.6
PRESENTED BY: First - in - Human Results With IMA401 , a MAGEA4 /8 - targeted T - cell Receptor - based Bispecific T - cell Engager ( TCER ), in Recurrent or Refractory Solid Tumors Martin Wermke¹ , Dirk Jaeger² , Annalen Bleckmann³ , Manik Chatterjee⁴, Stefanie Groepper ⁵, Daniel Heudobler ⁶, Judith S Hecker⁷, Silvia Spoerl ⁸, Martin Sebastian⁹, Moritz Kleemiss¹ ⁰, Heiko Becker¹¹ , Stefan Knop¹² , Farastuk Bozorgmehr¹³ , Mathias Haenel¹ ⁴, Sarah Missel¹ ⁵, Carsten Reinhardt¹ ⁵, Olga Veremchuk¹ ⁵, Manuel Ruh¹ ⁵, Cedrik Michael Britten¹ ⁵, Sebastian Ochsenreither¹ ⁶ ¹ TU Dresden University of Technology, NCT/UCC Early Clinical Trial Unit, Dresden, Germany; ² National Centre for Tumor Diseases , Heidelberg, Germany; ³ Universitätsklinikum Münster, Münster, Germany; ⁴ University of Wuerzburg , Medizinische Klinik 2, Würzburg, Germany; ⁵ Marien Hospital Dusseldorf , Düsseldorf, Germany; ⁶ University Hospital Regensburg, Regensburg, Germany; ⁷ Department of Medicine III, Technical University of Munich, Munich, Germany; ⁸ University Hospital Erlangen, Erlangen, Germany; ⁹ University Hospital Frankfurt, Frankfurt, Germany; ¹⁰ University Hospital Bonn, Bonn, Germany; ¹¹ Depart men t of Hematology , Oncology , and Stem Cell Transplantation, Medical Center – University of Freiburg, Freiburg, Germany; ¹² Nuremberg General Hospital, Nuremberg , Germany; ¹³ Thoraxklinik Heidelberg gGmbH, University Hospital Heidelberg, Heidelberg, Germany; ¹⁴ Klinikum Chemnitz gGmbH, Chemnitz, Germany ¹⁵ Immatics Biotech nol ogies GmbH, Tübingen, Germany; ¹⁶ Charite Universitätsmedizin Berlin, Berlin, Germany Prof. Dr. med. Martin Wermke, Abstract #2507
PRESENTED BY: Key Takeaways • TCR - based therapies enable immune recognition of intracellular tumor antigens presented by cell - surface HLA, expanding the therapeutic landscape beyond targets accessible to conventional immunotherapies • IMA401 is a novel TCR - based bispecific T - cell engager targeting MAGEA4/8, expressed in multiple cancers incl. head & neck cancer and sqNSCLC • IMA401 demonstrates a manageable tolerability profile and encouraging efficacy as monotherapy or in combination with ICI • Next steps include a combination with a PRAME - directed TCR - based T - cell engager (IMA402) for >90% prevalence in sqNSCLC Prof. Dr. med. Martin Wermke, Abstract #2507 HLA, human leukocyte antigen; head and neck (H&N) cancer (squamous cell and adenocarcinoma); ICI, immune checkpoint inhibitor ; M AGE, melanoma - assicated antigen; PRAME, preferentially expressed in melanoma; sqNSCLC , squamous cell non - small cell lung cancer; TCR: T - cell receptor; Dose escalation data presented by Wermke et al., ESMO 2024. Data cutoff Mar 02, 2026
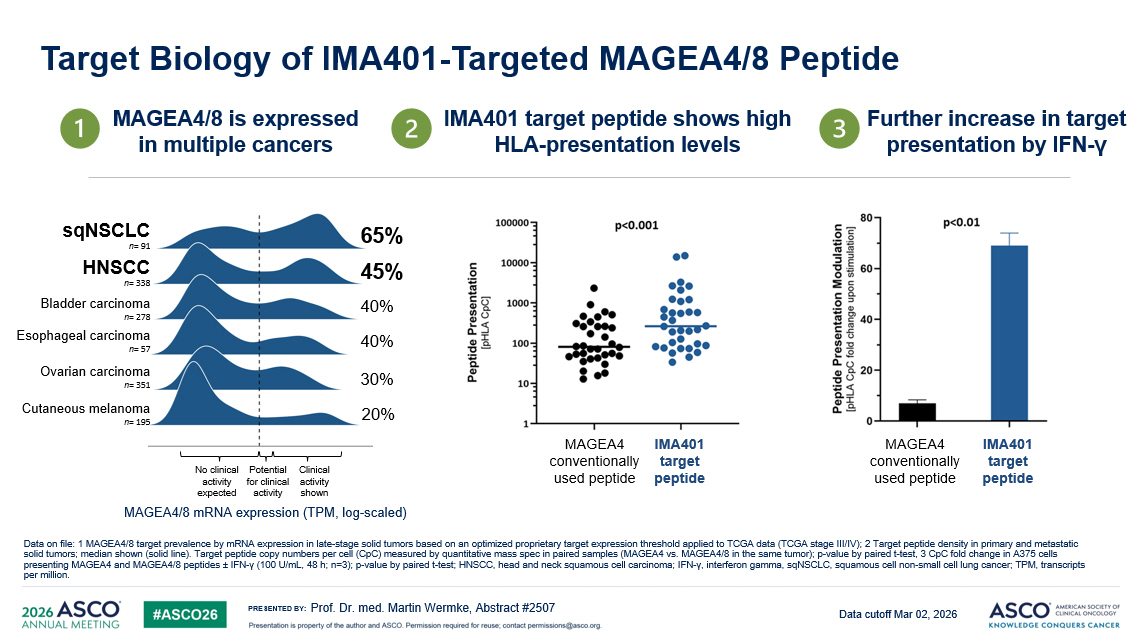
PRESENTED BY: Target Biology of IMA401 - Targeted MAGEA4/8 Peptide Prof. Dr. med. Martin Wermke, Abstract #2507 45% 40% 40% 30% 20% 65% Cutaneous melanoma n = 195 HNSCC n = 338 Ovarian carcinoma n = 351 sqNSCLC n = 91 Esophageal carcinoma n = 57 Bladder carcinoma n = 278 IMA401 target peptide shows high HLA - presentation levels MAGEA4/8 is expressed in multiple cancers Further increase in target presentation by IFN - γ MAGEA4 conventionally used peptide IMA401 target peptide MAGEA4 conventionally used peptide IMA401 target peptide MAGEA4/8 mRNA expression (TPM, log - scaled ) No clinical activity expected Clinical activity shown Potential for clinical activity Data on file: 1 MAGEA4/8 target prevalence by mRNA expression in late - stage solid tumors based on an optimized proprietary targe t expression threshold applied to TCGA data (TCGA stage III/IV); 2 Target peptide density in primary and metastatic solid tumors; median shown (solid line). Target peptide copy numbers per cell ( CpC ) measured by quantitative mass spec in paired samples (MAGEA4 vs. MAGEA4/8 in the same tumor); p - value by paired t - test, 3 CpC fold change in A375 cells presenting MAGEA4 and MAGEA4/8 peptides “ IFN - γ (100 U/mL, 48 h; n=3); p - value by paired t - test; HNSCC, head and neck squamous cell carcinoma; IFN - γ , interferon gamma, sqNSCLC , squamous cell non - small cell lung cancer; TPM, t ranscripts per million . Data cutoff Mar 02, 2026
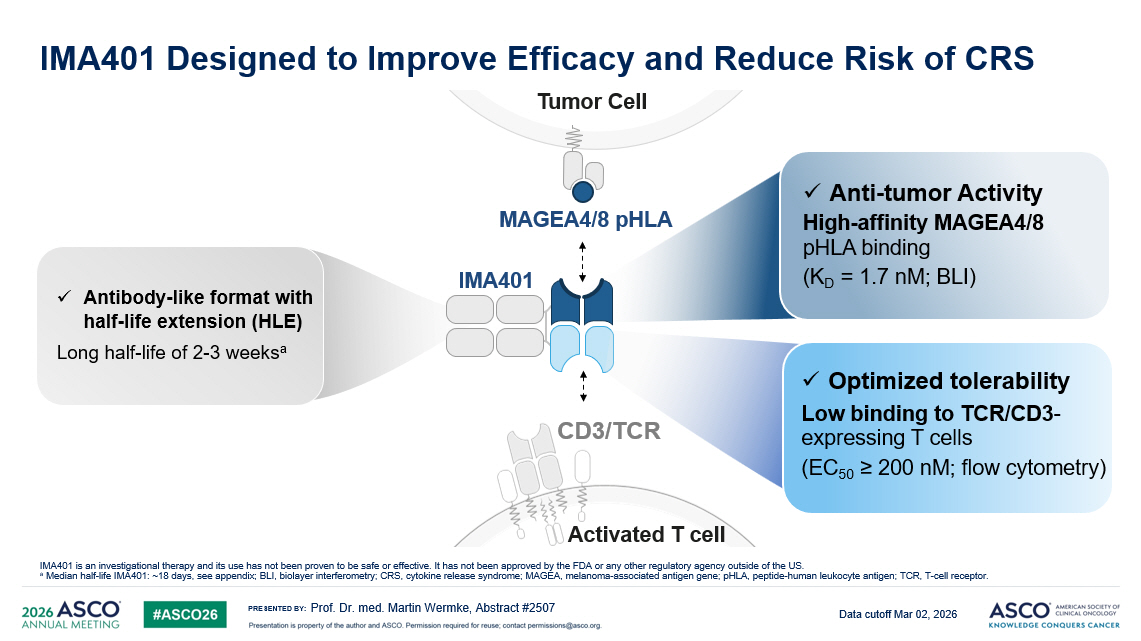
PRESENTED BY: CD3/TCR Activated T cell Tumor Cell MAGEA4/8 pHLA IMA401 x Anti - tumor Activity High - affinity MAGEA4/8 pHLA binding (K D = 1.7 nM ; BLI) x Antibody - like format with half - life extension (HLE) Long half - life of 2 - 3 weeks a x Optimized tolerability Low binding to TCR/CD3 - expressing T cells (EC 50 ≥ 200 nM ; flow cytometry) IMA401 Designed to Improve Efficacy and Reduce Risk of CRS Prof. Dr. med. Martin Wermke, Abstract #2507 IMA401 is an investigational therapy and its use has not been proven to be safe or effective. It has not been approved by the FDA or any other regulatory agency o ut side of the US. a Median half - life IMA401: ~18 days, see appendix; BLI, biolayer interferometry; CRS, cytokine release syndrome; MAGEA, melanoma - associated antigen gene; pHLA , peptide - human leukocyte antigen; TCR, T - cell receptor. Data cutoff Mar 02, 2026
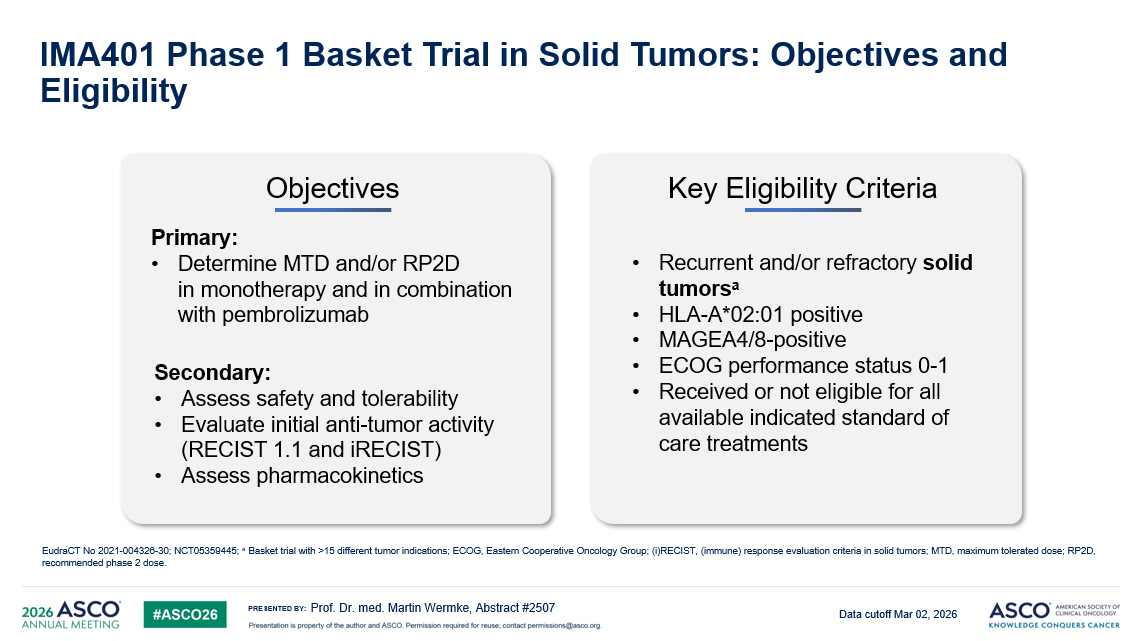
PRESENTED BY: IMA401 Phase 1 Basket Trial in Solid Tumors : Objectives and Eligibility Prof. Dr. med. Martin Wermke, Abstract #2507 Objectives Primary: • Determine MTD and/or RP2D in monotherapy and in combination with pembrolizumab Secondary: • Assess safety and tolerability • Evaluate initial anti - tumor activity (RECIST 1.1 and iRECIST ) • Assess pharmacokinetics Key Eligibility Criteria • Recurrent and/or refractory solid tumors a • HLA - A*02:01 positive • MAGEA4/8 - positive • ECOG performance status 0 - 1 • Received or not eligible for all available indicated standard of care treatments EudraCT No 2021 - 004326 - 30; NCT05359445; a Basket trial with >15 different tumor indications ; ECOG, Eastern Cooperative Oncology Group ; (i)RECIST, ( immune ) response evaluation criteria in solid tumors ; MTD, maximum tolerated dose; RP2D, recommended phase 2 dose. Data cutoff Mar 02, 2026
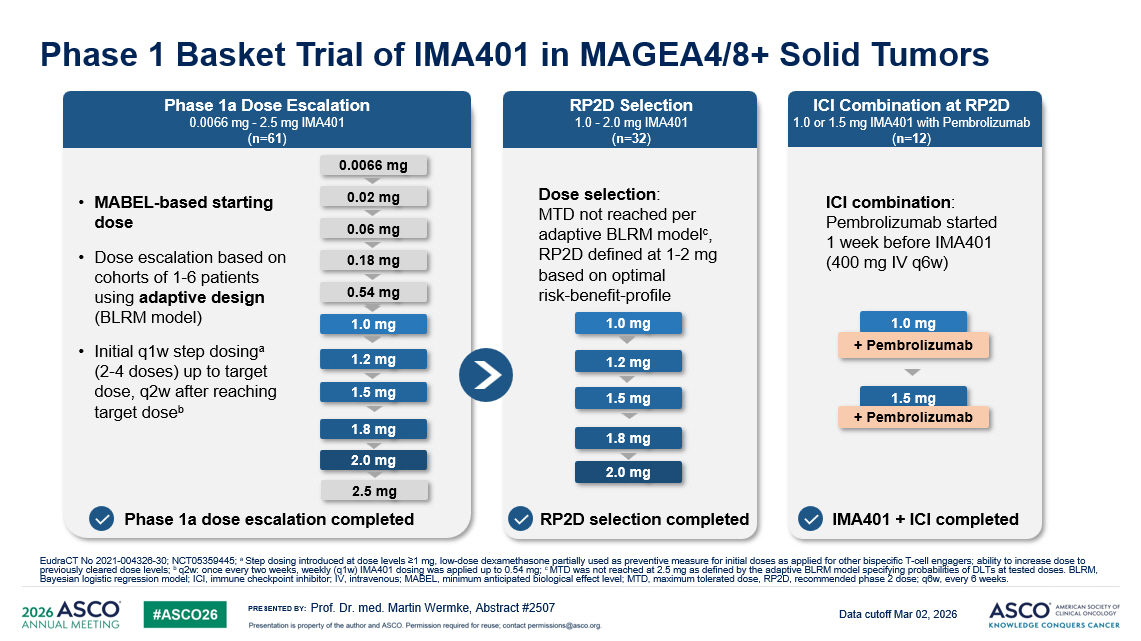
PRESENTED BY: Phase 1 Basket Trial of IMA401 in MAGEA4/8+ Solid Tumors Prof. Dr. med. Martin Wermke, Abstract #2507 0.18 mg 0.54 mg 1.8 mg 0.06 mg 1.2 mg 0.02 mg 0.0066 mg 2.0 mg 1.0 mg 1.5 mg 2.5 mg Phase 1a dose escalation completed 1.8 mg 1.2 mg 2.0 mg 1.0 mg 1.5 mg Dose selection : MTD not reached per adaptive BLRM model c , RP2D defined at 1 - 2 mg based on optimal risk - benefit - profile 1.0 mg 1.5 mg + Pembrolizumab + Pembrolizumab ICI combination : Pembrolizumab started 1 week before IMA401 (400 mg IV q6w) • MABEL - based starting dose • Dose escalation based on cohorts of 1 - 6 patients using adaptive design (BLRM model) • Initial q1w step dosing a (2 - 4 doses) up to target dose, q2w after reaching target dose b Phase 1a Dose Escalation 0.0066 mg - 2.5 mg IMA401 ( n=61 ) RP2D Selection 1.0 - 2.0 mg IMA401 ( n=32 ) ICI Combination at RP2D 1.0 or 1.5 mg IMA401 with Pembrolizumab ( n=12 ) RP2D selection completed IMA401 + ICI completed EudraCT No 2021 - 004326 - 30; NCT05359445; a Step dosing introduced at dose levels ≥1 mg, low - dose dexamethasone partially used as preventive measure for initial doses as ap plied for other bispecific T - cell engagers; ability to increase dose to previously cleared dose levels; b q2w: once every two weeks, weekly (q1w) IMA401 dosing was applied up to 0.54 mg; c MTD was not reached at 2.5 mg as defined by the adaptive BLRM model specifying probabilities of DLTs at tested doses. BLRM, Bayesian logistic regression model; ICI, immune checkpoint inhibitor; IV, intravenous; MABEL, minimum anticipated biological effect level; MTD, maximum tolerated dose, RP2D, recommended phase 2 dose; q6w, every 6 we eks. Data cutoff Mar 02, 2026
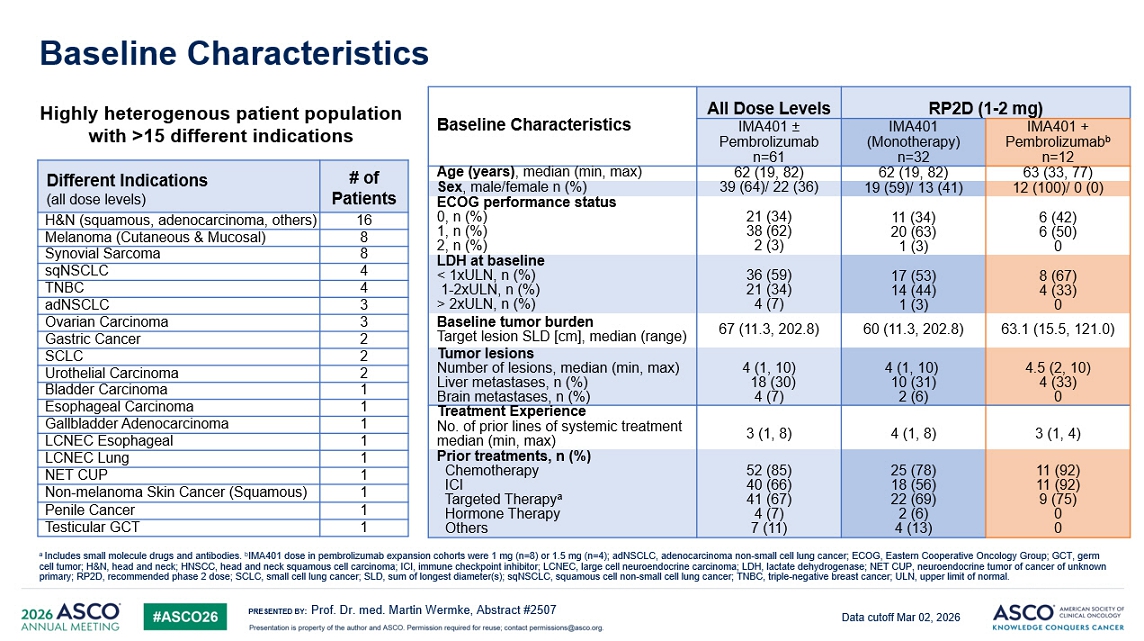
PRESENTED BY: RP2D (1 - 2 mg) All Dose Levels Baseline Characteristics IMA401 + Pembrolizumab b n=12 IMA401 (Monotherapy) n=32 IMA401 ± Pembrolizumab n=61 63 (33, 77) 62 (19, 82) 62 (19, 82) Age (years) , median (min, max) 12 (100)/ 0 (0) 19 (59)/ 13 (41) 39 (64)/ 22 (36) Sex , m ale/female n (%) 6 (42) 6 (50) 0 11 (34) 20 (63) 1 (3) 21 (34) 38 (62) 2 (3) ECOG performance status 0, n (%) 1, n (%) 2, n (%) 8 (67) 4 (33) 0 17 (53) 14 (44) 1 (3) 36 (59) 21 (34) 4 (7) LDH at baseline < 1xULN, n (%) 1 - 2xULN, n (%) > 2xULN, n (%) 63.1 (15.5, 121.0) 60 (11.3, 202.8) 67 (11.3, 202.8) Baseline tumor burden Target lesion SLD [cm], median (range) 4.5 (2, 10) 4 (33) 0 4 (1, 10) 10 (31) 2 (6) 4 (1, 10) 18 (30) 4 (7) Tumor lesions Number of lesions, median (min, max) Liver metastases, n (%) Brain metastases, n (%) Treatment Experience 3 (1, 4) 4 (1, 8) 3 (1, 8) No. of prior lines of systemic treatment median (min, max) 11 (92) 11 (92) 9 (75) 0 0 25 (78) 18 (56) 22 (69) 2 (6) 4 (13) 52 (85) 40 (66) 41 (67) 4 (7) 7 (11) Prior treatments, n (%) Chemotherapy ICI Targeted Therapy a Hormone Therapy Others Highly heterogenous patient population with >15 different indications Baseline Characteristics Prof. Dr. med. Martin Wermke, Abstract #2507 # of Patients Different Indications (all dose levels) 16 H&N (squamous, adenocarcinoma, others) 8 Melanoma (Cutaneous & Mucosal) 8 Synovial Sarcoma 4 sqNSCLC 4 TNBC 3 adNSCLC 3 Ovarian Carcinoma 2 Gastric Cancer 2 SCLC 2 Urothelial Carcinoma 1 Bladder Carcinoma 1 Esophageal Carcinoma 1 Gallbladder Adenocarcinoma 1 LCNEC Esophageal 1 LCNEC Lung 1 NET CUP 1 Non - melanoma Skin Cancer (Squamous) 1 Penile Cancer 1 Testicular GCT a Includes small molecule drugs and antibodies . b IMA401 dose in pembrolizumab expansion cohorts were 1 mg (n=8) or 1.5 mg (n=4); adNSCLC , adenocarcinoma non - small cell lung cancer ; ECOG, Eastern Cooperative Oncology Group; GCT, germ cell tumor; H&N, head and neck ; HNSCC, head and neck squamous cell carcinoma; ICI, immune checkpoint inhibitor ; LCNEC, large cell neuroendocrine carcinoma; LDH, lactate dehydrogenase ; NET CUP, neuroendocrine tumor of cancer of unknown primary ; RP2D, recommended phase 2 dose; SCLC, small cell lung cancer ; SLD, sum of longest diameter(s); sqNSCLC , squamous cell non - small cell lung cancer ; TNBC, triple - negative breast cancer ; ULN, upper limit of normal. Data cutoff Mar 02, 2026
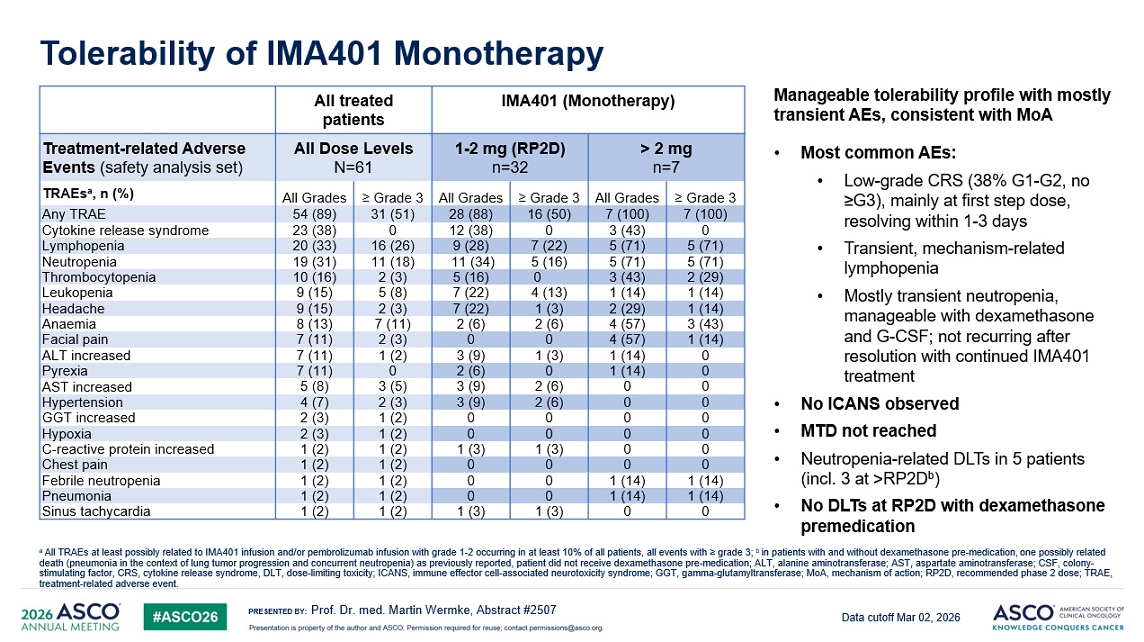
PRESENTED BY: Tolerability of IMA401 Monotherapy Prof. Dr. med. Martin Wermke, Abstract #2507 IMA401 (Monotherapy) A ll treated patients > 2 mg n=7 1 - 2 mg (RP2D) n=32 All Dose Levels N=61 Treatment - related Adverse Events (safety analysis set) ≥ Grade 3 All Grades ≥ Grade 3 All Grades ≥ Grade 3 All Grades TRAEs a , n (%) 7 (100) 7 (100) 16 (50) 28 (88) 31 (51) 54 (89) Any TRAE 0 3 (43) 0 12 (38) 0 23 (38) Cytokine release syndrome 5 (71) 5 (71) 7 (22) 9 (28) 16 (26) 20 (33) Lymphopenia 5 (71) 5 (71) 5 (16) 11 (34) 11 (18) 19 (31) Neutropenia 2 (29) 3 (43) 0 5 (16) 2 (3) 10 (16) Thrombocytopenia 1 (14) 1 (14) 4 (13) 7 (22) 5 (8) 9 (15) Leukopenia 1 (14) 2 (29) 1 (3) 7 (22) 2 (3) 9 (15) Headache 3 (43) 4 (57) 2 (6) 2 (6) 7 (11) 8 (13) Anaemia 1 (14) 4 (57) 0 0 2 (3) 7 (11) Facial pain 0 1 (14) 1 (3) 3 (9) 1 (2) 7 (11) ALT increased 0 1 (14) 0 2 (6) 0 7 (11) Pyrexia 0 0 2 (6) 3 (9) 3 (5) 5 (8) AST increased 0 0 2 (6) 3 (9) 2 (3) 4 (7) Hypertension 0 0 0 0 1 (2) 2 (3) GGT increased 0 0 0 0 1 (2) 2 (3) Hypoxia 0 0 1 (3) 1 (3) 1 (2) 1 (2) C - reactive protein increased 0 0 0 0 1 (2) 1 (2) Chest pain 1 (14) 1 (14) 0 0 1 (2) 1 (2) Febrile neutropenia 1 (14) 1 (14) 0 0 1 (2) 1 (2) Pneumonia 0 0 1 (3) 1 (3) 1 (2) 1 (2) Sinus tachycardia • Most common AEs: • Low - grade CRS (38% G1 - G2, no ≥G3 ), mainly at first step dose, resolving within 1 - 3 days • Transient, mechanism - related lymphopenia • Mostly transient neutropenia, manageable with dexamethasone and G - CSF; not recurring after resolution with continued IMA401 treatment • No ICANS observed • MTD not reached • Neutropenia - related DLTs in 5 patients (incl. 3 at >RP2D b ) • No DLTs at RP2D with dexamethasone premedication Manageable tolerability profile with mostly transient AEs, consistent with MoA a All TRAEs at least possibly related to IMA401 infusion and / or pembrolizumab infusion with grade 1 - 2 occurring in at least 10% of all patients , all events with ≥ grade 3; b in patients with and without dexamethasone pre - medication , one possibly related death (pneumonia in the context of lung tumor progression and concurrent neutropenia) as previously reported , patient did not receive dexamethasone pre - medication ; ALT, a lanine aminotransferase; AST, aspartate aminotransferase; CSF, colony - stimulating factor , CRS, cytokine release syndrome , DLT, dose - limiting toxicity ; ICANS, immune effector cell - associated neurotoxicity syndrome ; GGT, g amma - glutamyltransferase ; MoA , mechanism of action ; RP2D, recommended phase 2 dose; TRAE, treatment - related adverse event . Data cutoff Mar 02, 2026
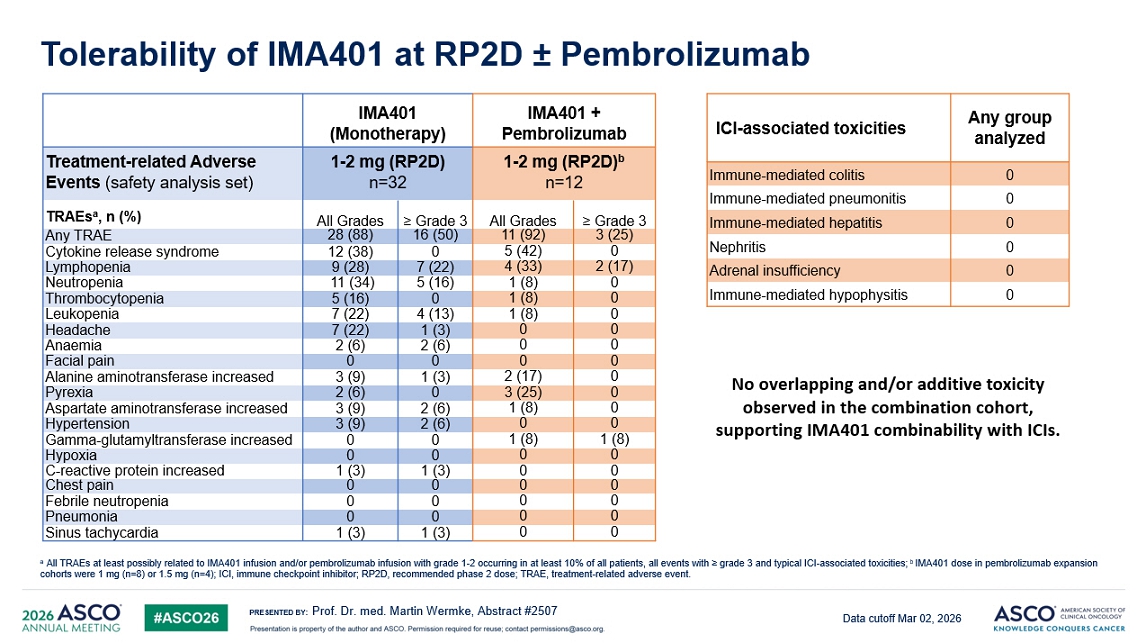
PRESENTED BY: IMA401 + Pembrolizumab IMA401 (Monotherapy) 1 - 2 mg (RP2D) b n=12 1 - 2 mg (RP2D) n=32 Treatment - related Adverse Events (safety analysis set) ≥ Grade 3 All Grades ≥ Grade 3 All Grades TRAEs a , n (%) 3 (25) 11 (92) 16 (50) 28 (88) Any TRAE 0 5 (42) 0 12 (38) Cytokine release syndrome 2 (17) 4 (33) 7 (22) 9 (28) Lymphopenia 0 1 (8) 5 (16) 11 (34) Neutropenia 0 1 (8) 0 5 (16) Thrombocytopenia 0 1 (8) 4 (13) 7 (22) Leukopenia 0 0 1 (3) 7 (22) Headache 0 0 2 (6) 2 (6) Anaemia 0 0 0 0 Facial pain 0 2 (17) 1 (3) 3 (9) Alanine aminotransferase increased 0 3 (25) 0 2 (6) Pyrexia 0 1 (8) 2 (6) 3 (9) Aspartate aminotransferase increased 0 0 2 (6) 3 (9) Hypertension 1 (8) 1 (8) 0 0 Gamma - glutamyltransferase increased 0 0 0 0 Hypoxia 0 0 1 (3) 1 (3) C - reactive protein increased 0 0 0 0 Chest pain 0 0 0 0 Febrile neutropenia 0 0 0 0 Pneumonia 0 0 1 (3) 1 (3) Sinus tachycardia Any group analyzed ICI - associated toxicities 0 Immune - mediated colitis 0 Immune - mediated pneumonitis 0 Immune - mediated hepatitis 0 Nephritis 0 Adrenal insufficiency 0 Immune - mediated hypophysitis No overlapping and/or additive toxicity observed in the combination cohort, supporting IMA401 combinability with ICIs. Tolerability of IMA401 at RP2D “ Pembrolizumab Prof. Dr. med. Martin Wermke, Abstract #2507 a All TRAEs at least possibly related to IMA401 infusion and / or pembrolizumab infusion with grade 1 - 2 occurring in at least 10% of all patients , all events with ≥ grade 3 and typical ICI - associated toxicities ; b IMA401 dose in pembrolizumab expansion cohorts were 1 mg (n=8) or 1.5 mg (n=4); ICI, immune checkpoint inhibitor ; RP2D, recommended phase 2 dose; TRAE, treatment - related adverse event . Data cutoff Mar 02, 2026
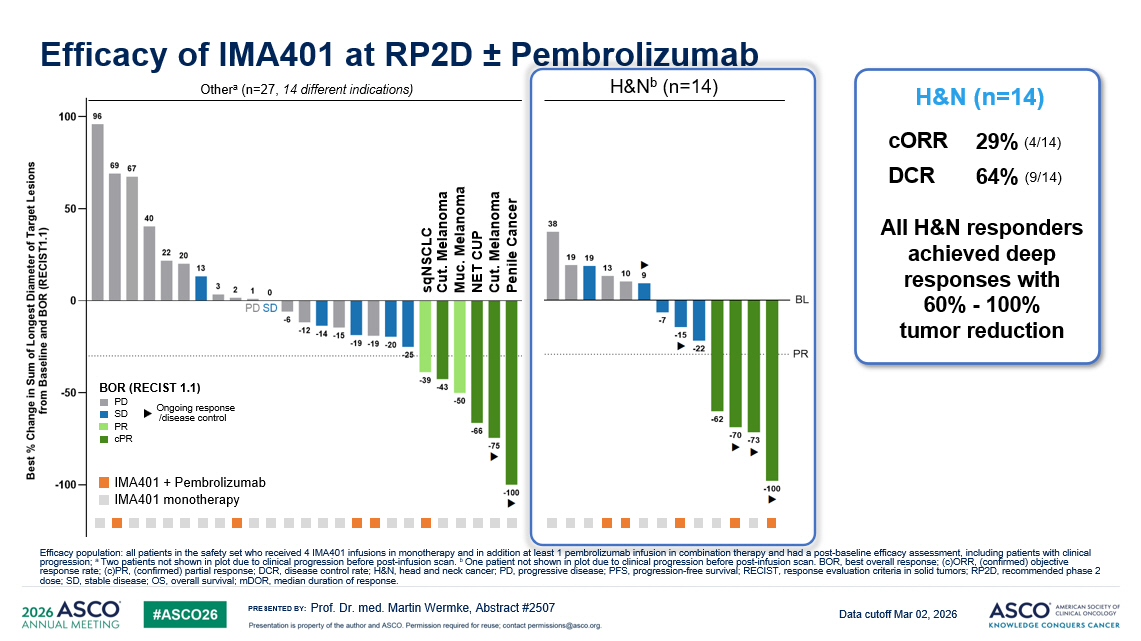
PRESENTED BY: Efficacy of IMA401 at RP2D “ Pembrolizumab Prof. Dr. med. Martin Wermke, Abstract #2507 H&N b ( n= 14) BOR (RECIST 1.1) PD SD PR cPR Ongoing response /disease control Other a (n=27, 14 different indications) IMA401 monotherapy IMA401 + Pembrolizumab 29 % ( 4/14 ) cORR 64% (9/14) DCR H&N (n=14) sqNSCLC Cut. Melanoma Cut. Melanoma Muc . Melanoma NET CUP Penile Cancer All H&N responders achieved deep responses with 60% - 100% tumor reduction Efficacy population: all patients in the safety set who received 4 IMA401 infusions in monotherapy and in addition at least 1 pe mbrolizumab infusion in combination therapy and had a post - baseline efficacy assessment, including patients with clinical progression; a Two patients not shown in plot due to clinical progression before post - infusion scan. b One patient not shown in plot due to clinical progression before post - infusion scan. BOR, best overall response; (c)ORR, (confir med) objective response rate; (c)PR, (confirmed) partial response; DCR, disease control rate; H&N, head and neck cancer; PD, progressive dis eas e; PFS, progression - free survival; RECIST, response evaluation criteria in solid tumors; RP2D, recommended phase 2 dose; SD, stable disease; OS, overall survival; mDOR , median duration of response. Data cutoff Mar 02, 2026
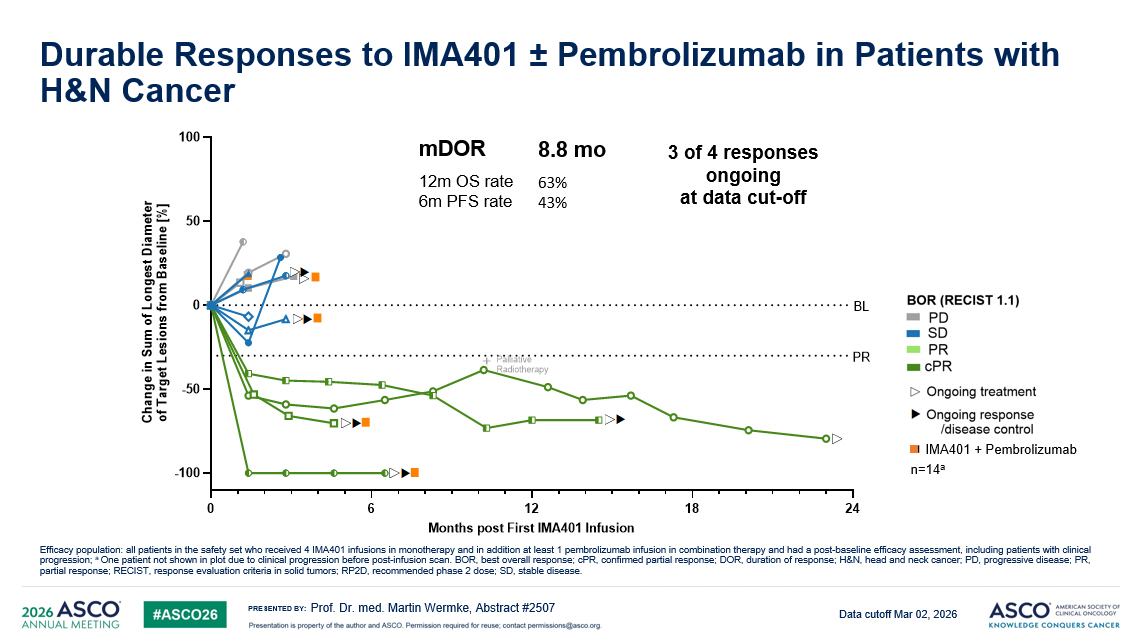
PRESENTED BY: 0 6 12 18 24 -100 -50 0 50 100 Months post First IMA401 Infusion C h a n g e i n S u m o f L o n g e s t D i a m e t e r o f T a r g e t L e s i o n s f r o m B a s e l i n e [ % ] BL PR ⯈ Palliative Radiotherapy + ⯈ ⯈ ⯈ ⯈ Durable Responses to IMA401 “ Pembrolizumab in Patients with H&N Cancer Prof. Dr. med. Martin Wermke, Abstract #2507 Efficacy population: all patients in the safety set who received 4 IMA401 infusions in monotherapy and in addition at least 1 pe mbrolizumab infusion in combination therapy and had a post - baseline efficacy assessment, including patients with clinical progression; a One patient not shown in plot due to clinical progression before post - infusion scan. BOR, best overall response; cPR , confirmed partial response; DOR, duration of response; H&N, head and neck cancer; PD, progressive disease; PR, partial response; RECIST, response evaluation criteria in solid tumors; RP2D, recommended phase 2 dose; SD, stable disease. n=14 a IMA401 + Pembrolizumab 8.8 mo mDOR 63% 43% 12m OS rate 6m PFS rate 3 of 4 responses ongoing at data cut - off Data cutoff Mar 02, 2026
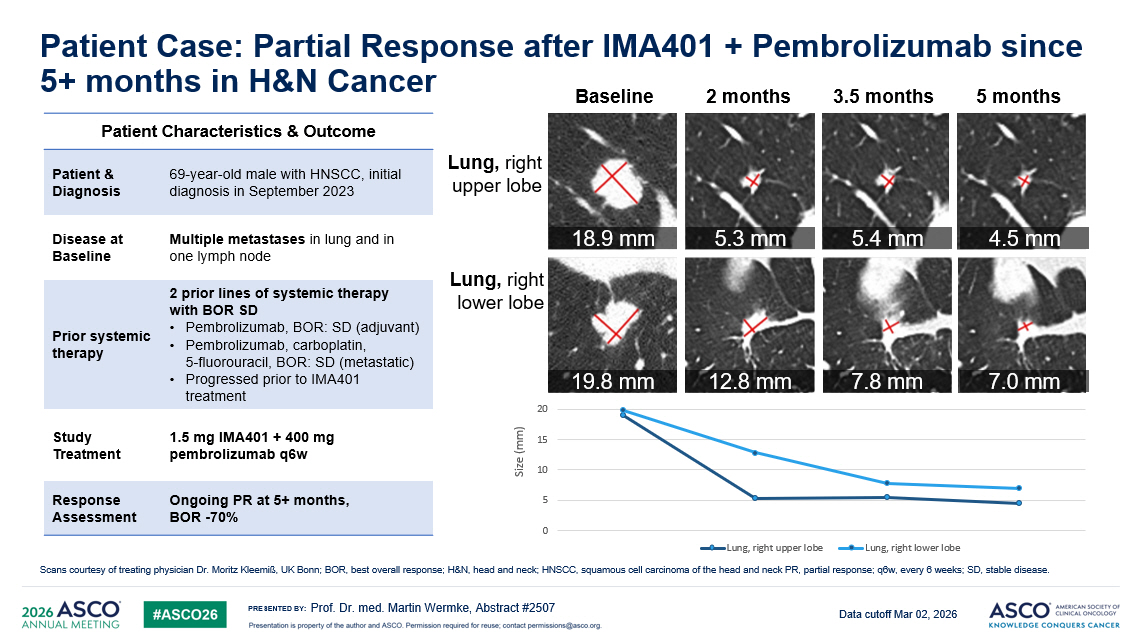
PRESENTED BY: Patient Case: Partial Response after IMA401 + Pembrolizumab since 5+ months in H&N Cancer Prof. Dr. med. Martin Wermke, Abstract #2507 Scans courtesy of treating physician Dr. Moritz Kleemiß , UK Bonn; BOR, best overall response; H&N, head and neck; HNSCC, squamous cell carcinoma of the head and neck PR, partial re spo nse; q6w, every 6 weeks; SD, stable disease. 12 Patient Characteristics & Outcome 69 - year - old male with HNSCC, initial diagnosis in September 2023 Patient & Diagnosis Multiple metastases in lung and in one lymph node Disease at Baseline 2 prior lines of systemic therapy with BOR SD • Pembrolizumab, BOR: SD (adjuvant) • Pembrolizumab, carboplatin, 5 - fluorouracil, BOR: SD (metastatic) • Progressed prior to IMA401 treatment Prior systemic therapy 1.5 mg IMA401 + 400 mg pembrolizumab q6w Study Treatment Ongoing PR at 5+ months, BOR - 70% Response Assessment Lung, right lower lobe 2 months 3.5 months 5 months Baseline Lung, right upper lobe 0 5 10 15 20 Lung, right upper lobe Lung, right lower lobe S ize (mm) 18.9 mm 5.3 mm 5.4 mm 4.5 mm 19.8 mm 12.8 mm 7.8 mm 7.0 mm Data cutoff Mar 02, 2026
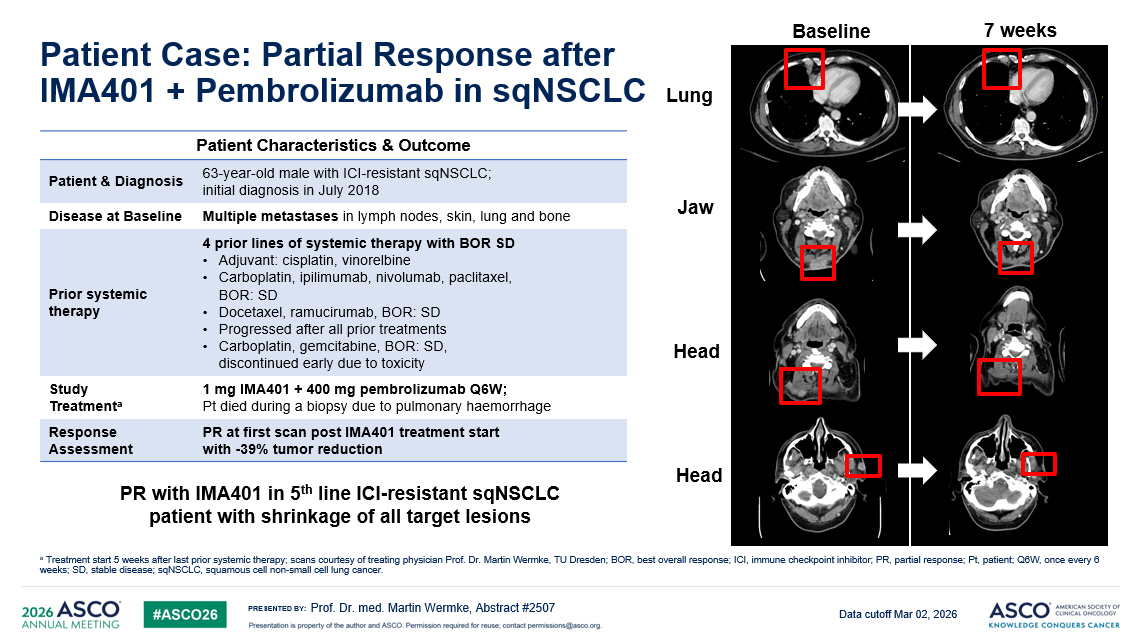
PRESENTED BY: Patient Case: Partial Response after IMA401 + Pembrolizumab in sqNSCLC Prof. Dr. med. Martin Wermke, Abstract #2507 a Treatment start 5 weeks after last prior systemic therapy; scans courtesy of treating physician Prof. Dr. Martin Wermke , TU Dresden; BOR, best overall response; ICI, immune checkpoint inhibitor; PR, partial response; Pt, patient; Q6W, once ever y 6 weeks; SD, stable disease; sqNSCLC , squamous cell non - small cell lung cancer. Lung Baseline 7 weeks Jaw Head Head PR with IMA401 in 5 th line ICI - resistant sqNSCLC patient with shrinkage of all target lesions Patient Characteristics & Outcome 63 - year - old male with ICI - resistant sqNSCLC ; initial diagnosis in July 2018 Patient & Diagnosis Multiple metastases i n lymph nodes, skin, lung and bone Disease at Baseline 4 prior lines of systemic therapy with BOR SD • Adjuvant: cisplatin, vinorelbine • Carboplatin, ipilimumab, nivolumab, paclitaxel, BOR: SD • Docetaxel, ramucirumab, BOR: SD • Progressed after all prior treatments • Carboplatin, gemcitabine, BOR: SD, discontinued early due to toxicity Prior systemic therapy 1 mg IMA401 + 400 mg pembrolizumab Q6W; Pt died during a biopsy due to pulmonary haemorrhage Study Treatment a PR at first scan post IMA401 treatment start with - 39% tumor reduction Response Assessment Data cutoff Mar 02, 2026
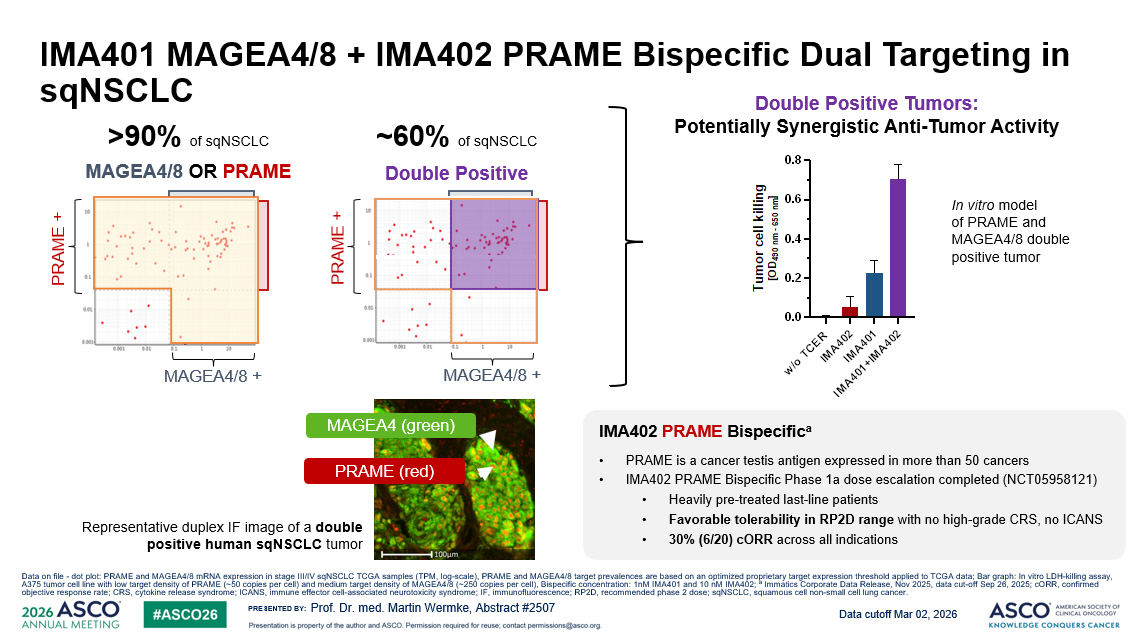
PRESENTED BY: MAGEA4/8 + PRAME + IMA401 MAGEA4/8 + IMA402 PRAME Bispecific Dual Targeting in sqNSCLC Prof. Dr. med. Martin Wermke, Abstract #2507 MAGEA4/8 + PRAME + >90% MAGEA4/8 OR PRAME of sqNSCLC Double Positive ~60% of sqNSCLC Representative duplex IF image of a double positive human sqNSCLC tumor PRAME (red) MAGEA4 (green) In vitro model of PRAME and MAGEA4/8 double positive tumor Double Positive Tumors: Potentially Synergistic Anti - Tumor Activity IMA402 PRAME Bispecific a • PRAME is a cancer testis antigen expressed in more than 50 cancers • IMA402 PRAME Bispecific Phase 1a dose escalation completed ( NCT05958121 ) • Heavily pre - treated last - line patients • Favorable tolerability in RP2D range with no high - grade CRS, no ICANS • 30% (6/20) cORR across all indications Data on file - dot plot: PRAME and MAGEA4/8 mRNA expression in stage III/IV sqNSCLC TCGA samples (TPM, log - scale), PRAME and MAGEA4/8 target prevalences are based on an optimized proprietary target expression th reshold applied to TCGA data; Bar graph: In vitro LDH - killing assay, A375 tumor cell line with low target density of PRAME (~50 copies per cell) and medium target density of MAGEA4/8 (~250 copies per cell) , Bispecific concentration: 1nM IMA401 and 10 nM IMA402; a Immatics Corporate Data Release, Nov 2025, data cut - off Sep 26, 2025; cORR , confirmed objective response rate; CRS, cytokine release syndrome; ICANS, immune effector cell - associated neurotoxicity syndrome; IF, immu nofluorescence; RP2D, recommended phase 2 dose; sqNSCLC , squamous cell non - small cell lung cancer. Data cutoff Mar 02, 2026
PRESENTED BY: Key Takeaways • TCR - based therapies enable immune recognition of intracellular tumor antigens presented by cell - surface HLA, expanding the therapeutic landscape beyond targets accessible to conventional immunotherapies • IMA401 is a novel TCR - based bispecific T - cell engager targeting MAGEA4/8, expressed in multiple cancers incl. head & neck cancer and sqNSCLC • IMA401 demonstrates a manageable tolerability profile and encouraging efficacy as monotherapy or in combination with ICI • Next steps include a combination with a PRAME - directed TCR - based T - cell engager (IMA402) for >90% prevalence in sqNSCLC Prof. Dr. med. Martin Wermke, Abstract #2507 HLA, human leukocyte antigen; head and neck (H&N) cancer (squamous cell and adenocarcinoma); ICI, immune checkpoint inhibitor ; M AGE, melanoma - assicated antigen; PRAME, preferentially expressed in melanoma; sqNSCLC , squamous cell non - small cell lung cancer; TCR: T - cell receptor; Dose escalation data presented by Wermke et al., ESMO 2024. Data cutoff Mar 02, 2026
PRESENTED BY: 16 IMA401 Phase 1 Trial Sponsor: Immatics Thank You – Trial Participants & Caregivers Prof. Dr. med. Martin Wermke, Abstract #2507 University Hospital, Dresden University Hospital Bonn Charité – University Medicine Berlin University Hospital Heidelberg TUM University Hospital Munich Germany University Hospital Würzburg Marien Hospital Düsseldorf University Hospital Münster University Hospital Frankfurt University Medical Center Freiburg University Hospital Regensburg Nuremberg General Hospital University Hospital Erlangen Chemnitz Clinical Centre National Centre for Tumor Diseases, Heidelberg
PRESENTED BY: Appendix Prof. Dr. med. Martin Wermke, Abstract #2507
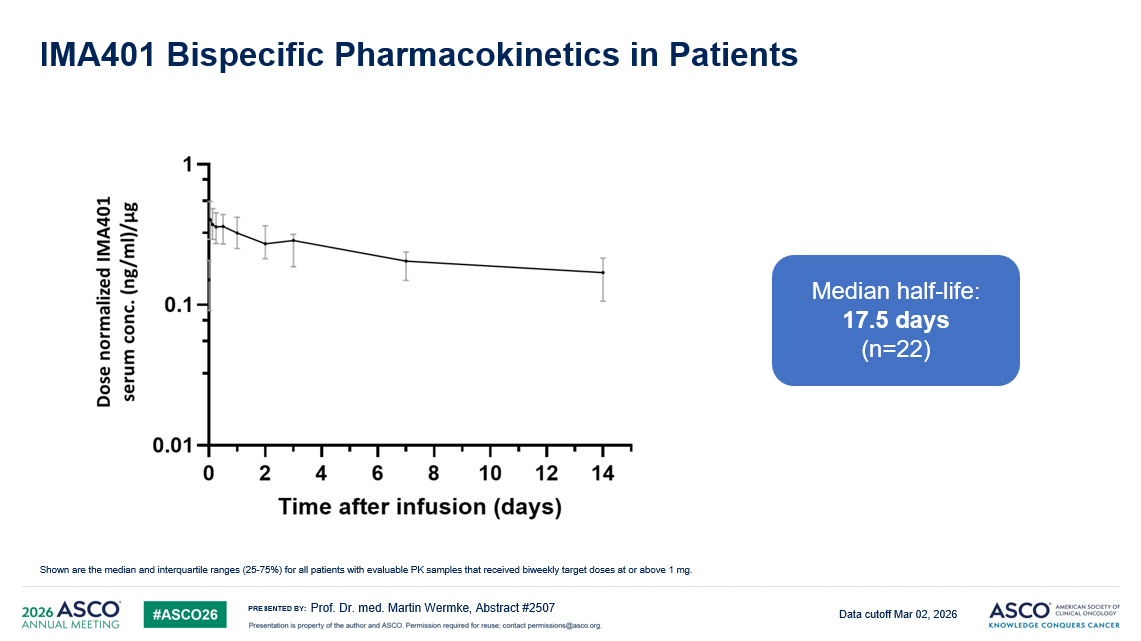
PRESENTED BY: IMA401 Bispecific Pharmacokinetics in Patients Prof. Dr. med. Martin Wermke, Abstract #2507 Shown are the median and interquartile ranges (25 - 75%) for all patients with evaluable PK samples that received biweekly target doses at or above 1 mg. Median half - life: 17.5 days (n=22) Data cutoff Mar 02, 2026
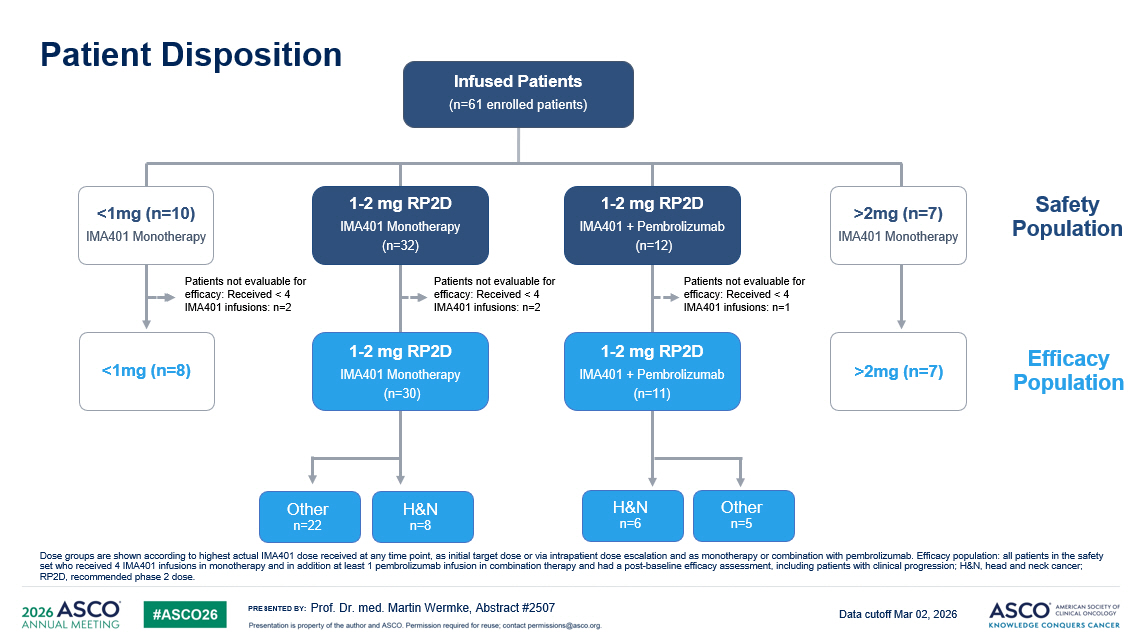
PRESENTED BY: Patient Disposition Prof. Dr. med. Martin Wermke, Abstract #2507 Dose groups are shown according to highest actual IMA401 dose received at any time point, as initial target dose or via intrapatient dose escalation and as monotherapy or combination with pembrolizumab. Efficacy population: all patients in the safety set who received 4 IMA401 infusions in monotherapy and in addition at least 1 pembrolizumab infusion in combination therapy a nd had a post - baseline efficacy assessment, including patients with clinical progression; H&N, head and neck cancer; RP2D, recommended phase 2 dose. Infused Patients (n=61 enrolled patients) 1 - 2 mg RP2D IMA401 Monotherapy (n=32) <1mg (n=8) Patients not evaluable for efficacy: Received < 4 IMA401 infusions: n=2 >2mg (n=7) IMA401 Monotherapy >2mg (n=7) <1mg (n=10) IMA401 Monotherapy 1 - 2 mg RP2D IMA401 + Pembrolizumab (n=12) 1 - 2 mg RP2D IMA401 + Pembrolizumab (n=11) 1 - 2 mg RP2D IMA401 Monotherapy (n=30) H&N n=8 Other n=22 Patients not evaluable for efficacy: Received < 4 IMA401 infusions: n=2 Patients not evaluable for efficacy: Received < 4 IMA401 infusions: n=1 Other n=5 H&N n=6 Safety Population Efficacy Population Data cutoff Mar 02, 2026
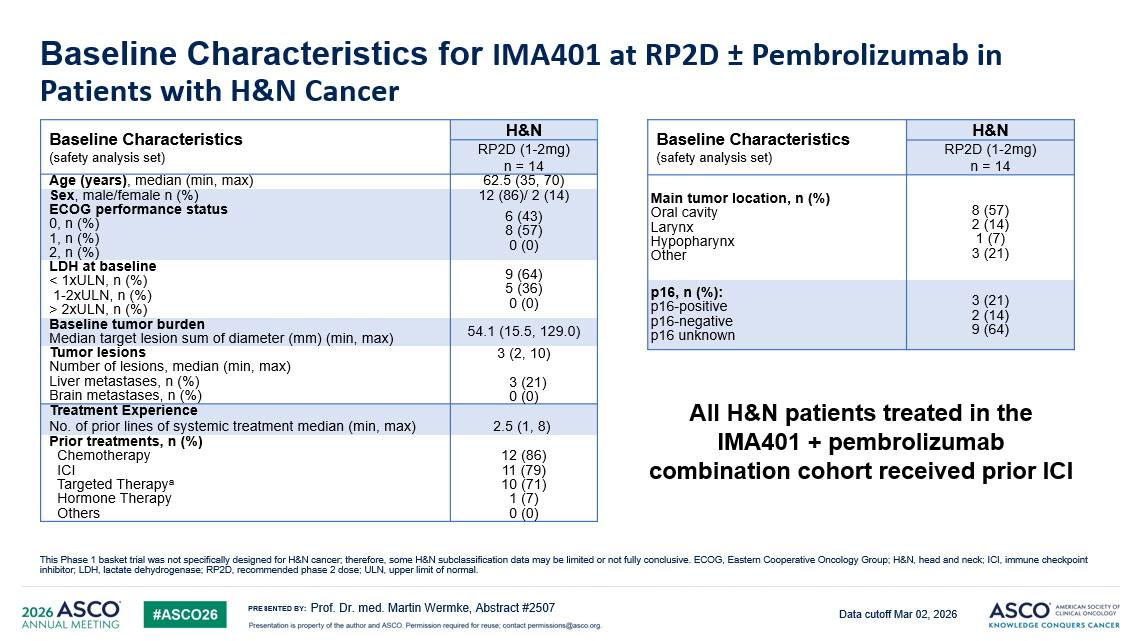
PRESENTED BY: Baseline Characteristics for IMA401 at RP2D ± Pembrolizumab in Patients with H&N Cancer Prof. Dr. med. Martin Wermke, Abstract #2507 This Phase 1 basket trial was not specifically designed for H&N cancer ; therefore , some H&N subclassification data may be limited or not fully conclusive . ECOG, Eastern Cooperative Oncology Group ; H&N, head and neck ; ICI, immune checkpoint inhibitor ; LDH, lactate dehydrogenase ; RP2D, recommended phase 2 dose; ULN, upper limit of normal. H&N Baseline Characteristics (safety analysis set) RP2D (1 - 2mg) n = 14 62.5 (35, 70) Age (years) , median (min, max) 12 (86)/ 2 (14) Sex , m ale/female n (%) 6 (43) 8 (57) 0 (0) ECOG performance status 0, n (%) 1, n (%) 2, n (%) 9 (64) 5 (36) 0 (0) LDH at baseline < 1xULN, n (%) 1 - 2xULN, n (%) > 2xULN, n (%) 54.1 (15.5, 129.0) Baseline tumor burden Median target lesion sum of diameter (mm) (min, max) 3 (2, 10) 3 (21) 0 (0) Tumor lesions Number of lesions, median (min, max) Liver metastases, n (%) Brain metastases, n (%) Treatment Experience 2.5 (1, 8) No. of prior lines of systemic treatment median (min, max) 12 (86) 11 (79) 10 (71) 1 (7) 0 (0) Prior treatments, n (%) Chemotherapy ICI Targeted Therapy a Hormone Therapy Others H&N Baseline Characteristics (safety analysis set) RP2D (1 - 2mg) n = 14 8 (57) 2 (14) 1 (7) 3 (21) Main tumor location, n (%) Oral cavity Larynx Hypopharynx Other 3 (21) 2 (14) 9 (64) p16, n (%): p16 - positive p16 - negative p16 unknown All H&N patients treated in the IMA401 + pembrolizumab combination cohort received prior ICI Data cutoff Mar 02, 2026
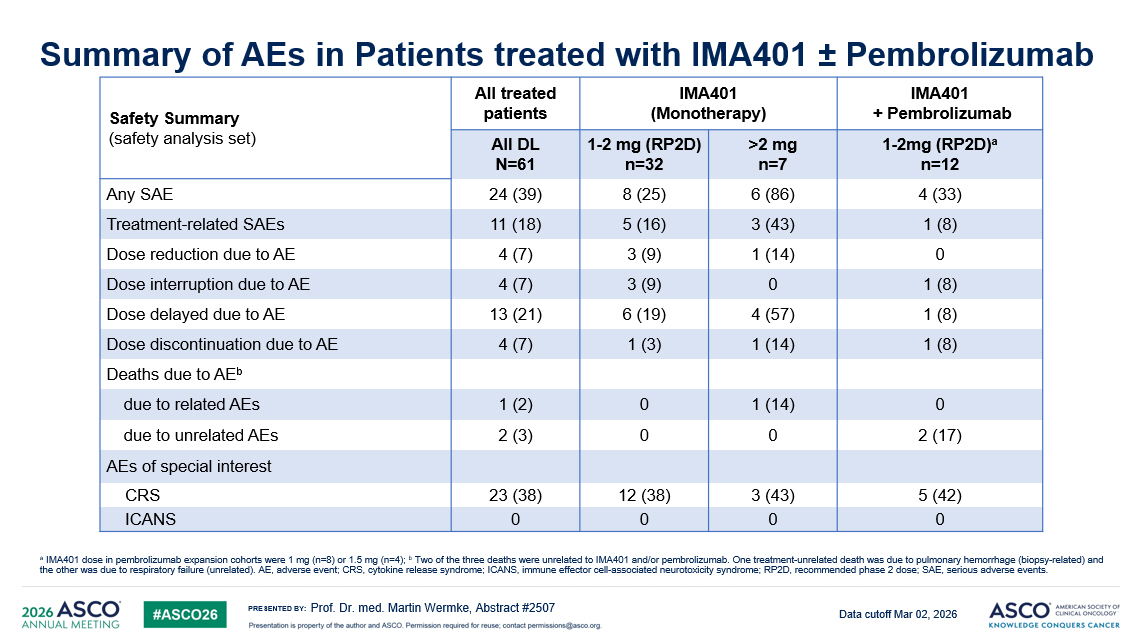
PRESENTED BY: Summary of AEs in Patients treated with IMA401 “ Pembrolizumab Prof. Dr. med. Martin Wermke , Abstract #2507 a IMA401 dose in pembrolizumab expansion cohorts were 1 mg (n=8) or 1.5 mg (n=4); b Two of the three deaths were unrelated to IMA401 and / or pembrolizumab . One treatment - unrelated death was due to pulmonary hemorrhage ( biopsy - related ) and the other was due to respiratory failure ( unrelated ). AE, adverse event ; CRS, cytokine release syndrome ; ICANS, immune effector cell - associated neurotoxicity syndrome ; RP2D, recommended phase 2 dose; SAE, serious adverse events . IMA401 + Pembrolizumab IMA401 (Monotherapy) All treated patients Safety Summary (safety analysis set) 1 - 2mg (RP2D) a n=12 >2 mg n=7 1 - 2 mg (RP2D) n=32 All DL N=61 4 (33) 6 (86) 8 (25) 24 (39) Any SAE 1 (8) 3 (43) 5 (16) 11 (18) Treatment - related SAEs 0 1 (14) 3 (9) 4 (7) Dose reduction due to AE 1 (8) 0 3 (9) 4 (7) Dose interruption due to AE 1 (8) 4 (57) 6 (19) 13 (21) Dose delayed due to AE 1 (8) 1 (14) 1 (3) 4 (7) Dose discontinuation due to AE Deaths due to AE b 0 1 (14) 0 1 (2) due to related AEs 2 (17) 0 0 2 (3) due to unrelated AEs AEs of special interest 5 (42) 3 (43) 12 (38) 23 (38) CRS 0 0 0 0 ICANS Data cutoff Mar 02, 2026
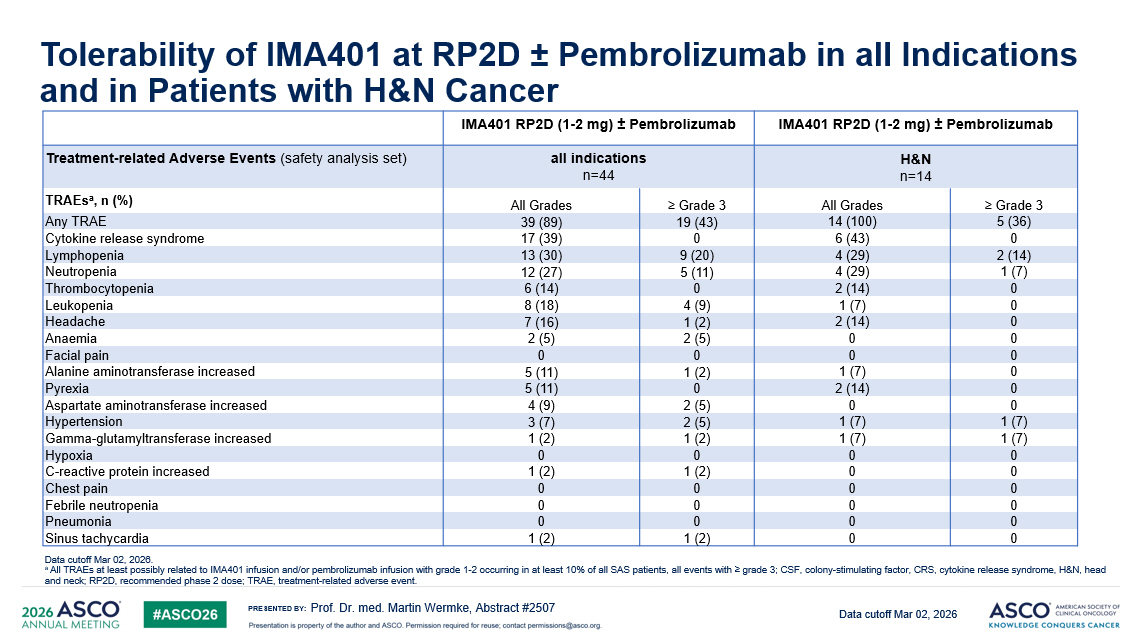
PRESENTED BY: Tolerability of IMA401 at RP2D “ Pembrolizumab in all Indications and in Patients with H&N Cancer IMA401 RP2D (1 - 2 mg) ± Pembrolizumab IMA401 RP2D (1 - 2 mg) ± Pembrolizumab H&N n=14 all indications n=44 Treatment - related Adverse Events (safety analysis set) ≥ Grade 3 All Grades ≥ Grade 3 All Grades TRAEs a , n (%) 5 (36) 14 (100) 19 (43) 39 (89) Any TRAE 0 6 (43) 0 17 (39) Cytokine release syndrome 2 (14) 4 (29) 9 (20) 13 (30) Lymphopenia 1 (7) 4 (29) 5 (11) 12 (27) Neutropenia 0 2 (14) 0 6 (14) Thrombocytopenia 0 1 (7) 4 (9) 8 (18) Leukopenia 0 2 (14) 1 (2) 7 (16) Headache 0 0 2 (5) 2 (5) Anaemia 0 0 0 0 Facial pain 0 1 (7) 1 (2) 5 (11) Alanine aminotransferase increased 0 2 (14) 0 5 (11) Pyrexia 0 0 2 (5) 4 (9) Aspartate aminotransferase increased 1 (7) 1 (7) 2 (5) 3 (7) Hypertension 1 (7) 1 (7) 1 (2) 1 (2) Gamma - glutamyltransferase increased 0 0 0 0 Hypoxia 0 0 1 (2) 1 (2) C - reactive protein increased 0 0 0 0 Chest pain 0 0 0 0 Febrile neutropenia 0 0 0 0 Pneumonia 0 0 1 (2) 1 (2) Sinus tachycardia Data cutoff Mar 02, 2026 . a All TRAEs at least possibly related to IMA401 infusion and/or pembrolizumab infusion with grade 1 - 2 occurring in at least 10% of all SAS patients, all events with ≥ grade 3 ; CSF, colony - stimulating factor, CRS, cytokine release syndrome, H&N, head and neck; RP2D, recommended phase 2 dose; TRAE, treatment - related adverse event. Data cutoff Mar 02, 2026 Prof. Dr. med. Martin Wermke , Abstract #2507
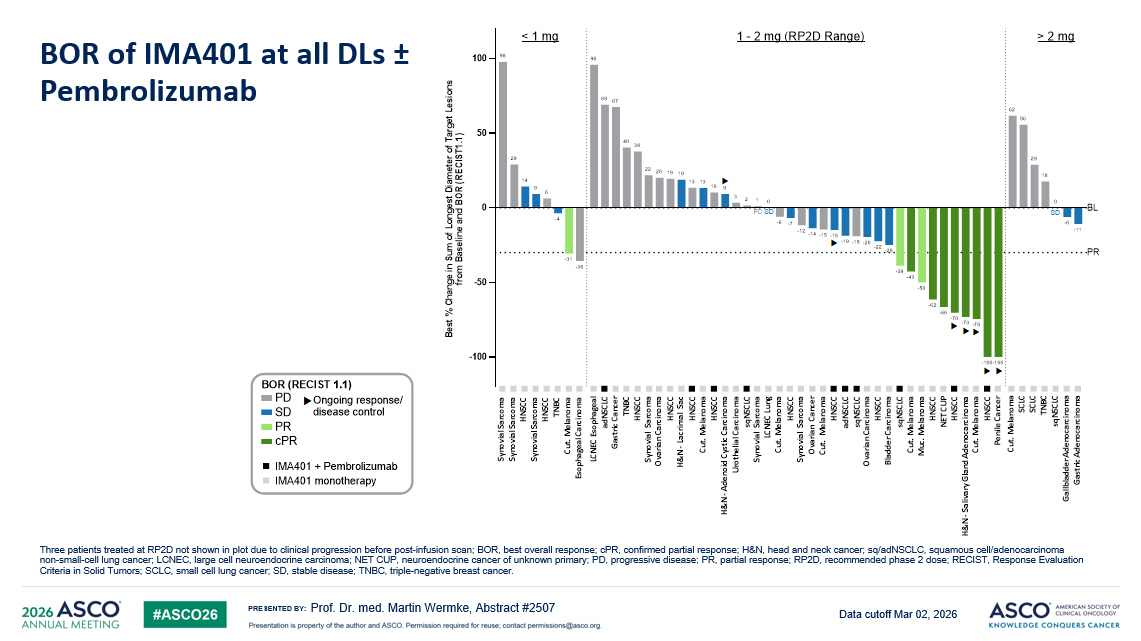
PRESENTED BY: PR -100 -50 0 50 100 -11 -6 0 18 29 56 62 -100-100 -75 -73 -70 -66 -62 -50 -43 -39 -25 -22 -20 -19 -19 -15 -15 -14 -12 -7 -6 0 1 2 3 9 10 13 13 19 19 20 22 38 40 67 69 96 -36 -31 -4 6 9 14 29 98 B e s t % C h a n g e i n S u m o f L o n g e s t D i a m e t e r o f T a r g e t L e s i o n s f r o m B a s e l i n e a n d B O R ( R E C I S T 1 . 1 ) BL ⯈ BOR (RECIST 1.1) Ongoing response/ disease control PD PR cPR SD SD IMA401 + Pembrolizumab ⯈ ⯈ ⯈ < 1 mg 1 - 2 mg (RP2D Range) > 2 mg ⯈ SDPD ⯈ ⯈ ⯈ S y n o v i a l S a r c o m a S y n o v i a l S a r c o m a H N S C C S y n o v i a l S a r c o m a H N S C C T N B C C u t . M e l a n o m a E s o p h a g e a l C a r c i n o m a C u t . M e l a n o m a S C L C S C L C T N B C s q N S C L C G a l l b l a d d e r A d e n o c a r c i n o m a G a s t r i c A d e n o c a r c i n o m a L C N E C E s o p h a g e a l a d N S C L C G a s t r i c C a n c e r T N B C H N S C C S y n o v i a l S a r c o m a O v a r i a n C a r c i n o m a H & N - L a c r i m a l S a c H N S C C H N S C C C u t . M e l a n o m a H N S C C H & N - A d e n o i d C y s t i c C a r c i n o m a U r o t h e l i a l C a r c i n o m a s q N S C L C S y n o v i a l S a r c o m a L C N E C L u n g C u t . M e l a n o m a H N S C C S y n o v i a l S a r c o m a O v a r i a n C a n c e r C u t . M e l a n o m a H N S C C a d N S C L C s q N S C L C O v a r i a n C a r c i n o m a H N S C C B l a d d e r C a r c i n o m a s q N S C L C C u t . M e l a n o m a M u c . M e l a n o m a H N S C C N E T C U P H N S C C H & N - S a l i v a r y G l a n d A d e n o c a r c i n o m a C u t . M e l a n o m a H N S C C P e n i l e C a n c e r IMA401 monotherapy BOR of IMA401 at all DLs ± Pembrolizumab Prof. Dr. med. Martin Wermke, Abstract #2507 Three patients treated at RP2D not shown in plot due to clinical progression before post - infusion scan ; BOR, best overall response; cPR , confirmed partial response; H&N, head and neck cancer ; sq / adNSCLC , squamous cell /adenocarcinoma non - small - cell lung cancer ; LCNEC, large cell neuroendocrine carcinoma; NET CUP, neuroendocrine cancer of unknown primary ; PD, progressive disease ; PR, partial response; RP2D, recommended phase 2 dose; RECIST, Response Evaluation Criteria in Solid Tumors ; SCLC, small cell lung cancer ; SD, stable disease ; TNBC, triple - negative breast cancer . PR -100 -50 0 50 100 -11 -6 0 18 29 56 62 -100-100 -75 -73 -70 -66 -62 -50 -43 -39 -25 -22 -20 -19 -19 -15 -15 -14 -12 -7 -6 0 1 2 3 9 10 13 13 19 19 20 22 38 40 67 69 96 -36 -31 -4 6 9 14 29 98 B e s t % C h a n g e i n S u m o f L o n g e s t D i a m e t e r o f T a r g e t L e s i o n s f r o m B a s e l i n e a n d B O R ( R E C I S T 1 . 1 ) BL ⯈ BOR (RECIST 1.1) Ongoing response/ disease control PD PR cPR SD SD IMA401 + Pembrolizumab ⯈ ⯈ ⯈ < 1 mg 1 - 2 mg (RP2D Range) > 2 mg ⯈ SDPD ⯈ ⯈ ⯈ S y n o v i a l S a r c o m a S y n o v i a l S a r c o m a H N S C C S y n o v i a l S a r c o m a H N S C C T N B C C u t . M e l a n o m a E s o p h a g e a l C a r c i n o m a C u t . M e l a n o m a S C L C S C L C T N B C s q N S C L C G a l l b l a d d e r A d e n o c a r c i n o m a G a s t r i c A d e n o c a r c i n o m a L C N E C E s o p h a g e a l a d N S C L C G a s t r i c C a n c e r T N B C H N S C C S y n o v i a l S a r c o m a O v a r i a n C a r c i n o m a H & N - L a c r i m a l S a c H N S C C H N S C C C u t . M e l a n o m a H N S C C H & N - A d e n o i d C y s t i c C a r c i n o m a U r o t h e l i a l C a r c i n o m a s q N S C L C S y n o v i a l S a r c o m a L C N E C L u n g C u t . M e l a n o m a H N S C C S y n o v i a l S a r c o m a O v a r i a n C a n c e r C u t . M e l a n o m a H N S C C a d N S C L C s q N S C L C O v a r i a n C a r c i n o m a H N S C C B l a d d e r C a r c i n o m a s q N S C L C C u t . M e l a n o m a M u c . M e l a n o m a H N S C C N E T C U P H N S C C H & N - S a l i v a r y G l a n d A d e n o c a r c i n o m a C u t . M e l a n o m a H N S C C P e n i l e C a n c e r IMA401 monotherapy Data cutoff Mar 02, 2026
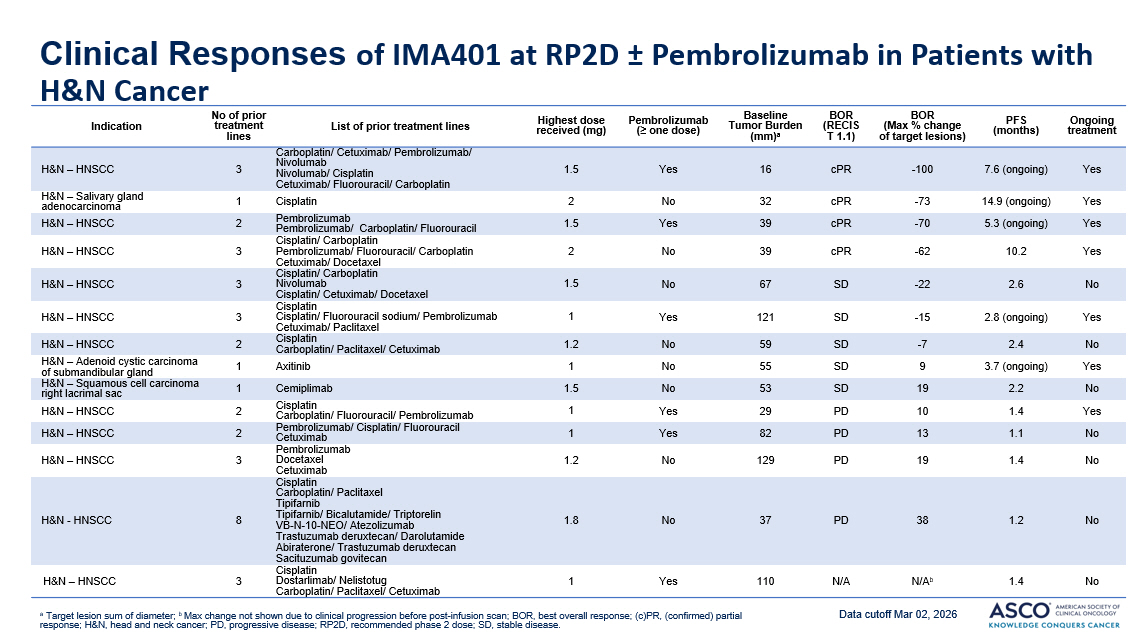
PRESENTED BY: Clinical Responses of IMA401 at RP2D ± Pembrolizumab in Patients with H&N Cancer a Target lesion sum of diameter ; b Max change not shown due to clinical progression before post - infusion scan ; BOR, best overall response; (c)PR, ( confirmed ) partial response; H&N, head and neck cancer ; PD, progressive disease ; RP2D, recommended phase 2 dose; SD, stable disease . Ongoing treatment PFS (months) BOR (Max % change of target lesions) BOR (RECIS T 1.1) Baseline Tumor Burden (mm) a Pembrolizumab (≥ one dose) Highest dose received (mg) List of prior treatment lines No of prior treatment lines Indication Yes 7.6 (ongoing) - 100 cPR 16 Yes 1.5 Carboplatin/ Cetuximab/ Pembrolizumab/ Nivolumab Nivolumab/ Cisplatin Cetuximab/ Fluorouracil/ Carboplatin 3 H&N – HNSCC Yes 14.9 (ongoing) - 73 cPR 32 No 2 Cisplatin 1 H&N – Salivary gland adenocarcinoma Yes 5.3 (ongoing) - 70 cPR 39 Yes 1.5 Pembrolizumab Pembrolizumab/ Carboplatin/ Fluorouracil 2 H&N – HNSCC Yes 10.2 - 6 2 cPR 39 No 2 Cisplatin/ Carboplatin Pembrolizumab/ Fluorouracil/ Carboplatin Cetuximab/ Docetaxel 3 H&N – HNSCC No 2.6 - 22 SD 67 No 1.5 Cisplatin/ Carboplatin Nivolumab Cisplatin/ Cetuximab/ Docetaxel 3 H&N – HNSCC Yes 2.8 (ongoing) - 1 5 SD 121 Yes 1 Cisplatin Cisplatin/ Fluorouracil sodium/ Pembrolizumab Cetuximab/ Paclitaxel 3 H&N – HNSCC No 2.4 - 7 SD 59 No 1 . 2 Cisplatin Carboplatin/ Paclitaxel/ Cetuximab 2 H&N – HNSCC Yes 3.7 (ongoing) 9 SD 55 No 1 Axitinib 1 H&N – Adenoid cystic carcinoma of submandibular gland No 2.2 19 SD 53 No 1.5 Cemiplimab 1 H&N – Squamous cell carcinoma right lacrimal sac Yes 1.4 10 PD 29 Yes 1 Cisplatin Carboplatin/ Fluorouracil/ Pembrolizumab 2 H&N – HNSCC No 1.1 13 PD 82 Yes 1 Pembrolizumab/ Cisplatin/ Fluorouracil Cetuximab 2 H&N – HNSCC No 1.4 19 PD 129 No 1.2 Pembrolizumab Docetaxel Cetuximab 3 H&N – HNSCC No 1.2 38 PD 37 No 1.8 Cisplatin Carboplatin/ Paclitaxel Tipifarnib Tipifarnib/ Bicalutamide/ Triptorelin VB - N - 10 - NEO/ Atezolizumab Trastuzumab deruxtecan/ Darolutamide Abiraterone/ Trastuzumab deruxtecan Sacituzumab govitecan 8 H&N - HNSCC No 1.4 N/A b N/A 110 Yes 1 Cisplatin Dostarlimab / Nelistotug Carboplatin/ Paclitaxel/ Cetuximab 3 H&N – HNSCC Data cutoff Mar 02, 2026
PRESENTED BY: Thank you Prof. Dr. med. Martin Wermke, Abstract #2507