.2
© Immatics. Not for further reproduction or distribution. IMA203CD8 Cell Therapy in PRAME - positive Solid Tumors - Phase 1a Dose Escalation Clinical Data Update December 11, 2025
Disclaimer This presentation (“Presentation”) is provided by Immatics N . V . (“Immatics” or the “Company”) for informational purposes only . The information contained herein does not purport to be all inclusive and none of Immatics, any of its affiliates, any of its or their respective control persons, officers, directors, employees or representatives makes any representation or warranty, express or implied, as to the accuracy, completeness or reliability of the information contained in this Presentation . Forward - Looking Statements . Certain statements in this presentation may be considered forward - looking statements . Forward - looking statements generally relate to future events or the Company’s future financial or operating performance . For example, statements concerning timing of data read - outs for product candidates, observations from the Company’s clinical trials, the timing, outcome and design of clinical trials, the nature of clinical trials (including whether such clinical trials will be registration - enabling), the timing of IND, CTA or BLA filings, estimated market opportunities of product candidates, the Company’s focus on partnerships to advance its strategy, and other metrics are forward - looking statements . In some cases, you can identify forward - looking statements by terminology such as “may”, “should”, “expect”, “plan”, “target”, “intend”, “will”, “estimate”, “anticipate”, “believe”, “predict”, “potential” or “continue”, or the negatives of these terms or variations of them or similar terminology . Such forward - looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ materially from those expressed or implied by such forward looking statements . These forward - looking statements are based upon estimates and assumptions that, while considered reasonable by Immatics and its management, are inherently uncertain . New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties . Factors that may cause actual results to differ materially from current expectations include, but are not limited to, various factors beyond management's control including general economic conditions and other risks, uncertainties and factors set forth in the Company’s Annual Report on Form 20 - F and other filings with the Securities and Exchange Commission (SEC) . Nothing in this presentation should be regarded as a representation by any person that the forward - looking statements set forth herein will be achieved or that any of the contemplated results of such forward - looking statements will be achieved . You should not place undue reliance on forward - looking statements, which speak only as of the date they are made . The Company undertakes no duty to update these forward - looking statements . No Offer or Solicitation . This communication is for informational purposes only and does not constitute, or form a part of, an offer to sell or the solicitation of an offer to sell or an offer to buy or the solicitation of an offer to buy any securities, and there shall be no sale of securities, in any jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such jurisdiction . No offer of securities shall be made except by means of a prospectus meeting the requirements of Section 10 of the Securities Act of 1933 , as amended, or in an offering exempt from registration . Certain information contained in this Presentation relates to or is based on studies, publications, surveys and the Company’s own internal estimates and research . In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions . Finally, while the Company believes its internal research is reliable, such research has not been verified by any independent source . All the scientific and clinical data presented within this presentation are – by definition prior to completion of the clinical trial and a clinical study report – preliminary in nature and subject to further quality checks including customary source data verification . 2
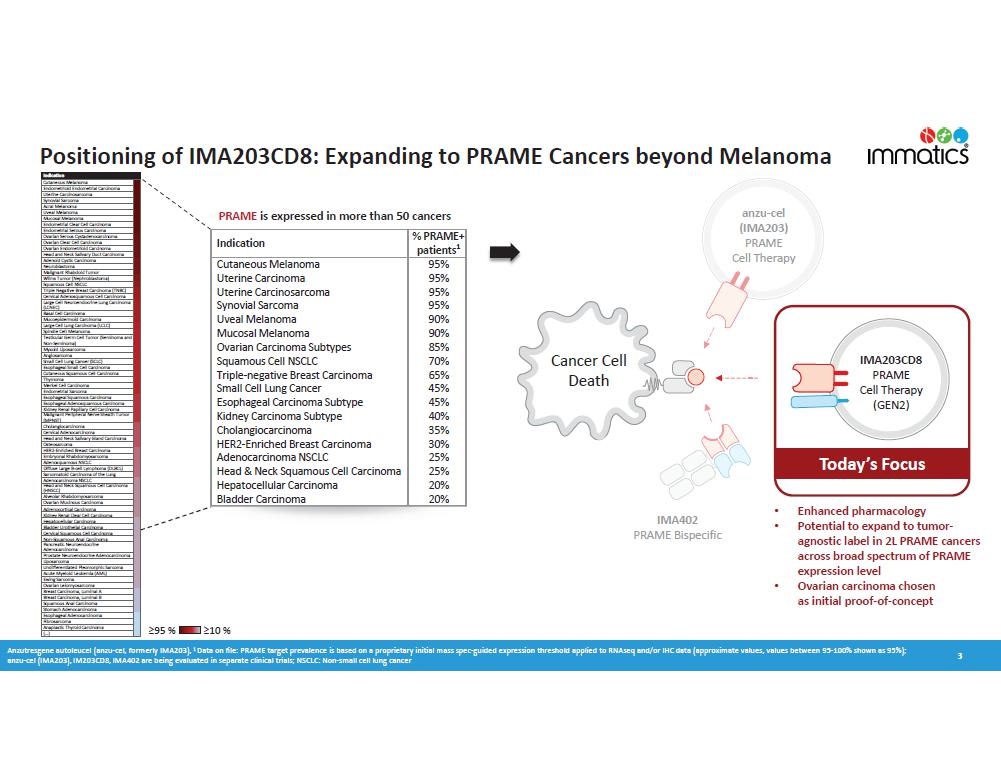
nzu c el (I M A203) P R AME Cell Therapy 295 % 210 % Anzutresgene autoleucel (anzu - cel, formerly IMA203), 1 Data on file: PRAME target prevalence is based on a proprietary initial mass spec - guided expression threshold applied to RNAseq and/or IHC data (approximate values, values between 95 - 100% shown as 95%); anzu - cel (IMA203), IM203CD8, IMA402 are being evaluated in separate clinical trials; NSCLC: Non - small cell lung cancer Cancer Cell Death I M A402 PRAME Bispecific PRAME is expressed in more than 50 cancers % PRAME+ patients 1 Indication 95% Cutaneous Melanoma 95% Uterine Carcinoma 95% Uterine Carcinosarcoma 95% Synovial Sarcoma 90% Uveal Melanoma 90% Mucosal Melanoma 85% Ovarian Carcinoma Subtypes 70% Squamous Cell NSCLC 65% Triple - negative Breast Carcinoma 45% Small Cell Lung Cancer 45% Esophageal Carcinoma Subtype 40% Kidney Carcinoma Subtype 35% Cholangiocarcinoma 30% HER2 - Enriched Breast Carcinoma 25% Adenocarcinoma NSCLC 25% Head & Neck Squamous Cell Carcinoma 20% Hepatocellular Carcinoma 20% Bladder Carcinoma 3 Cutaneous Melanoma Endometrioid Endometrial Carcinoma Uterine Carcinosarcoma Synovial Sarcoma Acral Melanoma Uveal Melanoma Mucosal Melanoma Endometrial Clear Cell Carcinoma Endometrial Serous Carcinoma Ovarian Serous Cystadenocarcinoma Ovarian Clear Cell Carcinoma Ovarian Endometrioid Carcinoma Head and Neck Salivary Duct Carcinoma Adenoid Cystic Carcinoma Neuroblastoma Malignant Rhabdoid Tumor Wilms Tumor (Nephroblastoma) Squamous Cell NSCLC Triple Negative Breast Carcinoma (TNBC) Cervical Adenosquamous Cell Carcinoma Large Cell Neuroendocrine Lung Carcinoma (LCNEC) Basal Cell Carcinoma Mucoepidermoid Carcinoma Large Cell Lung Carcinoma (LCLC) Spindle Cell Melanoma Testicular Germ Cell Tumor (Seminoma and Non - Seminoma) Myxoid Liposarcoma Angiosarcoma Small Cell Lung Cancer (SCLC) Esophageal Small Cell Carcinoma Cutaneous Squamous Cell Carcinoma Thymoma Merkel Cell Carcinoma Endometrial Sarcoma Esophageal Squamous Carcinoma Esophageal Adenosquamous Carcinoma Kidney Renal Papillary Cell Carcinoma Malignant Peripheral Nerve Sheath Tumor (MPNST) Cholangiocarcinoma Cervical Adenocarcinoma Head and Neck Salivary Gland Carcinoma Osteosarcoma HER2 - Enriched Breast Carcinoma Embryonal Rhabdomyosarcoma Adenosquamous NSCLC Diffuse Large B - cell Lymphoma (DLBCL) Sarcomatoid Carcinoma of the Lung Adenocarcinoma NSCLC Head and Neck Squamous Cell Carcinoma (HNSCC) Alveolar Rhabdomyosarcoma Ovarian Mucinous Carcinoma Adrenocortical Carcinoma Kidney Renal Clear Cell Carcinoma Hepatocellular Carcinoma Bladder Urothelial Carcinoma Cervical Squamous Cell Carcinoma Non - Squamous Anal Carcinoma Pancreatic Neuroendocrine Adenocarcinoma Prostate Neuroendocrine Adenocarcinoma Liposarcoma Undifferentiated Pleomorphic Sarcoma Acute Myeloid Leukemia (AML) Ewing Sarcoma Ovarian Leiomyosarcoma Breast Carcinoma, Luminal A Breast Carcinoma, Luminal B Squamous Anal Carcinoma Stomach Adenocarcinoma Esophageal Adenocarcinoma Fibrosarcoma Anaplastic Thyroid Carcinoma (…) Indication a z - cel ( I M A 203 ) PRAME Cell Therapy MA402 PRAME Bispecific Today’s Focus IMA203CD8 PRAME Cell Therapy (GEN2) • Enhanced pharmacology • Potential to expand to tumor - agnostic label in 2L PRAME cancers across broad spectrum of PRAME expression level • Ovarian carcinoma chosen as initial proof - of - concept Positioning of IMA203CD8: Expanding to PRAME Cancers beyond Melanoma
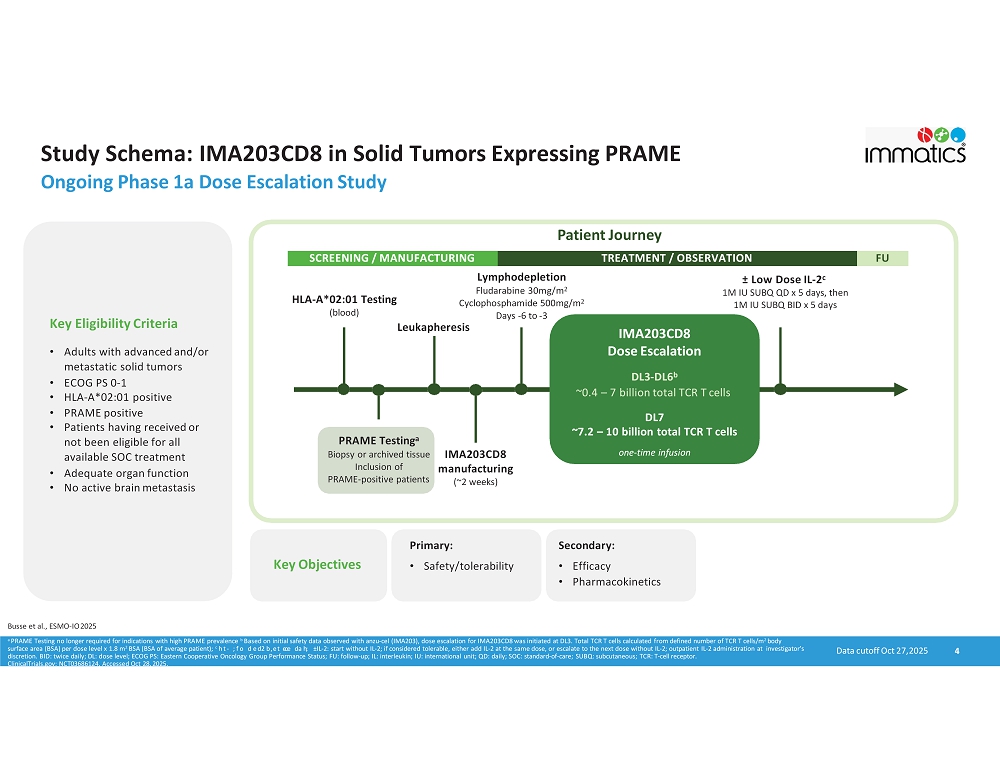
Study Schema: IMA203CD8 in Solid Tumors Expressing PRAME Ongoing Phase 1a Dose Escalation Study 4 Busse et al., ESMO - IO 2025 PRAME Testing a Biopsy or archived tissue Inclusion of PRAME - positive patients IMA203CD8 manu f a cturing (~2 weeks) Lymphodepletion Fludarabine 30mg/m 2 Cyclophosphamide 500mg/m 2 Days - 6 to - 3 ц Low Dose IL - 2 c 1M IU SUBQ QD x 5 days, then 1M IU SUBQ BID x 5 days Leukapheresis HLA - A*02:01 Testing (blood) Patient Journey SCREENING / MANUFACTURING TREATMENT / OBSERVATION FU Key Eligibility Criteria • Adults with advanced and/or metastatic solid tumors • ECOG PS 0 - 1 • HLA - A*02:01 positive • PRAME positive • Patients having received or not been eligible for all available SOC treatment • Adequate organ function • No active brain metastasis IMA203CD8 Dose Escalation DL3 - DL6 b ~0.4 – 7 billion total TCR T cells DL7 ~7.2 – 10 billion total TCR T cells one - time infusion Key Objectives Primary: • Safety/tolerability Secondary: • Efficacy • Pharmacokinetics Data cutoff Oct 27, 2025 a PRAME Testing no longer required for indications with high PRAME prevalence b Based on initial safety data observed with anzu - cel (IMA203), dose escalation for IMA203CD8 was initiated at DL3. Total TCR T cells calculated from defined number of TCR T cells/m 2 body surface area (BSA) per dose level x 1.8 m 2 BSA (BSA of average patient); c h t - ;fo d e d 2 b,et eo e da h ; ц IL - 2: start without IL - 2; if considered tolerable, either add IL - 2 at the same dose, or escalate to the next dose without IL - 2; outpatient IL - 2 administration at investigator’s discretion. BID: twice daily; DL: dose level; ECOG PS: Eastern Cooperative Oncology Group Performance Status; FU: follow - up; IL: interleukin; IU: international unit; QD: daily; SOC: standard - of - care; SUBQ: subcutaneous; TCR: T - cell receptor. ClinicalTrials.gov: NCT03686124, Accessed Oct 28, 2025.
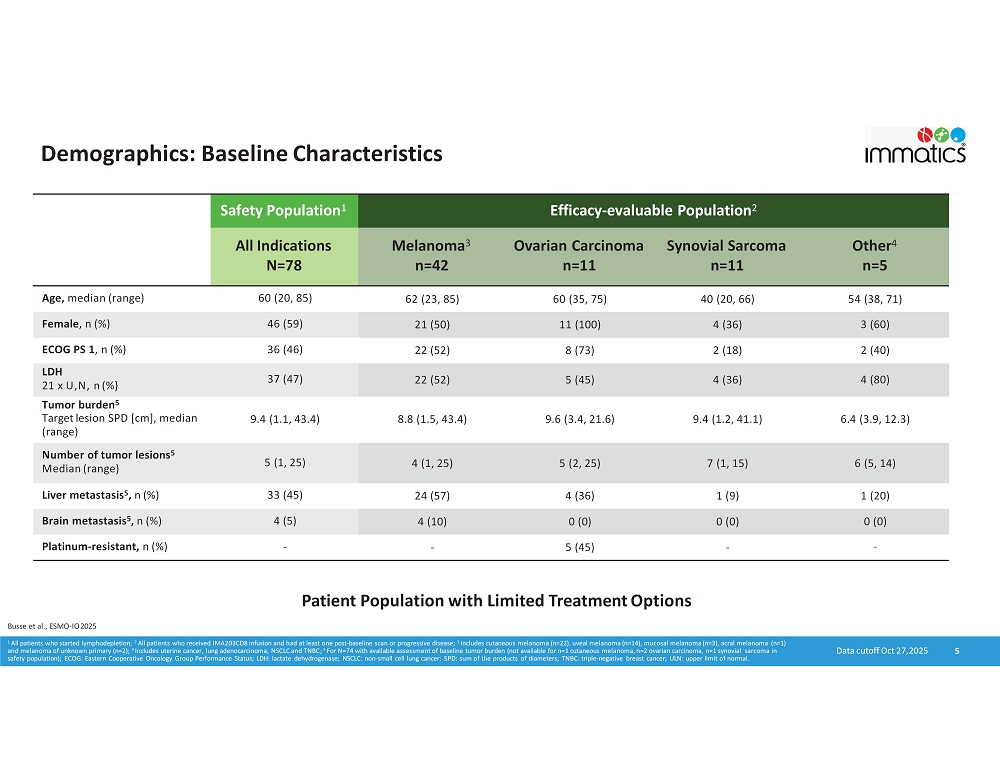
Demographics: Baseline Characteristics 5 Efficacy - evaluable Population 2 Safety Population 1 Other 4 n=5 Synovial Sarcoma n=11 Ovarian Carcinoma n=11 Melan o m a 3 n=42 All Indications N=78 54 (38, 71) 40 (20, 66) 60 (35, 75) 62 (23, 85) 60 (20, 85) Age, median (range) 3 (60) 4 (36) 11 (100) 21 (50) 46 (59) Female , n (%) 2 (40) 2 (18) 8 (73) 22 (52) 36 (46) ECOG PS 1 , n (%) 4 (80) 4 (36) 5 (45) 22 (52) 37 (47) LDH 21 x U,N, n (%} Tumor burden 5 6.4 (3.9, 12.3) 9.4 (1.2, 41.1) 9.6 (3.4, 21.6) 8.8 (1.5, 43.4) 9.4 (1.1, 43.4) Target lesion SPD [cm], median (range) 6 (5, 14) 7 (1, 15) 5 (2, 25) 4 (1, 25) 5 (1, 25) Number of tumor lesions 5 Median (range) 1 (20) 1 (9) 4 (36) 24 (57) 33 (45) Liver metastasis 5 , n (%) 0 (0) 0 (0) 0 (0) 4 (10) 4 (5) Brain metastasis 5 , n (%) - - 5 (45) - - Platinum - resistant, n (%) Data cutoff Oct 27, 2025 Patient Population with Limited Treatment Options Busse et al., ESMO - IO 2025 1 All patients who started lymphodepletion; 2 All patients who received IMA203CD8 infusion and had at least one post - baseline scan or progressive disease; 3 Includes cutaneous melanoma (n=22), uveal melanoma (n=14), mucosal melanoma (n=3), acral melanoma (n=1) and melanoma of unknown primary (n=2); 4 Includes uterine cancer, lung adenocarcinoma, NSCLC and TNBC; 5 For N=74 with available assessment of baseline tumor burden (not available for n=1 cutaneous melanoma, n=2 ovarian carcinoma, n=1 synovial sarcoma in safety population); ECOG: Eastern Cooperative Oncology Group Performance Status; LDH: lactate dehydrogenase; NSCLC: non - small cell lung cancer; SPD: sum of the products of diameters; TNBC: triple - negative breast cancer; ULN: upper limit of normal.
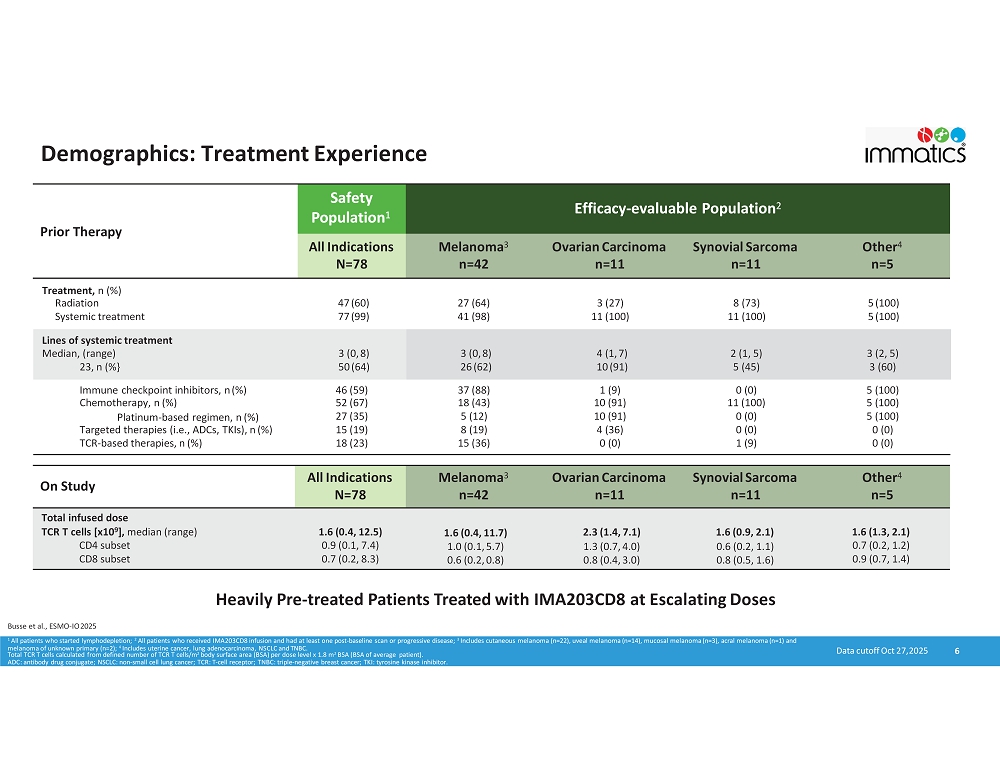
Demographics: Treatment Experience 6 Efficacy - evaluable Population 2 Safety P o pu l at i o n 1 Prior Therapy O the r 4 n=5 Synovial Sarcoma n=11 Ovarian Carcinoma n=11 Melanoma 3 n=42 All Indications N=78 Treatment, n (%) 5 (100) 8 (73) 3 (27) 27 (64) 47 (60) Radiation 5 (100) 11 (100) 11 (100) 41 (98) 77 (99) Systemic treatment Lines of systemic treatment 3 (2, 5) 2 (1, 5) 4 (1, 7) 3 (0, 8) 3 (0, 8) Median, (range) 3 (60) 5 (45) 10 (91) 26 (62) 50 (64) 23, n (%} 5 (100) 0 (0) 1 (9) 37 (88) 46 (59) Immune checkpoint inhibitors, n (%) 5 (100) 11 (100) 10 (91) 18 (43) 52 (67) Chemotherapy, n (%) 5 (100) 0 (0) 10 (91) 5 (12) 27 (35) Platinum - based regimen, n (%) 0 (0) 0 (0) 4 (36) 8 (19) 15 (19) Targeted therapies (i.e., ADCs, TKIs), n (%) 0 (0) 1 (9) 0 (0) 15 (36) 18 (23) TCR - based therapies, n (%) Data cutoff Oct 27, 2025 Busse et al., ESMO - IO 2025 O the r 4 n=5 Synovial Sarcoma n=11 Ovarian Carcinoma n=11 Melanoma 3 n=42 All Indications N=78 On Study Total infused dose 1.6 (1.3, 2.1) 1.6 (0.9, 2.1) 2.3 (1.4, 7.1) 1.6 (0.4, 11.7) 1.6 (0.4, 12.5) TCR T cells [x10 9 ], median (range) 0.7 (0.2, 1.2) 0.6 (0.2, 1.1) 1.3 (0.7, 4.0) 1.0 (0.1, 5.7) 0.9 (0.1, 7.4) CD4 subset 0.9 (0.7, 1.4) 0.8 (0.5, 1.6) 0.8 (0.4, 3.0) 0.6 (0.2, 0.8) 0.7 (0.2, 8.3) CD8 subset Heavily Pre - treated Patients Treated with IMA203CD8 at Escalating Doses 1 All patients who started lymphodepletion; 2 All patients who received IMA203CD8 infusion and had at least one post - baseline scan or progressive disease; 3 Includes cutaneous melanoma (n=22), uveal melanoma (n=14), mucosal melanoma (n=3), acral melanoma (n=1) and melanoma of unknown primary (n=2); 4 Includes uterine cancer, lung adenocarcinoma, NSCLC and TNBC. Total TCR T cells calculated from defined number of TCR T cells/m 2 body surface area (BSA) per dose level x 1.8 m 2 BSA (BSA of average patient). ADC: antibody drug conjugate; NSCLC: non - small cell lung cancer; TCR: T - cell receptor; TNBC: triple - negative breast cancer; TKI: tyrosine kinase inhibitor.
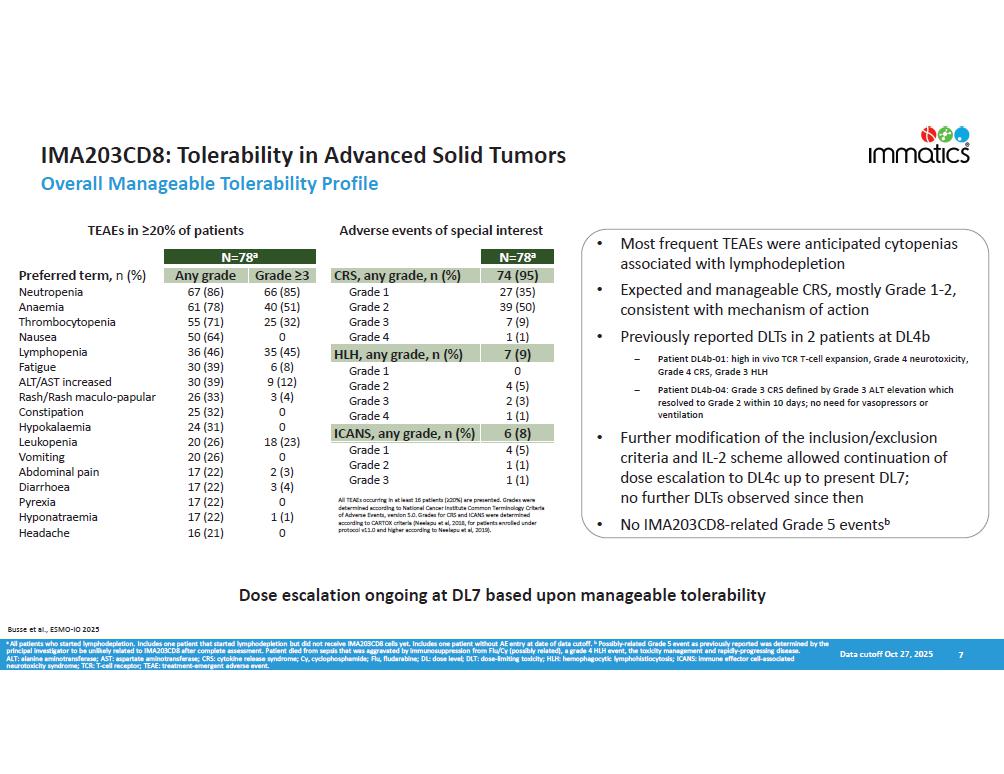
IMA203CD8: Tolerability in Advanced Solid Tumors Overall Manageable Tolerability Profile 7 • Most frequent TEAEs were anticipated cytopenias associated with lymphodepletion • Expected and manageable CRS, mostly Grade 1 - 2, consistent with mechanism of action • Previously reported DLTs in 2 patients at DL4b Patient DL4b - 01: high in vivo TCR T - cell expansion, Grade 4 neurotoxicity, Grade 4 CRS, Grade 3 HLH Patient DL4b - 04: Grade 3 CRS defined by Grade 3 ALT elevation which resolved to Grade 2 within 10 days; no need for vasopressors or ventilation • Further modification of the inclusion/exclusion criteria and IL - 2 scheme allowed continuation of dose escalation to DL4c up to present DL7; no further DLTs observed since then • No IMA203CD8 - related Grade 5 events b TEAEs in ೦ 20% of patients Adverse events of special interest N=78 a Grade ೦ 3 Any grade Preferred term, n (%) 66 (85) 67 (86) Neutropenia 40 (51) 61 (78) Anaemia 25 (32) 55 (71) Thrombocytopenia 0 50 (64) Nausea 35 (45) 36 (46) Lymphopenia 6 (8) 30 (39) Fatigue 9 (12) 30 (39) ALT/AST increased 3 (4) 26 (33) Rash/Rash maculo - papular 0 25 (32) Constipation 0 24 (31) Hypokalaemia 18 (23) 20 (26) Leukopenia 0 20 (26) Vomiting 2 (3) 17 (22) Abdominal pain 3 (4) 17 (22) Diarrhoea 0 17 (22) Pyrexia 1 (1) 17 (22) Hyponatraemia 0 16 (21) Headache N=78 a 74 (95) CRS, any grade, n (%) 27 (35) Grade 1 39 (50) Grade 2 7 (9) Grade 3 1 (1) Grade 4 7 (9) HLH, any grade, n (%) 0 Grade 1 4 (5) Grade 2 2 (3) Grade 3 1 (1) Grade 4 6 (8) ICANS, any grade, n (%) 4 (5) Grade 1 1 (1) Grade 2 1 (1) Grade 3 Dose escalation ongoing at DL7 based upon manageable tolerability Data cutoff Oct 27, 2025 dd h ho ftta en en h d oh 1 he nho (2 0%} o nh ; ; o determined according to National Cancer Institute Common Terminology Criteria of Adverse Events, version 5.0. Grades for CRS and ICANS were determined according to CARTOX criteria (Neelapu et al, 2018, for patients enrolled under protocol v11.0 and higher according to Neelapu et al, 2019). Busse et al., ESMO - IO 2025 a All patients who started lymphodepletion. Includes one patient that started lymphodepletion but did not receive IMA203CD8 cells yet. Includes one patient without AE entry at date of data cutoff. b Possibly - related Grade 5 event as previously reported was determined by the principal investigator to be unlikely related to IMA203CD8 after complete assessment. Patient died from sepsis that was aggravated by immunosuppression from Flu/Cy (possibly related), a grade 4 HLH event, the toxicity management and rapidly - progressing disease. ALT: alanine aminotransferase; AST: aspartate aminotransferase; CRS: cytokine release syndrome; Cy, cyclophosphamide; Flu, fludarabine; DL: dose level; DLT: dose - limiting toxicity; HLH: hemophagocytic lymphohistiocytosis; ICANS: immune effector cell - associated neurotoxicity syndrome; TCR: T - cell receptor; TEAE: treatment - emergent adverse event.
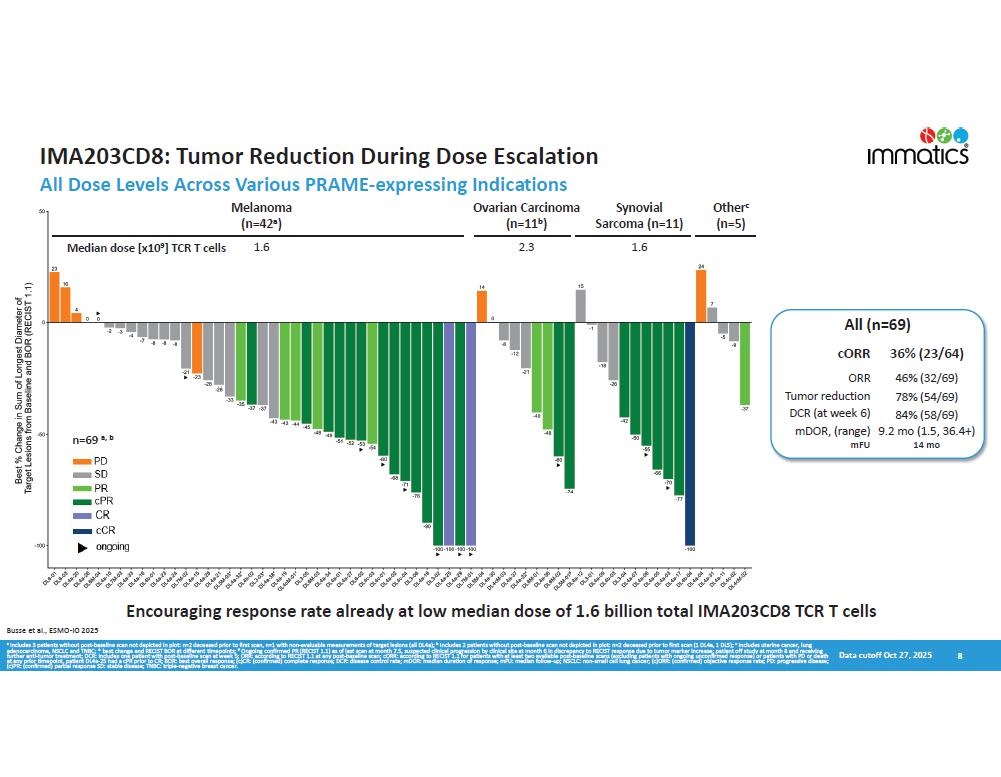
8 n=69 a, b Me lanoma (n=42 a ) Ovarian Carcinoma (n=11 b ) Synovial Sarcoma (n=11) Othe r c (n=5) 1 . 6 2 . 3 1 . 6 All (n=69) 36% (23/64) cORR 46% (32/69) OR R 78% (54/69) Tumor reduction 84% (58/69) DCR (at week 6) 9.2 mo (1.5, 36.4+) mDOR, (range) 14 mo mFU IMA203CD8: Tumor Reduction During Dose Escalation All Dose Levels Across Various PRAME - expressing Indications Encouraging response rate already at low median dose of 1.6 billion total IMA203CD8 TCR T cells Busse et al., ESMO - IO 2025 a Includes 3 patients without post - baseline scan not depicted in plot: n=2 deceased prior to first scan, n=1 with non - evaluable measurements of target lesions (all DL4a); b Includes 2 patients without post - baseline scan not depicted in plot: n=2 deceased prior to first scan (1 DL4a, 1 DL5); c Includes uterine cancer, lung adenocarcinoma, NSCLC and TNBC; * best change and RECIST BOR at different timepoints; # Ongoing confirmed PR (RECIST 1.1) as of last scan at month 7.5, suspected clinical progression by clinical site at month 6 in discrepancy to RECIST response due to tumor marker increase; patient off study at month 8 and receiving further anti - tumor treatment; DCR: includes one patient with post - baseline scan at week 5; ORR: according to RECIST 1.1 at any post - baseline scan; cORR: according to RECIST 1.1 for patients with at least two available post - baseline scans (excluding patients with ongoing unconfirmed response) or patients with PD or death Data cutoff Oct 27, 2025 at any prior timepoint, patient DL4a - 25 had a cPR prior to CR; BOR: best overall response; (c)CR: (confirmed) complete response; DCR: disease control rate; mDOR: median duration of response; mFU: median follow - up; NSCLC: non - small cell lung cancer; (c)ORR: (confirmed) objective response rate; PD: progressive disease; (c)PR: (confirmed) partial response SD: stable disease; TNBC: triple - negative breast cancer. Median dose [x10 9 ] TCR T cells
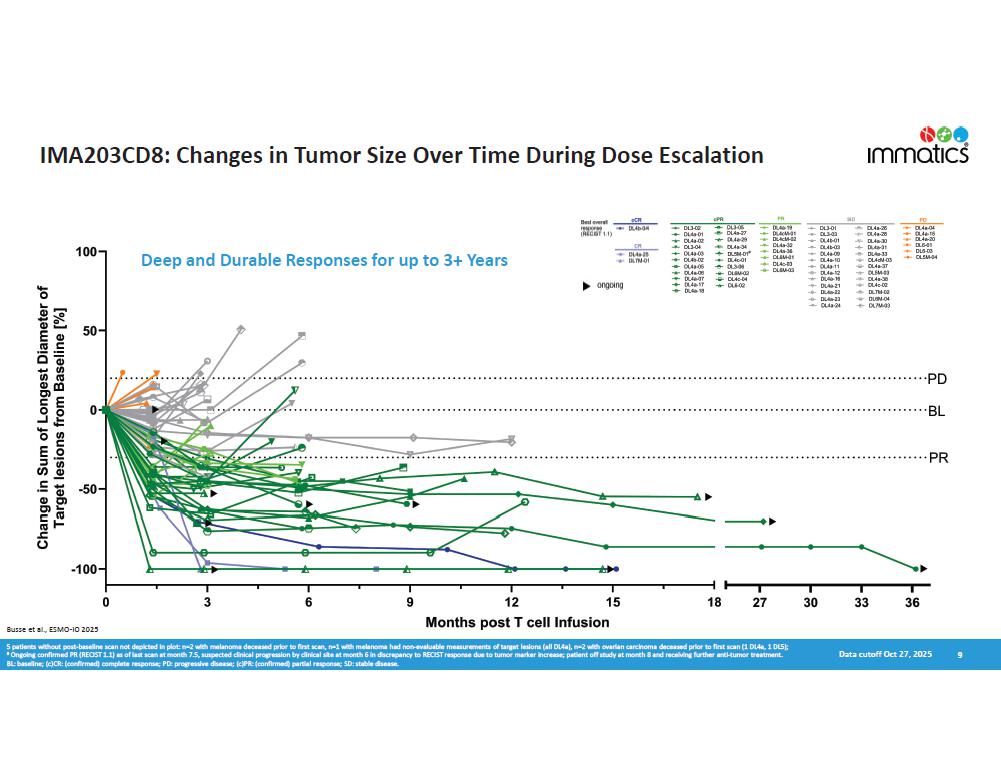
IMA203CD8: Changes in Tumor Size Over Time During Dose Escalation 9 Data cutoff Oct 27, 2025 Busse et al., ESMO - IO 2025 Deep and Durable Responses for up to 3+ Years 5 patients without post - baseline scan not depicted in plot: n=2 with melanoma deceased prior to first scan, n=1 with melanoma had non - evaluable measurements of target lesions (all DL4a), n=2 with ovarian carcinoma deceased prior to first scan (1 DL4a, 1 DL5); # Ongoing confirmed PR (RECIST 1.1) as of last scan at month 7.5, suspected clinical progression by clinical site at month 6 in discrepancy to RECIST response due to tumor marker increase; patient off study at month 8 and receiving further anti - tumor treatment. BL: baseline; (c)CR: (confirmed) complete response; PD: progressive disease; (c)PR: (confirmed) partial response; SD: stable disease.
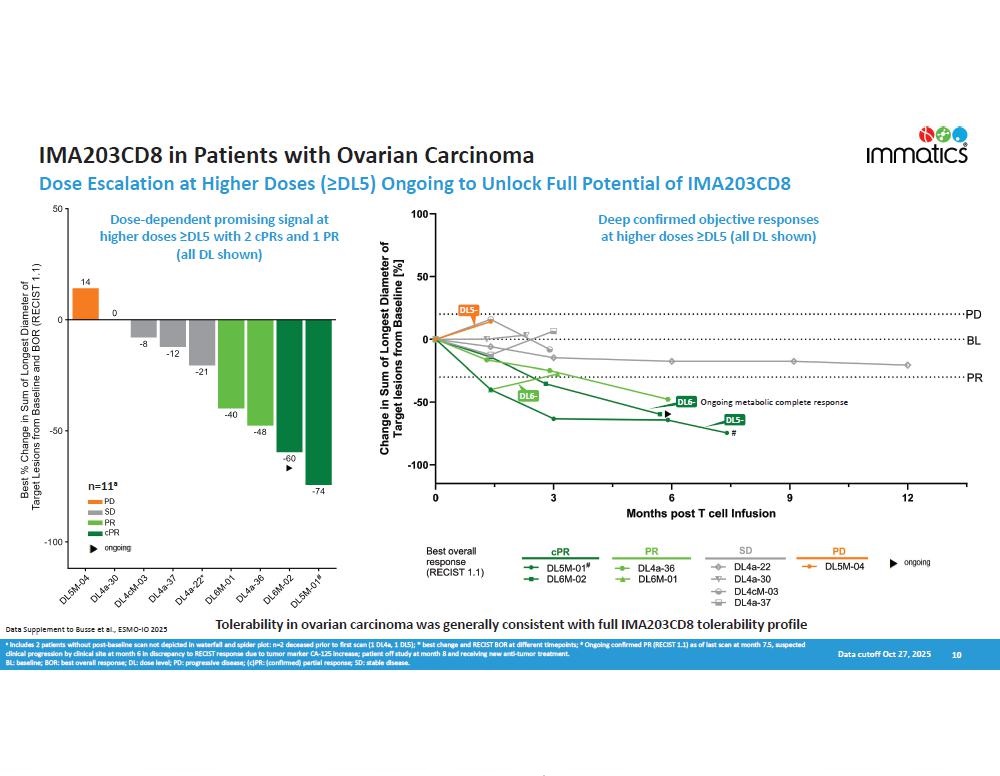
IMA203CD8 in Patients with Ovarian Carcinoma Dose Escalation at Higher Doses ( ೦ DLS) Ongoing to Unlock Full Potential of IMA203CD8 10 Dose - dependent promising signal at higher doses ೦ DLS with 2 cPRs and 1 PR (all DL shown) Deep confirmed objective responses at higher doses ೦ DLS (all DL shown) n=11 a Data cutoff Oct 27, 2025 a Includes 2 patients without post - baseline scan not depicted in waterfall and spider plot: n=2 deceased prior to first scan (1 DL4a, 1 DL5); * best change and RECIST BOR at different timepoints; # Ongoing confirmed PR (RECIST 1.1) as of last scan at month 7.5, suspected clinical progression by clinical site at month 6 in discrepancy to RECIST response due to tumor marker CA - 125 increase; patient off study at month 8 and receiving new anti - tumor treatment. BL: baseline; BOR: best overall response; DL: dose level; PD: progressive disease; (c)PR: (confirmed) partial response; SD: stable disease. Tolerability in ovarian carcinoma was generally consistent with full IMA203CD8 tolerability profile D L 6 - D L 5 - D L 5 - # DL6 - Ongoing metabolic complete response Data Supplement to Busse et al., ESMO - IO 2025
Conclusions Towards Proof - of - concept for Tumor - agnostic Targeting of PRAME cancers with IMA203CD8 • M n bd hfd bedehy h ent oen ;fo d e do eh - mfoh f qa nh 2 ; 3 ho b en nhete h ; tyhf ne • Encouraging clinical anti - tumor activity after one - time infusion of IMA203CD8 already at a low median dose of 1.6 billion total TCR T cells • Deep and durable objective responses in advanced solid tumors during dose escalation including beyond melanoma • 3 complete responses plus 2 cPRs with - 100% reduction of target lesions • 66% (21/32) of responders showing deep responses with tumor ;athefn ff 2 50% • 7 responses ongoing for ೦ 1 year post infusion • Promising initial dose - dependent signal in S patients with ovarian carcinoma treated at ೦ DLS : 2 cPRs, including 1 ongoing metabolic complete response, and 1 PR – all observed without post - infusion low - dose IL - 2 • Early proof - of - concept data in ovarian carcinoma supports the strategy to position IMA203CD8 in the tumor - agnostic setting of advanced PRAME cancers beyond melanoma, starting with gynecologic cancers • The Phase 1 trial could also support the positioning of IMA203CD8 without the requirement of post - infusion low - dose IL - 2 in the future • Dose escalation and determination of RP2D on track to be completed in 2026 to unlock the full clinical potential of IMA203CD8 • Efficacy readouts including patients treated at the two highest dose levels (DL6 and DL7) expected in 2026 11 Data cutoff Oct 27, 2025 Busse et al., ESMO - IO 2025 AE: adverse event; cPR: confirmed partial response; RP2D: recommended phase 2 dose.
University Hospital Dresden University Hospital Bonn University Hospital Würzburg University Hospital Hamburg Charité Berlin University Hospital Heidelberg University Medicine Mainz TUM University Hospital Munich IMA203CD8 Phase 1 Study Sponsor: Immatics Massachusetts General Hospital University of Pittsburgh Medical Center MD Anderson Cancer Center United States University of Miami Health System Fox Chase Cancer Center Thank You – Study Participants & Caregivers 12 Germany

Appendix 13
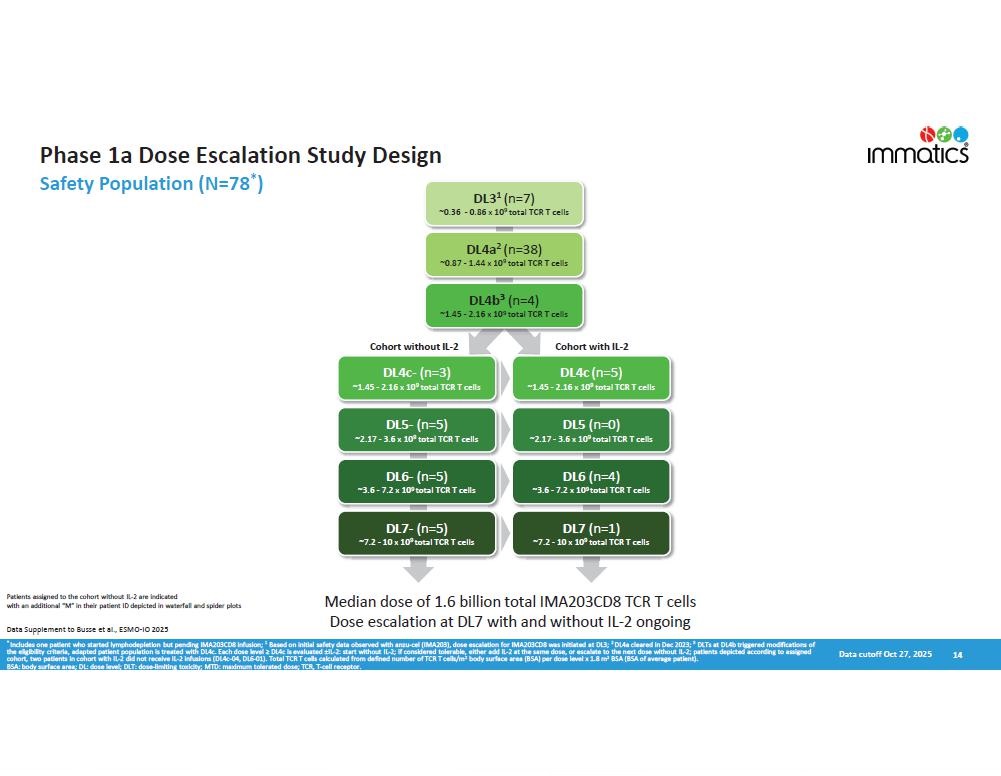
Phase 1a Dose Escalation Study Design Safety Population (N=78 * ) DL3 1 (n=7) DL4c (n=5) ~1.45 - 2.16 x 10 9 total TCR T cells DL5 (n=0) ~2.17 - 3.6 x 10 9 total TCR T cells DL6 (n=4) ~3.6 - 7.2 x 10 9 total TCR T cells DL7 (n=1) ~7.2 - 10 x 10 9 total TCR T cells DL4c - (n=3) ~1.45 - 2.16 x 10 9 total TCR T cells DL5 - (n=5) ~2.17 - 3.6 x 10 9 total TCR T cells DL6 - (n=5) ~3.6 - 7.2 x 10 9 total TCR T cells DL7 - (n=5) ~7.2 - 10 x 10 9 total TCR T cells Median dose of 1.6 billion total IMA203CD8 TCR T cells Dose escalation at DL7 with and without IL - 2 ongoing 14 Data cutoff Oct 27, 2025 ~0.36 - 0.86 x 10 9 total TCR T cells DL4a 2 (n=38) ~0.87 - 1.44 x 10 9 total TCR T cells DL4b 3 (n=4) ~1.45 - 2.16 x 10 9 total TCR T cells Cohort without IL - 2 Cohort with IL - 2 * Includes one patient who started lymphodepletion but pending IMA203CD8 infusion; 1 Based on initial safety data observed with anzu - cel (IMA203), dose escalation for IMA203CD8 was initiated at DL3; 2 DL4a cleared in Dec 2023; 3 DLTs at DL4b triggered modifications of h - de ebedehy t eh e , ; h ; he nh f ad hefn eo h h ; eh - b,et h t - ;fo d e d 2 b,et eo e da h ; ц IL - 2: start without IL - 2; if considered tolerable, either add IL - 2 at the same dose, or escalate to the next dose without IL - 2; patients depicted according to assigned cohort, two patients in cohort with IL - 2 did not receive IL - 2 infusions (DL4c - 04, DL6 - 01). Total TCR T cells calculated from defined number of TCR T cells/m 2 body surface area (BSA) per dose level x 1.8 m 2 BSA (BSA of average patient). BSA: body surface area; DL: dose level; DLT: dose - limiting toxicity; MTD: maximum tolerated dose; TCR, T - cell receptor. Patients assigned to the cohort without IL - 2 are indicated with an additional “M” in their patient ID depicted in waterfall and spider plots Data Supplement to Busse et al., ESMO - IO 2025
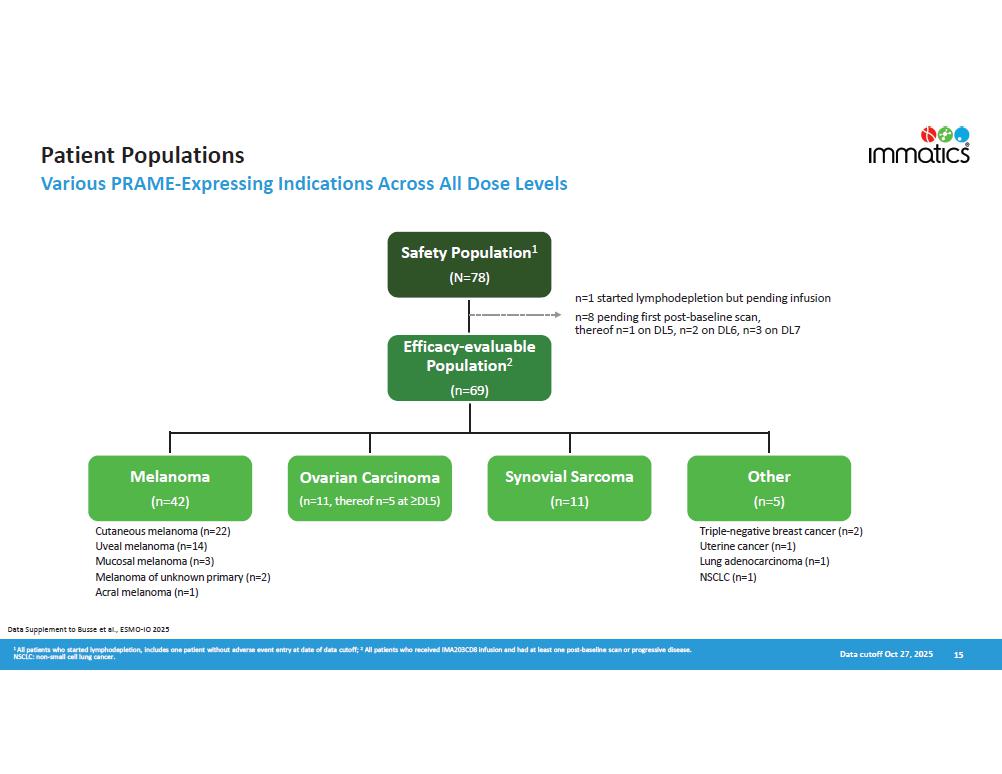
Other (n=5) 15 Safety Population 1 (N=78) n=1 started lymphodepletion but pending infusion n=8 pending first post - baseline scan, thereof n=1 on DL5, n=2 on DL6, n=3 on DL7 E ffi c acy - e v aluable Population 2 (n=69) Melanoma (n=42) Ovarian Carcinoma (n=11, thereof n=5 at 2b,5} Synovial Sarcoma (n=11) Patient Populations Various PRAME - Expressing Indications Across All Dose Levels Cutaneous melanoma (n=22) Uveal melanoma (n=14) Mucosal melanoma (n=3) Melanoma of unknown primary (n=2) Acral melanoma (n=1) 1 All patients who started lymphodepletion, includes one patient without adverse event entry at date of data cutoff; 2 All patients who received IMA203CD8 infusion and had at least one post - baseline scan or progressive disease. NSCLC: non - small cell lung cancer. Triple - negative breast cancer (n=2) Uterine cancer (n=1) Lung adenocarcinoma (n=1) NSCLC (n=1) Data cutoff Oct 27, 2025 Data Supplement to Busse et al., ESMO - IO 2025
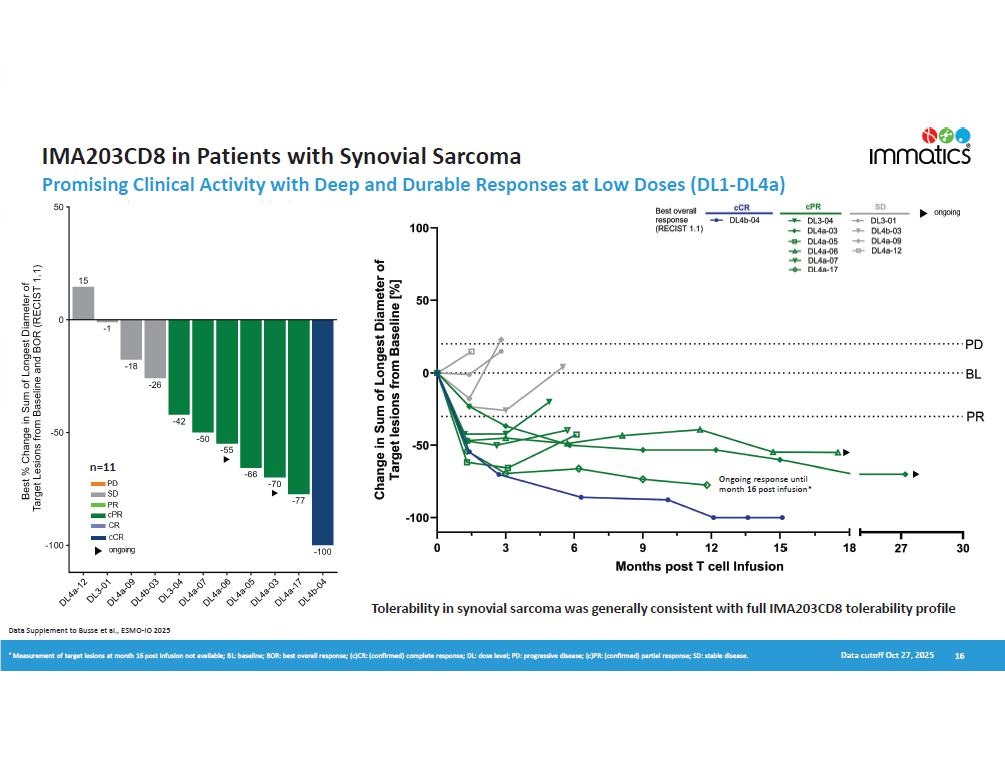
IMA203CD8 in Patients with Synovial Sarcoma Promising Clinical Activity with Deep and Durable Responses at Low Doses (DL1 - DL4a) 16 Data cutoff Oct 27, 2025 Tolerability in synovial sarcoma was generally consistent with full IMA203CD8 tolerability profile n=11 Ongoing response until month 16 post infusion* Data Supplement to Busse et al., ESMO - IO 2025 * Measurement of target lesions at month 16 post infusion not available; BL: baseline; BOR: best overall response; (c)CR: (confirmed) complete response; DL: dose level; PD: progressive disease; (c)PR: (confirmed) partial response; SD: stable disease.
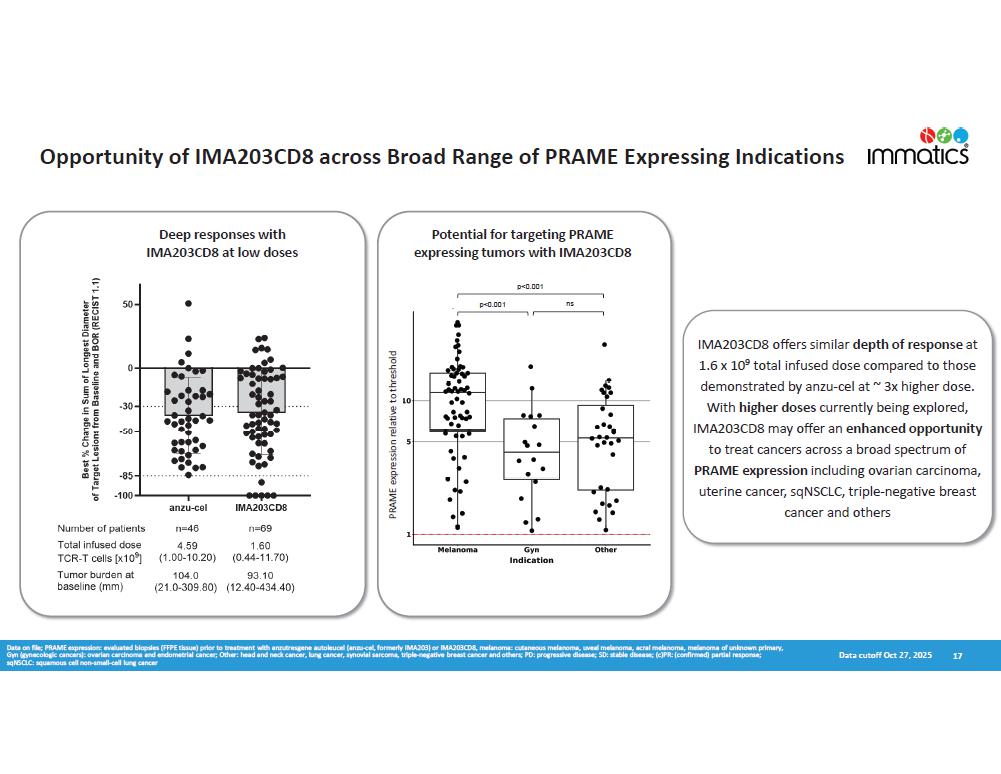
Opportunity of IMA203CD8 across Broad Range of PRAME Expressing Indications 17 Data on file; PRAME expression: evaluated biopsies (FFPE tissue) prior to treatment with anzutresgene autoleucel (anzu - cel, formerly IMA203) or IMA203CD8, melanoma: cutaneous melanoma, uveal melanoma, acral melanoma, melanoma of unknown primary, Gyn (gynecologic cancers): ovarian carcinoma and endometrial cancer; Other: head and neck cancer, lung cancer, synovial sarcoma, triple - negative breast cancer and others; PD: progressive disease; SD: stable disease; (c)PR: (confirmed) partial response; sqNSCLC: squamous cell non - small - cell lung cancer IMA 203 CD 8 offers similar depth of response at 1 . 6 x 10 9 total infused dose compared to those demonstrated by anzu - cel at ~ 3 x higher dose . With higher doses currently being explored, IMA203CD8 may offer an enhanced opportunity to treat cancers across a broad spectrum of PRAME expression including ovarian carcinoma, uterine cancer, sqNSCLC, triple - negative breast cancer and others Deep responses with IMA203CD8 at low doses Potential for targeting PRAME expressing tumors with IMA203CD8 p<0.001 ns p<0.001 Data cutoff Oct 27, 2025 PRAME expression relative to threshold
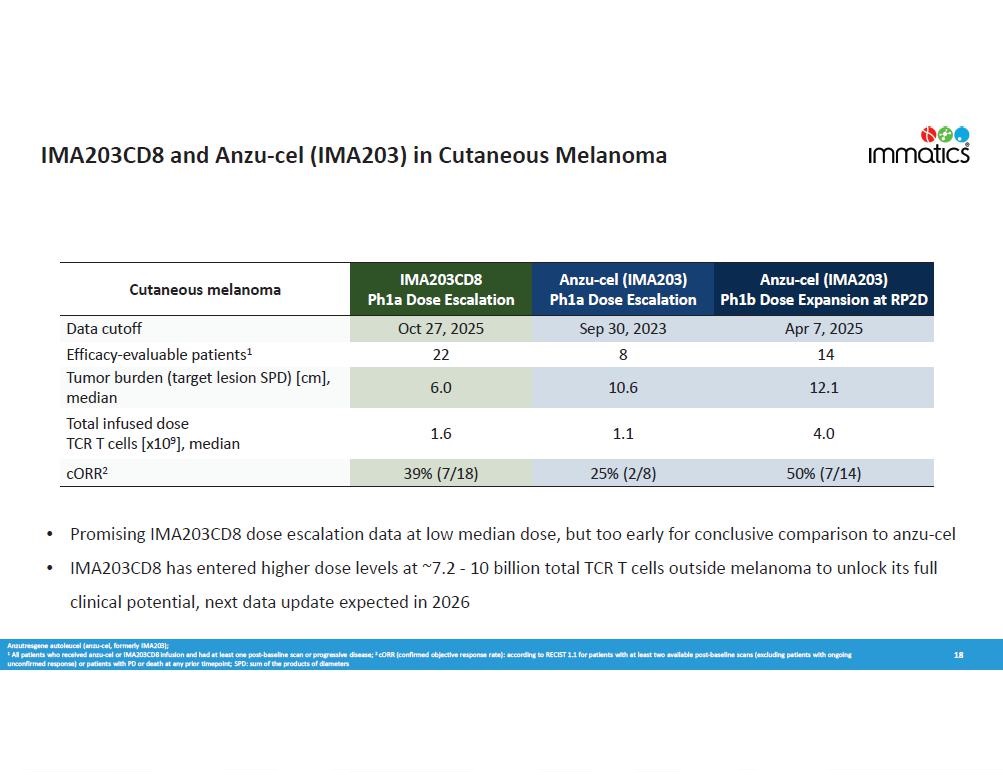
IMA203CD8 and Anzu - cel (IMA203) in Cutaneous Melanoma 18 • Promising IMA203CD8 dose escalation data at low median dose, but too early for conclusive comparison to anzu - cel • IMA203CD8 has entered higher dose levels at ~7.2 - 10 billion total TCR T cells outside melanoma to unlock its full clinical potential, next data update expected in 2026 Anzutresgene autoleucel (anzu - cel, formerly IMA203); 1 All patients who received anzu - cel or IMA203CD8 infusion and had at least one post - baseline scan or progressive disease; 2 cORR (confirmed objective response rate): according to RECIST 1.1 for patients with at least two available post - baseline scans (excluding patients with ongoing unconfirmed response) or patients with PD or death at any prior timepoint; SPD: sum of the products of diameters Anzu - cel (IMA203) Ph1b Dose Expansion at RP2D Anzu - cel (IMA203) Ph1a Dose Escalation IMA203CD8 Ph1a Dose Escalation Cutaneous melanoma Sep 30, 2023 Apr 7, 2025 Oct 27, 2025 Data cutoff 14 8 22 Efficacy - evaluable patients 1 12.1 10.6 6.0 Tumor burden (target lesion SPD) [cm], median 4.0 1.1 1.6 Total infused dose TCR T cells [x10 9 ], median 50% (7/14) 25% (2/8) 39% (7/18) cORR 2