolved) • No IMA402 - related Grade 5 events • Dose escalation remains ongoing at DL11 (12,000 µg) (as of May 13) • MTD not reached 1 All treatment - emergent adverse events (TEAEs) at least possibly related to IMA402 infusion with grade 1 - 2 occurring in at least 9% of patients and all events with grade 3 - 5; CRS: Cytokine release syndrome; MTD: Maximum tolerated dose; DLT: dose limiting toxicity; One AE “Rash, Intermittent” was not coded at data cut - off, but added to the preferred term “Rash” Data cut - off Nov 6, 2024 PRAME Wave #3: IMA402
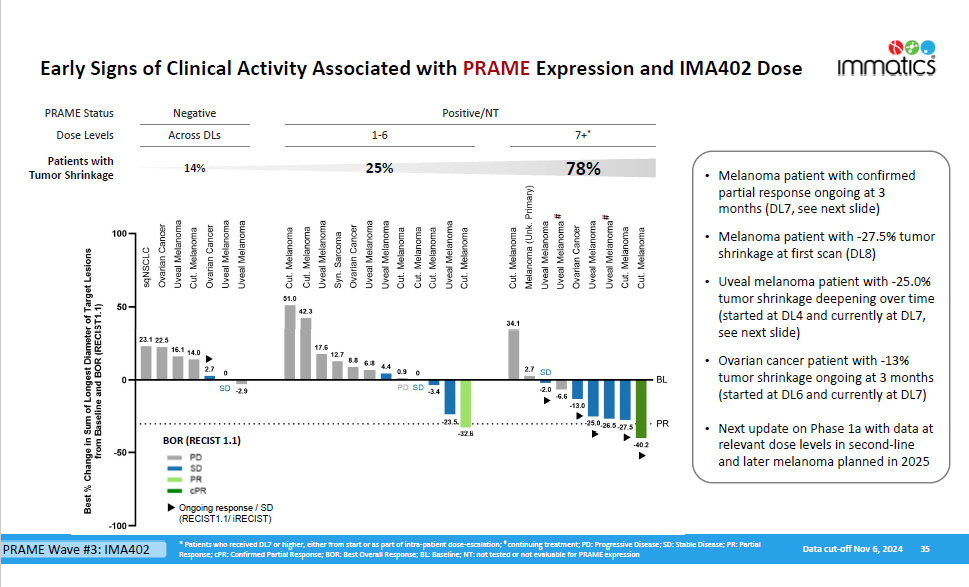
Positive/NT Ne g a ti v e 7+ * 1 - 6 Across DLs PRAME Status Dose Levels 78% 25% 14% Patients with Tumor Shrinkage Early Signs of Clinical Activity Associated with PRAME Expression and IMA402 Dose 35 BOR (RECIST 1.1) Ongoing response / SD (RECIST1.1/ iRECIST) Data cut - off Nov 6, 2024 * Patients who received DL7 or higher, either from start or as part of intra - patient dose - escalation; # continuing treatment; PD: Progressive Disease; SD: Stable Disease; PR: Partial Response; cPR: Confirmed Partial Response; BOR: Best Overall Response; BL: Baseline; NT: not tested or not evaluable for PRAME expression # # • Melanoma patient with confirmed partial response ongoing at 3 months (DL7, see next slide) • Melanoma patient with - 27.5% tumor shrinkage at first scan (DL8) • Uveal melanoma patient with - 25.0% tumor shrinkage deepening over time (started at DL4 and currently at DL7, see next slide) • Ovarian cancer patient with - 13% tumor shrinkage ongoing at 3 months (started at DL6 and currently at DL7) • Next update on Phase 1a with data at relevant dose levels in second - line and later melanoma planned in 2025 PRAME Wave #3: IMA402
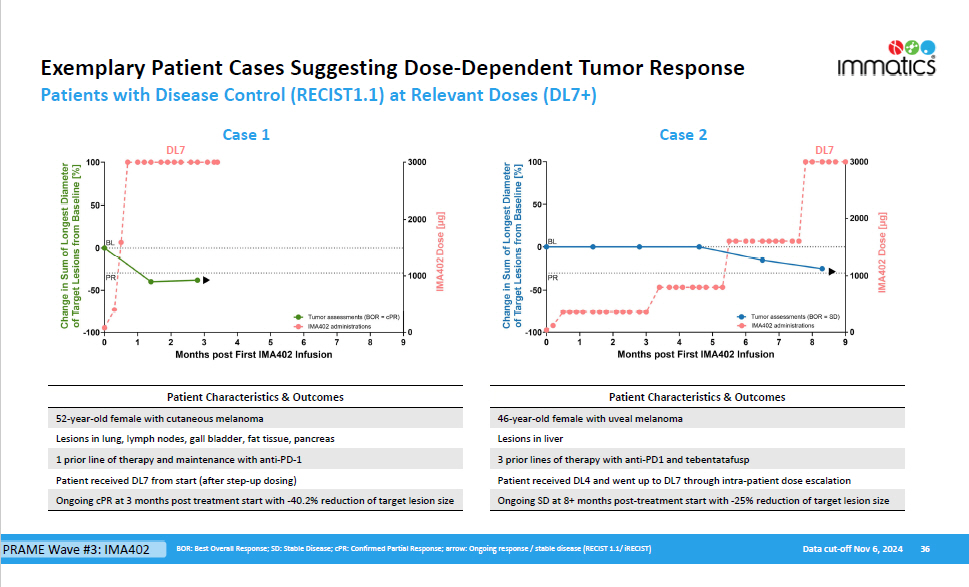
Exemplary Patient Cases Suggesting Dose - Dependent Tumor Response 36 Data cut - off Nov 6, 2024 BOR: Best Overall Response; SD: Stable Disease; cPR: Confirmed Partial Response; arrow: Ongoing response / stable disease (RECIST 1.1/ iRECIST) Patients with Disease Control (RECIST1.1) at Relevant Doses (DL7+) Case 1 Case 2 DL7 DL7 Patient Characteristics & Outcomes 52 - year - old female with cutaneous melanoma Lesions in lung, lymph nodes, gall bladder, fat tissue, pancreas 1 prior line of therapy and maintenance with anti - PD - 1 Patient received DL7 from start (after step - up dosing) Ongoing cPR at 3 months post treatment start with - 40.2% reduction of target lesion size Patient Characteristics & Outcomes 46 - year - old female with uveal melanoma Lesions in liver 3 prior lines of therapy with anti - PD1 and tebentatafusp Patient received DL4 and went up to DL7 through intra - patient dose escalation Ongoing SD at 8+ months post - treatment start with - 25% reduction of target lesion size PRAME Wave #3: IMA402

IMA401 MAGEA4/8 Bispecific Driving Innovation beyond PRAME beyond PRAME
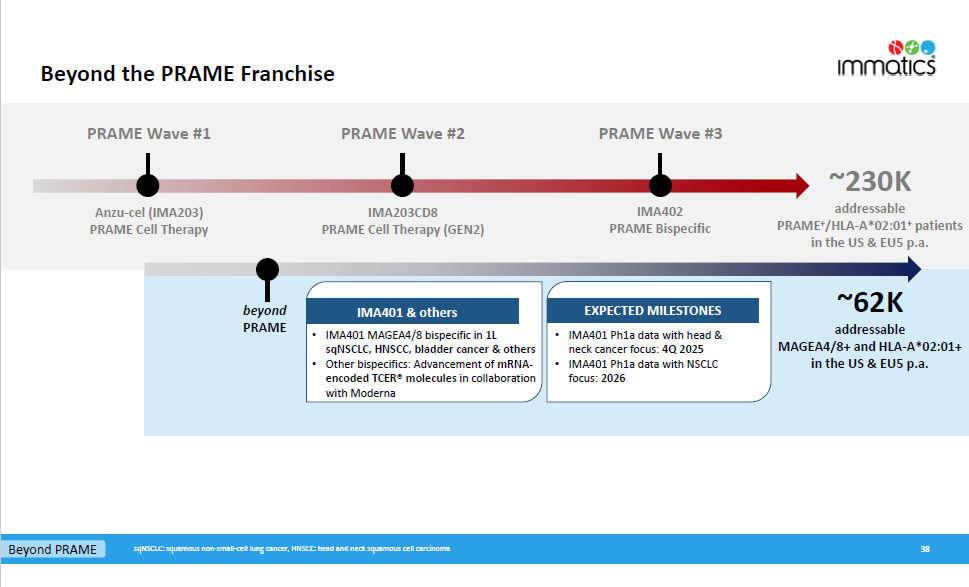
Beyond the PRAME Franchise PRAME Wave #1 PRAME Wave #2 PRAME Wave #3 ~230K addressable PRAME + /HLA - A*02:01 + patients in the US & EU5 p.a. Anzu - cel (IMA203) PRAME Cell Therapy IMA203CD8 PRAME Cell Therapy (GEN2) IMA402 PRAME Bispecific ~62K addressable MAGEA4/8+ and HLA - A*02:01+ in the US & EU5 p.a. b e yond PRAME 38 EXPECTED MILESTONES • IMA401 Ph1a data with head & neck cancer focus: 4Q 2025 • IMA401 Ph1a data with NSCLC focus: 2026 IMA401 & others • IMA 401 MAGEA 4 / 8 bispecific in 1 L sqNSCLC, HNSCC, bladder cancer & others • Other bispecifics : Advancement of mRNA - encoded TCER® molecules in collaboration with Moderna Beyond PRAME sqNSCLC: squamous non - small - cell lung cancer, HNSCC: head and neck squamous cell carcinoma
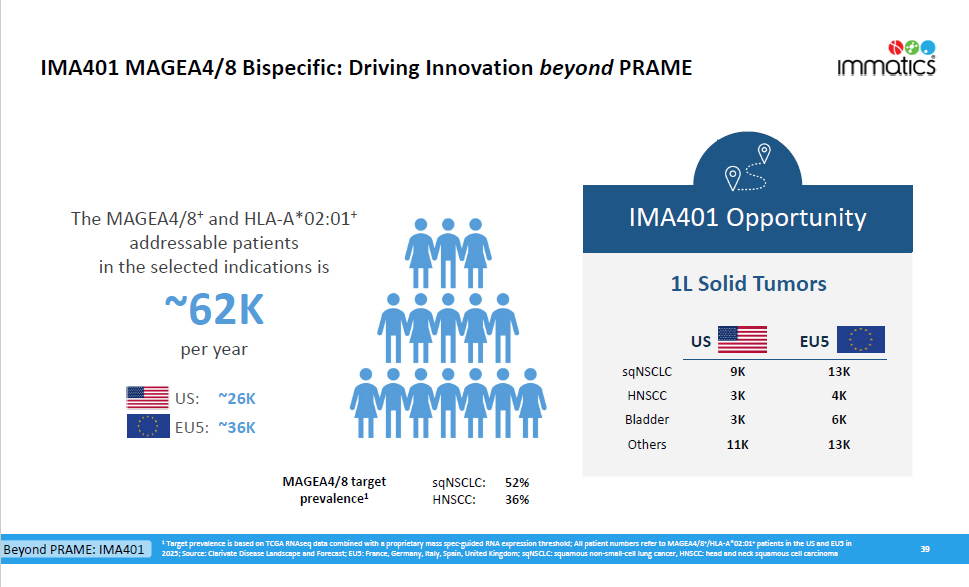
IMA401 MAGEA4/8 Bispecific: Driving Innovation beyond PRAME 39 IMA401 Opportunity 1 Target prevalence is based on TCGA RNAseq data combined with a proprietary mass spec - guided RNA expression threshold; All patient numbers refer to MAGEA4/8 + /HLA - A*02:01 + patients in the US and EU5 in 2025; Source: Clarivate Disease Landscape and Forecast; EU5: France, Germany, Italy, Spain, United Kingdom; sqNSCLC: squamous non - small - cell lung cancer, HNSCC: head and neck squamous cell carcinoma The MAGEA4/8 + and HLA - A*02:01 + addressable patients in the selected indications is ~62K per year ~26K US: ~36K EU5: Beyond PRAME: IMA401 1L Solid Tumors US EU5 13K 4K 6K 13K 9K 3K 3K 11K sqNSC L C HNSCC Bladder Others MAGEA4/8 target prevalence 1 sqNSC L C: 52% HNSCC: 36%
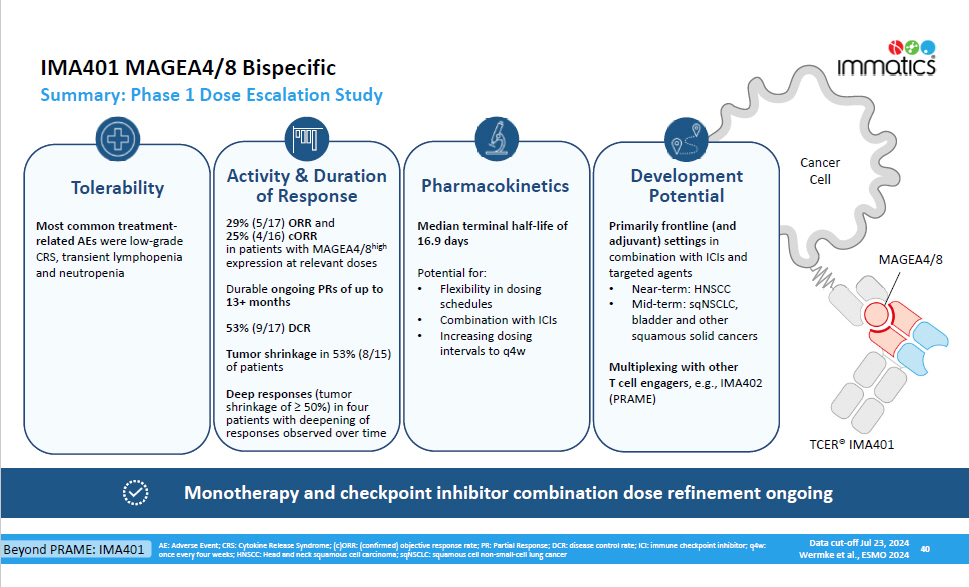
Cancer Cell MAG E A4/8 IMA401 MAGEA4/8 Bispecific Summary: Phase 1 Dose Escalation Study 40 AE: Adverse Event; CRS: Cytokine Release Syndrome; (c)ORR: (confirmed) objective response rate; PR: Partial Response; DCR: disease control rate; ICI: immune checkpoint inhibitor; q4w: once every four weeks; HNSCC: Head and neck squamous cell carcinoma; sqNSCLC: squamous cell non - small - cell lung cancer Data cut - off Jul 23, 2024 Wermke et al., ESMO 2024 Durable ongoing PRs of up to 13+ months 53% (9/17) DCR Tumor shrinkage in 53% (8/15) of patients Deep responses (tumor shrinkage of ≥ 50%) in four patients with deepening of responses observed over time Tolerability Activity & Duration of Response 29% (5/17) ORR and 25% (4/16) cORR in patients with MAGEA4/8 high expression at relevant doses • Near - term: HNSCC • Mid - term: sqNSCLC, bladder and other squamous solid cancers Multiplexing with other T cell engagers , e.g., IMA402 (PRAME) De v elopme n t Potential Primarily frontline (and adjuvant) settings in combination with ICIs and targeted agents Most common treatment - related AEs were low - grade CRS, transient lymphopenia and neutropenia Pharmacokinetics Median terminal half - life of 16.9 days Potential for: • Flexibility in dosing schedules • Combination with ICIs • Increasing dosing intervals to q4w Monotherapy and checkpoint inhibitor combination dose refinement ongoing TCER® IMA401 Beyond PRAME: IMA401
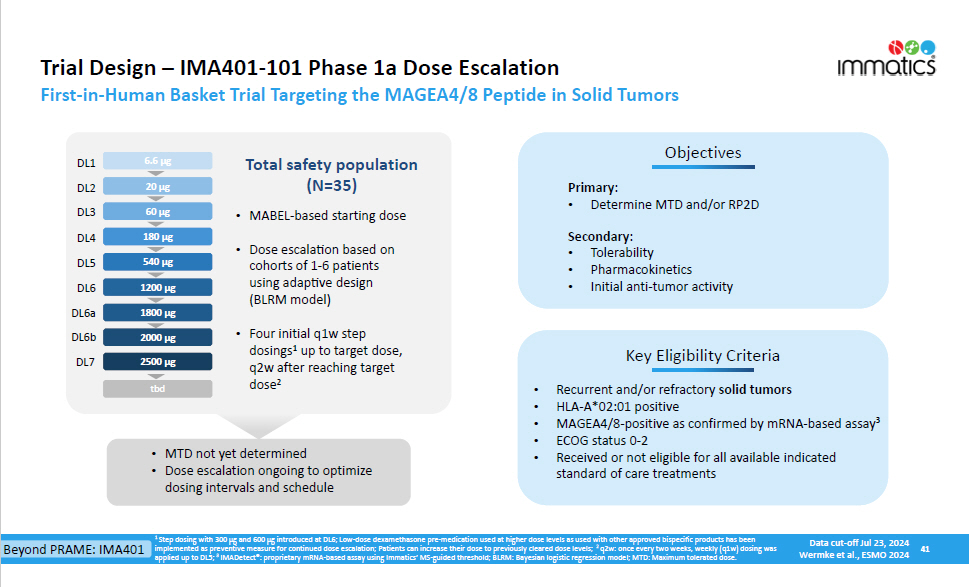
41 180 µg 540 µg 1800 µg 1800 µg 2500 µg 2500 µg Key Eligibility Criteria Objecti v es Primary: • Determine MTD and/or RP2D Secondary: • Tolerability • Pharmacokinetics • Initial anti - tumor activity • Recurrent and/or refractory solid tumors • HLA - A*02:01 positive • MAGEA4/8 - positive as confirmed by mRNA - based assay 3 • ECOG status 0 - 2 • Received or not eligible for all available indicated standard of care treatments 60 µg 1200 µg 20 µg 6.6 µg 6.6 µg 20 µg 60 µg 180 µg 540 µg • MTD not yet determined • Dose escalation ongoing to optimize dosing intervals and schedule Total safety population (N=35) • MABEL - based starting dose • Dose escalation based on cohorts of 1 - 6 patients using adaptive design (BLRM model) • Four initial q1w step dosings 1 up to target dose, q2w after reaching target dose 2 Trial Design – IMA401 - 101 Phase 1a Dose Escalation First - in - Human Basket Trial Targeting the MAGEA4/8 Peptide in Solid Tumors 1 Step dosing with 300 µg and 600 µg introduced at DL6; Low - dose dexamethasone pre - medication used at higher dose levels as used with other approved bispecific products has been implemented as preventive measure for continued dose escalation; Patients can increase their dose to previously cleared dose levels; 2 q2w: once every two weeks, weekly (q1w) dosing was applied up to DL5; 3 IMADetect®: proprietary mRNA - based assay using Immatics’ MS - guided threshold; BLRM: Bayesian logistic regression model; MTD: Maximum tolerated dose. D L 1 D L 2 D L 3 D L 4 D L 5 D L 6a D L 7 D L 6 tb d tbd 2000 µg 2000 µg D L 6b Beyond PRAME: IMA401 Data cut - off Jul 23, 2024 Wermke et al., ESMO 2024
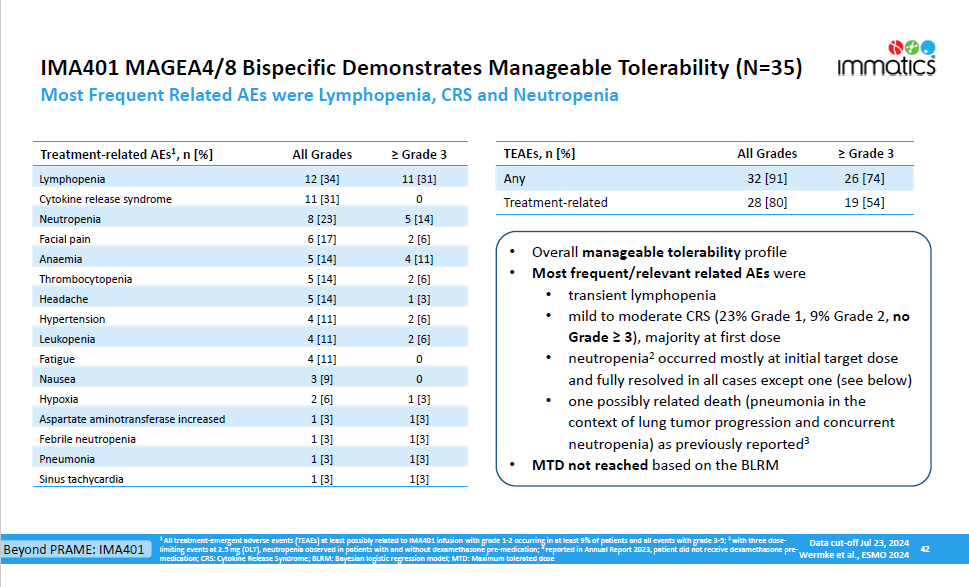
42 IMA401 MAGEA4/8 Bispecific Demonstrates Manageable Tolerability (N=35) Most Frequent Related AEs were Lymphopenia, CRS and Neutropenia ≥ Grade 3 All Grades TEAEs, n [%] 26 [74] 19 [54] 32 [91] 28 [80] Any Treatment - related ≥ Grade 3 All Grades Treatment - related AEs 1 , n [%] 11 [31] 0 5 [14] 2 [6] 4 [11] 2 [6] 1 [3] 2 [6] 2 [6] 0 0 1 [3] 1[3] 1[3] 1[3] 12 [34] 11 [31] 8 [23] 6 [17] 5 [14] 5 [14] 5 [14] 4 [11] 4 [11] 4 [11] 3 [9] 2 [6] 1 [3] 1 [3] 1 [3] Lymphopenia Cytokine release syndrome Neutropenia Facial pain Anaemia Th r o mbocy t openia Headache Hypertension Leukopenia Fatigue Nausea Hyp o xia Aspartate aminotransferase increased Febrile neutropenia Pneumonia Sinus tachycardia 1 [3] 1[3] • Overall manageable tolerability profile • Most frequent/relevant related AEs were • transient lymphopenia • mild to moderate CRS (23% Grade 1, 9% Grade 2, no Grade ≥ 3 ), majority at first dose • neutropenia 2 occurred mostly at initial target dose and fully resolved in all cases except one (see below) • one possibly related death (pneumonia in the context of lung tumor progression and concurrent neutropenia) as previously reported 3 • MTD not reached based on the BLRM 1 All treatment - emergent adverse events (TEAEs) at least possibly related to IMA401 infusion with grade 1 - 2 occurring in at least 9% of patients and all events with grade 3 - 5; 2 with three dose - limiting events at 2.5 mg (DLT), neutropenia observed in patients with and without dexamethasone pre - medication; 3 reported in Annual Report 2023, patient did not receive dexamethasone pre - medication; CRS: Cytokine Release Syndrome; BLRM: Bayesian logistic regression model; MTD: Maximum tolerated dose Beyond PRAME: IMA401 Data cut - off Jul 23, 2024 Wermke et al., ESMO 2024
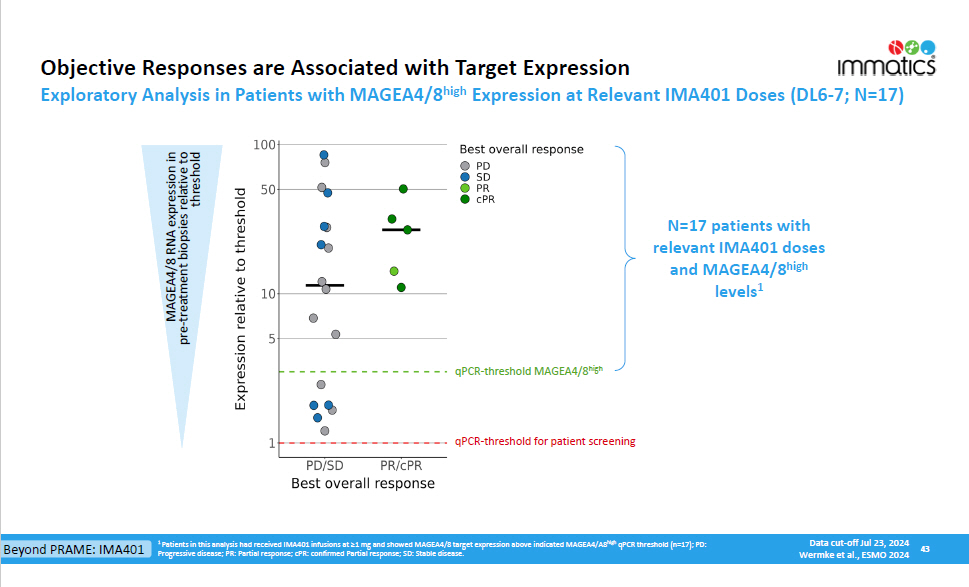
1 Patients in this analysis had received IMA401 infusions at ≥1 mg and showed MAGEA4/8 target expression above indicated MAGEA4/A8 high qPCR threshold (n=17); PD: Progressive disease; PR: Partial response; cPR: confirmed Partial response; SD: Stable disease. Objective Responses are Associated with Target Expression Exploratory Analysis in Patients with MAGEA4/8 high Expression at Relevant IMA401 Doses (DL6 - 7; N=17) 43 qPCR - threshold MAGEA4/8 high qPCR - threshold for patient screening MAGEA4/8 RNA expression in pre - treatment biopsies relative to th r e shold N=17 patients with relevant IMA401 doses and MAGEA4/8 high levels 1 Beyond PRAME: IMA401 Data cut - off Jul 23, 2024 Wermke et al., ESMO 2024
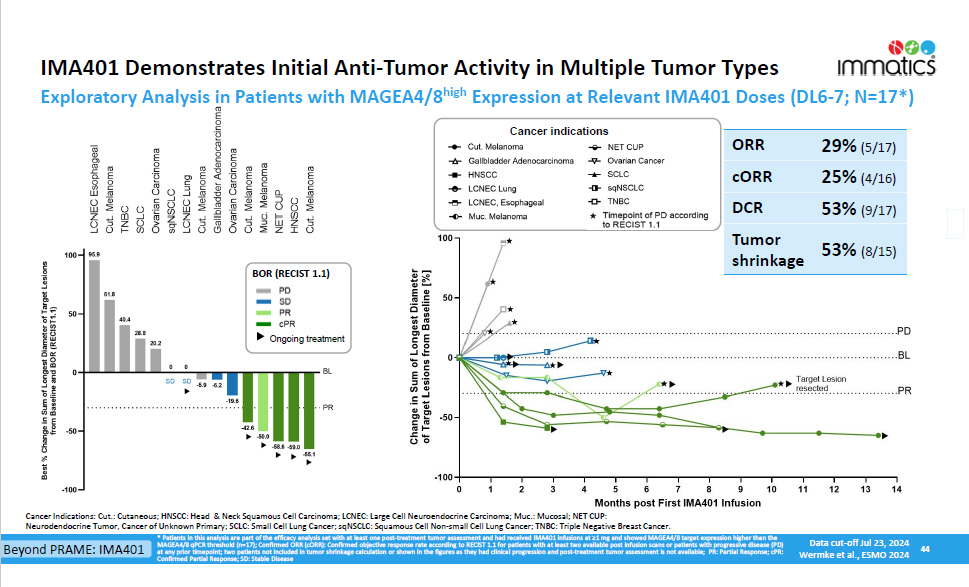
IMA401 Demonstrates Initial Anti - Tumor Activity in Multiple Tumor Types 44 * Patients in this analysis are part of the efficacy analysis set with at least one post - treatment tumor assessment and had received IMA401 infusions at ≥1 mg and showed MAGEA4/8 target expression higher than the MAGEA4/8 qPCR threshold (n=17); Confirmed ORR (cORR): Confirmed objective response rate according to RECIST 1.1 for patients with at least two available post infusion scans or patients with progressive disease (PD) at any prior timepoint; two patients not included in tumor shrinkage calculation or shown in the figures as they had clinical progression and post - treatment tumor assessment is not available; PR: Partial Response; cPR: Confirmed Partial Response; SD: Stable Disease Exploratory Analysis in Patients with MAGEA4/8 high Expression at Relevant IMA401 Doses (DL6 - 7; N=17*) ORR 29% (5/17) cORR 25% (4/16) DCR 53% (9/17) Tumor 53% (8/15) shrinkage Cancer Indications: Cut.: Cutaneous; HNSCC: Head & Neck Squamous Cell Carcinoma; LCNEC: Large Cell Neuroendocrine Carcinoma; Muc.: Mucosal; NET CUP: Neurodendocrine Tumor, Cancer of Unknown Primary; SCLC: Small Cell Lung Cancer; sqNSCLC: Squamous Cell Non - small Cell Lung Cancer; TNBC: Triple Negative Breast Cancer. BOR (RECIST 1.1) Ongoing treatment Cancer indications Beyond PRAME: IMA401 Data cut - off Jul 23, 2024 Wermke et al., ESMO 2024

Delivering © Immatics. Not for further reproduction or distribution. www.immatics.com the Power of T cells to Cancer Patients Appendix
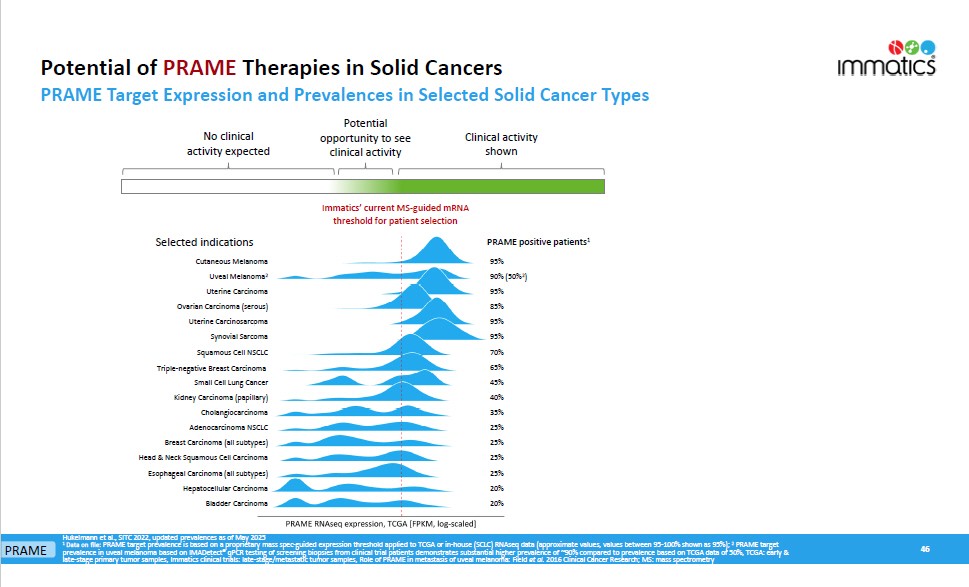
Potential of PRAME Therapies in Solid Cancers 46 Hukelmann et al., SITC 2022, updated prevalences as of May 2025 1 Data on file: PRAME target prevalence is based on a proprietary mass spec - guided expression threshold applied to TCGA or in - house (SCLC) RNAseq data (approximate values, values between 95 - 100% shown as 95%); 2 PRAME target prevalence in uveal melanoma based on IMADetect® qPCR testing of screening biopsies from clinical trial patients demonstrates substantial higher prevalence of ~90% compared to prevalence based on TCGA data of 50%, TCGA: early & late - stage primary tumor samples, Immatics clinical trials: late - stage/metastatic tumor samples, Role of PRAME in metastasis of uveal melanoma: Field et al. 2016 Clinical Cancer Research; MS: mass spectrometry Immatics’ current MS - guided mRNA threshold for patient selection Selected indications Clinical activity shown No clinical activity expected PRAME Target Expression and Prevalences in Selected Solid Cancer Types Potential opportunity to see clinical activity PRAME 95% Cutaneous Melanoma 90% (50% 2 ) Uveal Melanoma 2 95% Uterine Carcinoma 85% Ovarian Carcinoma (serous) 95% Uterine Carcinosarcoma 95% Synovial Sarcoma 70% Squamous Cell NSCLC 65% Triple - negative Breast Carcinoma 45% Small Cell Lung Cancer 40% Kidney Carcinoma (papillary) 35% Cholangiocarcinoma 25% Adenocarcinoma NSCLC 25% Breast Carcinoma (all subtypes) 25% Head & Neck Squamous Cell Carcinoma 25% Esophageal Carcinoma (all subtypes) 20% Hepatocellular Carcinoma 20% Bladder Carcinoma PRAME positive patients 1
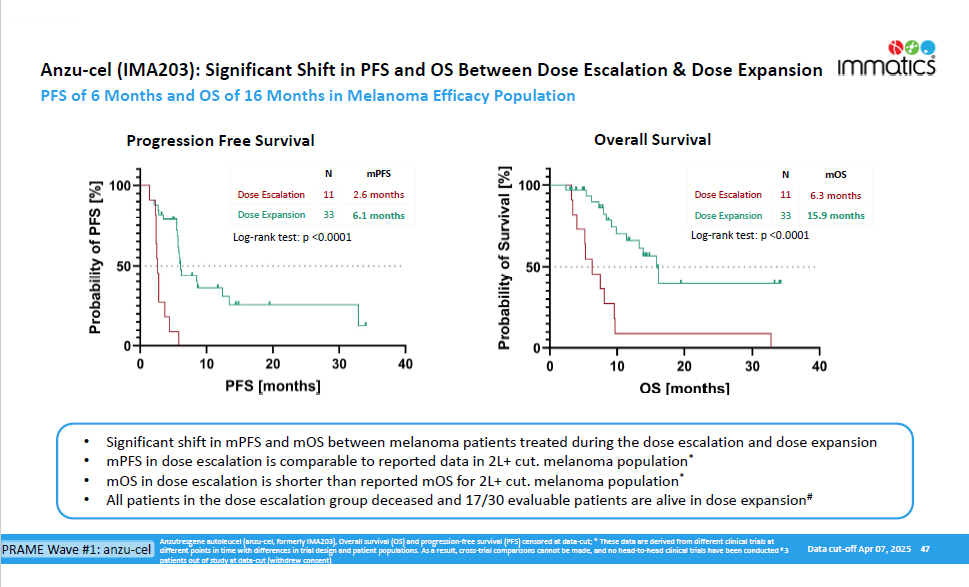
Data cut - off Apr 07, 2025 47 Anzu - cel (IMA203): Significant Shift in PFS and OS Between Dose Escalation & Dose Expansion PFS of 6 Months and OS of 16 Months in Melanoma Efficacy Population Progression Free Survival Overall Survival N mPFS 2.6 months 11 Dose Escalation 6.1 months 33 Dose Expansion N mOS 6.3 months 11 Dose Escalation 15.9 months 33 Dose Expansion • Significant shift in mPFS and mOS between melanoma patients treated during the dose escalation and dose expansion • mPFS in dose escalation is comparable to reported data in 2L+ cut. melanoma population * • mOS in dose escalation is shorter than reported mOS for 2L+ cut. melanoma population * • All patients in the dose escalation group deceased and 17/30 evaluable patients are alive in dose expansion # Log - rank test: p <0.0001 Log - rank test: p <0.0001 Anzutresgene autoleucel (anzu - cel, formerly IMA203), Overall survival (OS) and progression - free survival (PFS) censored at data - cut; * These data are derived from different clinical trials at PRAME Wave #1: anzu - cel different points in time with differences in trial design and patient populations. As a result, cross - trial comparisons cannot be made, and no head - to - head clinical trials have been conducted # 3 patients out of study at data - cut (withdrew consent)