.7
PRESENTED BY: Patient - level Clinical Response Dynamics in Advanced Melanoma With Anzu - cel, a PRAME - targeted TCR T - cell Therapy Diwakar Davar 1 , Sapna Pradyuman Patel 2 , Leonel Fernando Hernandez - Aya 3 , Tobias Albert Wilhelm Holderried 4 , Antonia Busse 5 , Apostolia Maria Tsimberidou 6 , Dejka M. Araujo 6 , Manik Chatterjee 7,8 , Winfried Alsdorf 9 , Silvana Hengler 10 , M. Alper Kursunel 10 , Delfi Krishna 11 , Dmitry Pankov 11 , Cedrik Michael Britten 10 , Martin Wermke 12 ¹University of Pittsburgh Medical Center (UPMC), Hillman Cancer Center, Pittsburgh,PA ; 2 UCHealth, University of Colorado Hospital, Aurora, CO; 3 University of Miami, Miami, FL; 4 University Hospital Bonn, Bonn, Germany; 5 Charite Medical University Hospital, Berlin, Germany; 6 The University of Texas MD Anderson Cancer Center, Houston, TX; 7 Translational Oncology /Early Clinical Trial Unit (ECTU), Comprehensive Cancer Center Mainfranken; 8 University Hospital Würzburg, Würzburg, Germany; 9 Department of Hematology and Oncology University Hospital Hamburg Eppendorf, Hamburg, Germany; 10 Immatics Biotechnologies GmbH, Tuebingen, Germany; 11 Immatics US, Inc., Houston, TX, USA; 12 University Hospital Carl Gustav Carus, Dresden, Germany Diwakar Davar M.D., Abstract #9508
PRESENTED BY: Key Takeaways • TCR - based therapies enable immune recognition of intracellular tumor antigens presented by cell - surface HLA, expanding the therapeutic landscape beyond targets accessible to conventional immunotherapies • Anzutresgene autoleucel ( anzu - cel, IMA203) is a one - time autologous TCR T - cell therapy targeting the cancer - associated antigen PRAME, which is expressed in >50 cancers and represents a novel immunotherapy target for melanoma • Anzu - cel demonstrates a predictable and manageable tolerability profile and rapid, deep, and durable systemic antitumor activity in settings of high unmet need: metastatic PD - 1 - relapsed melanoma and metastatic uveal melanoma • Exploratory response analysis supports the hypothesis that the broad systemic reach of anzu - cel can sustain disease control across multiple metastatic sites • Findings support continued development of anzu - cel in melanoma, including the randomized Phase 3 SUPRAME trial (NCT06743126) Diwakar Davar M.D., Abstract #9508 Anzu - cel, anzutresgene autoleucel ; HLA, human leukocyte antigen; PRAME, preferentially expressed antigen in melanoma; TCR, T - cell receptor.
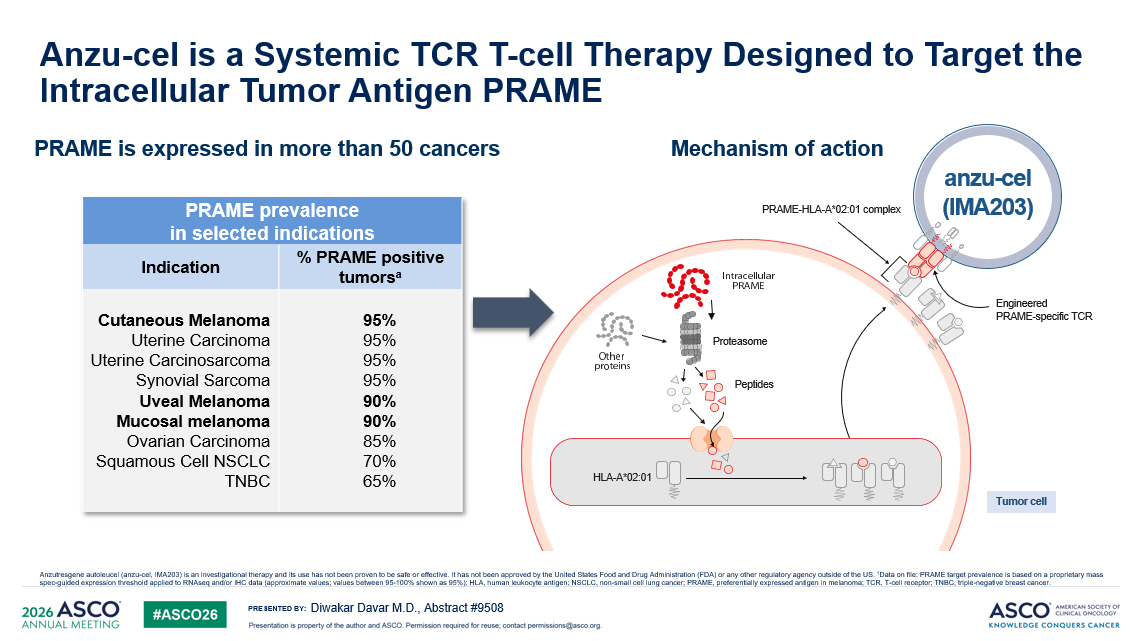
PRESENTED BY: Anzu - cel is a Systemic TCR T - cell Therapy Designed to Target the Intracellular Tumor Antigen PRAME Diwakar Davar M.D., Abstract #9508 Anzutresgene autoleucel (anzu - cel, IMA203) is an investigational therapy and its use has not been proven to be safe or effective . It has not been approved by the United States Food and Drug Administration (FDA) or any other regulatory agency outside of the US. 1 Data on file: PRAME target prevalence is based on a proprietary mass spec - guided expression threshold applied to RNAseq and/or IHC data (approximate values; values between 95 - 100% shown as 95%); HL A, human leukocyte antigen; NSCLC, non - small cell lung cancer; PRAME, preferentially expressed antigen in melanoma ; TCR, T - cell receptor; TNBC, triple - negative breast cancer. PRAME is expressed in more than 50 cancers Mechanism of action anzu - cel (IMA203) PRAME - HLA - A*02:01 complex Proteasome Peptides HLA - A*02:01 Tumor cell Engineered PRAME - specific TCR PRAME prevalence in selected indications % PRAME positive tumors a Indication 95% 95% 95% 95% 90% 90% 85% 70% 65% Cutaneous Melanoma Uterine Carcinoma Uterine Carcinosarcoma Synovial Sarcoma Uveal Melanoma Mucosal melanoma Ovarian Carcinoma Squamous Cell NSCLC TNBC
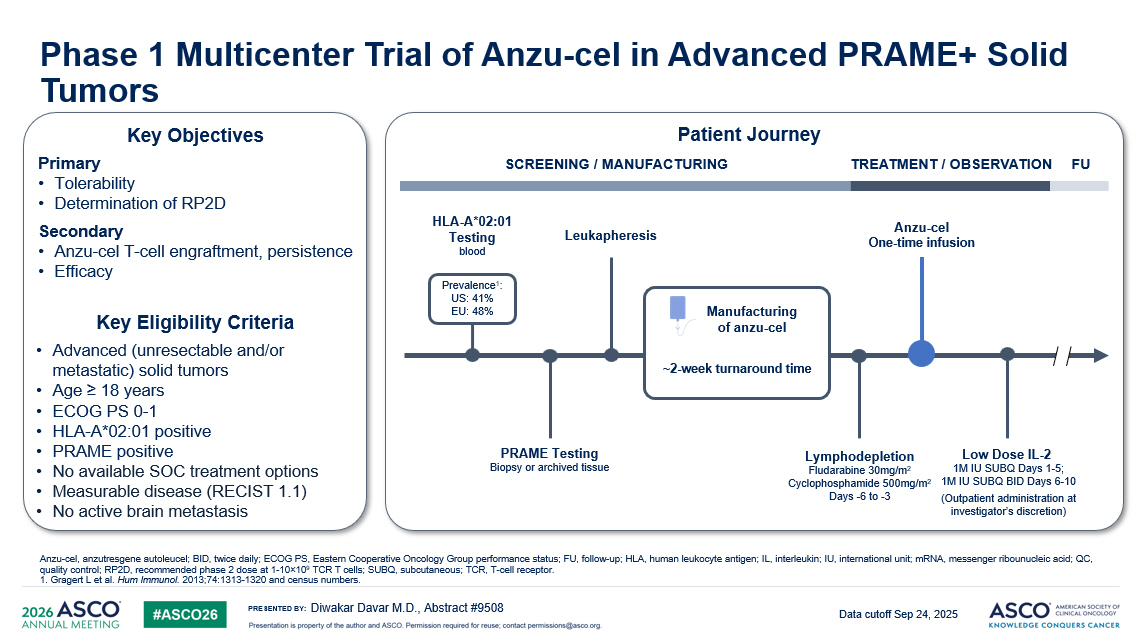
PRESENTED BY: Phase 1 Multicenter Trial of Anzu - cel in Advanced PRAME+ Solid Tumors Diwakar Davar M.D., Abstract #9508 Anzu - cel, a nzutresgene autoleucel ; BID, twice daily; ECOG PS, Eastern Cooperative Oncology Group performance status; FU, follow - up; HLA, human leukocyte antigen; I L, interleukin; IU, international unit; mRNA, messenger ribounucleic acid; QC, quality control; RP2D, recommended phase 2 dose at 1 - 10 î 10 9 TCR T cells; SUBQ, subcutaneous; TCR, T - cell receptor . 1. Gragert L et al. Hum Immunol. 2013;74:1313 - 1320 and census numbers. Data cutoff Sep 24, 2025 Key Objectives Primary • Tolerability • Determination of RP2D Secondary • Anzu - cel T - cell engraftment, persistence • Efficacy Key Eligibility Criteria • Advanced (unresectable and/or metastatic) solid tumors • Age ≥ 18 years • ECOG PS 0 - 1 • HLA - A*02:01 positive • PRAME positive • No available SOC treatment options • Measurable disease (RECIST 1.1) • No active brain metastasis SCREENING / MANUFACTURING Leukapheresis Anzu - cel One - time infusion Lymphodepletion Fludarabine 30mg/m 2 Cyclophosphamide 500mg/m 2 Days - 6 to - 3 Low Dose IL - 2 1M IU SUBQ Days 1 - 5; 1M IU SUBQ BID Days 6 - 10 (Outpatient administration at investigator’s discretion) PRAME Testing Biopsy or archived tissue TREATMENT / OBSERVATION FU HLA - A*02:01 Testing blood Prevalence 1 : US: 41% EU: 48% Manufacturing of anzu - cel ~2 - week turnaround time Patient Journey
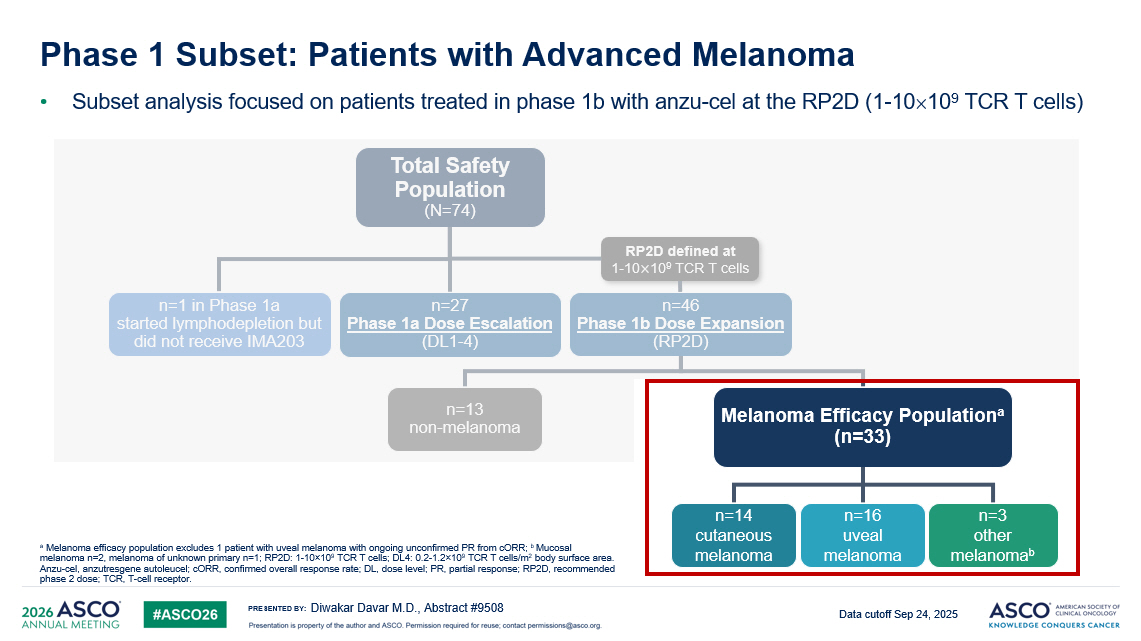
PRESENTED BY: Phase 1 Subset: Patients with Advanced Melanoma • Subset analysis focused on patients treated in phase 1b with anzu - cel at the RP2D (1 - 10 10 9 TCR T cells) Diwakar Davar M.D., Abstract #9508 a Melanoma efficacy population excludes 1 patient with uveal melanoma with ongoing unconfirmed PR from cORR ; b Mucosal melanoma n=2, melanoma of unknown primary n=1; RP2D: 1 - 10 î 10 9 TCR T cells; DL4: 0.2 - 1.2 î 10 9 TCR T cells/m 2 body surface area. Anzu - cel, a nzutresgene autoleucel ; cORR , confirmed overall response rate; DL, dose level; PR, partial response; RP2D, recommended phase 2 dose; TCR, T - cell receptor . Data cutoff Sep 24, 2025 Total Safety Population (N=74) Melanoma Efficacy Population a (n=33) n=13 non - melanoma n=3 o ther melanoma b n=14 cutaneous melanoma n=16 u veal melanoma n=27 Phase 1a Dose Escalation (DL1 - 4) n=1 in Phase 1a started lymphodepletion but did not receive IMA203 n=46 Phase 1b Dose Expansion (RP2D) RP2D defined at 1 - 10 ൈ 10 9 TCR T cells
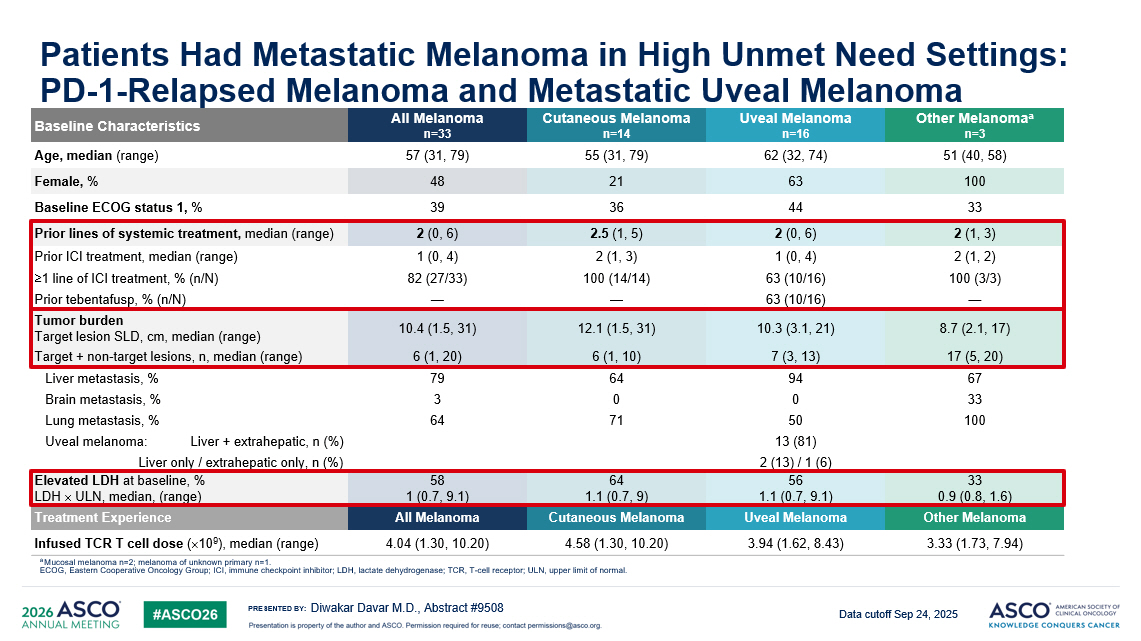
PRESENTED BY: Patients Had Metastatic Melanoma in High Unmet Need Settings: PD - 1 - Relapsed Melanoma and Metastatic Uveal Melanoma Diwakar Davar M.D., Abstract #9508 a Mucosal melanoma n=2; melanoma of unknown primary n=1. ECOG, Eastern Cooperative Oncology Group; ICI, immune checkpoint inhibitor; LDH, lactate dehydrogenase; TCR, T - cell receptor; UL N, upper limit of normal. Data cutoff Sep 24, 2025 Other Melanoma a n=3 Uveal Melanoma n=16 Cutaneous Melanoma n=14 All Melanoma n=33 Baseline Characteristics 51 (40, 58) 62 (32, 74) 55 (31, 79) 57 (31, 79) Age, median (range) 100 63 21 48 Female, % 33 44 36 39 Baseline ECOG status 1, % 2 (1, 3) 2 (0, 6) 2.5 (1, 5) 2 (0, 6) Prior lines of systemic treatment, median ( range) 2 (1, 2) 1 (0, 4) 2 (1, 3) 1 (0, 4) Prior ICI treatment, median (range) 100 (3/3) 63 (10/16) 100 (14/14) 82 (27/33) ≥1 line of ICI treatment, % (n/N) — 63 (10/16) — — Prior tebentafusp , % (n/N) 8.7 (2.1, 17) 10.3 (3.1, 21) 12.1 (1.5, 31) 10.4 (1.5, 31) Tumor burden Target lesion SLD, cm, median (range) 17 (5, 20) 7 (3, 13) 6 (1, 10) 6 (1, 20) Target + non - target lesions, n, median (range) 67 94 64 79 Liver metastasis, % 33 0 0 3 Brain metastasis, % 100 50 71 64 Lung metastasis, % 13 (81) Uveal melanoma: Liver + extrahepatic, n (%) 2 (13) / 1 (6) Liver only / extrahepatic only, n (%) 33 0.9 (0.8, 1.6) 56 1.1 (0.7, 9.1) 64 1.1 (0.7, 9) 58 1 (0.7, 9.1) Elevated LDH at baseline, % LDH ULN, median, (range) Other Melanoma Uveal Melanoma Cutaneous Melanoma All Melanoma Treatment Experience 3.33 (1.73, 7.94) 3.94 (1.62, 8.43) 4.58 (1.30, 10.20) 4.04 (1.30, 10.20) Infused TCR T cell dose ( 10 9 ), median (range)
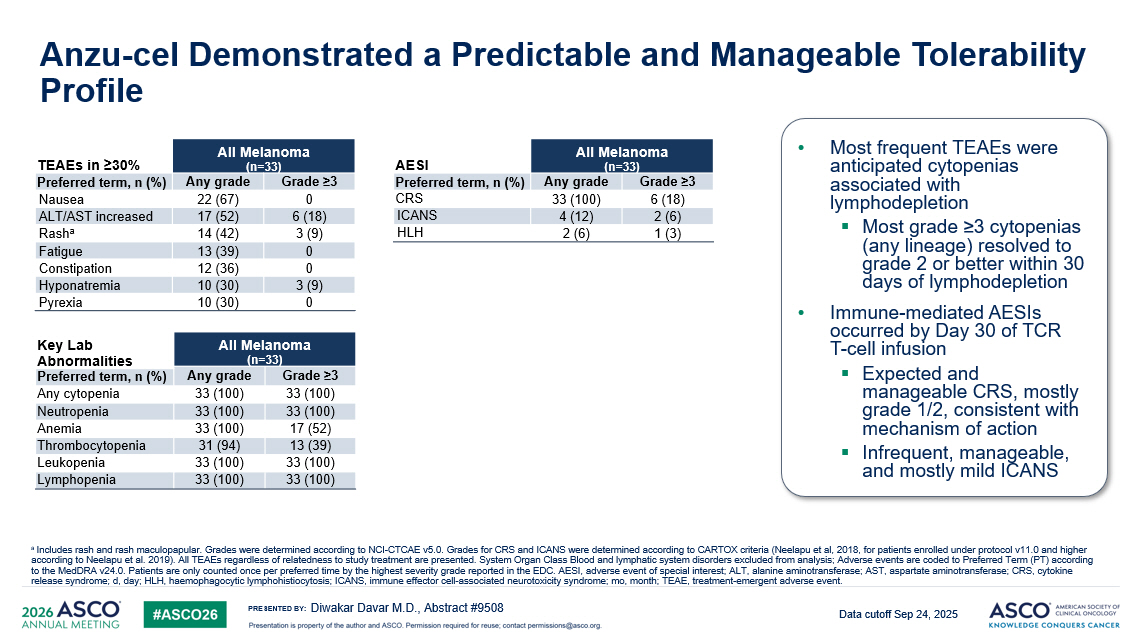
PRESENTED BY: Anzu - cel Demonstrated a Predictable and Manageable Tolerability Profile • Most frequent TEAEs were anticipated cytopenias associated with lymphodepletion ▪ Most grade ≥3 cytopenias (any lineage) resolved to grade 2 or better within 30 days of lymphodepletion • Immune - mediated AESIs occurred by Day 30 of TCR T - cell infusion ▪ Expected and manageable CRS, mostly grade 1/2, consistent with mechanism of action ▪ Infrequent, manageable, and mostly mild ICANS Diwakar Davar M.D., Abstract #9508 a Includes rash and rash maculopapular. Grades were determined according to NCI - CTCAE v5.0. Grades for CRS and ICANS were determin ed according to CARTOX criteria ( Neelapu et al, 2018, for patients enrolled under protocol v11.0 and higher according to Neelapu et al. 2019). All TEAEs regardless of relatedness to study treatment are presented. System Organ Class Blood and lymphatic sy st em disorders excluded from analysis; Adverse events are coded to Preferred Term (PT) according to the MedDRA v24.0. Patients are only counted once per preferred time by the highest severity grade reported in the EDC. AES I, adverse event of special interest; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRS, cytokine release syndrome; d, day; HLH, haemophagocytic lymphohistiocytosis; ICANS, immune effector cell - associated neurotoxicity syndrome; mo , month; TEAE, treatment - emergent adverse event. All Melanoma ( n =33) TEAEs in ≥30% Grade ≥3 Any grade Preferred term, n (%) 0 22 (67) Nausea 6 (18) 17 (52) ALT/AST increased 3 (9) 14 (42) Rash a 0 13 (39) Fatigue 0 12 (36) Constipation 3 (9) 10 (30) Hyponatremia 0 10 (30) Pyrexia All Melanoma (n=33) AESI Grade ≥3 Any grade Preferred term, n (%) 6 (18) 33 (100) CRS 2 (6) 4 (12) ICANS 1 (3) 2 (6) HLH All Melanoma (n=33) Key Lab Abnormalities Grade ≥3 Any grade Preferred term, n (%) 33 (100) 33 (100) Any cytopenia 33 (100) 33 (100) Neutropenia 17 (52) 33 (100) Anemia 13 (39) 31 (94) Thrombocytopenia 3 3 (100) 33 (100) Leukopenia 33 (100) 33 (100) Lymphopenia Data cutoff Sep 24, 2025
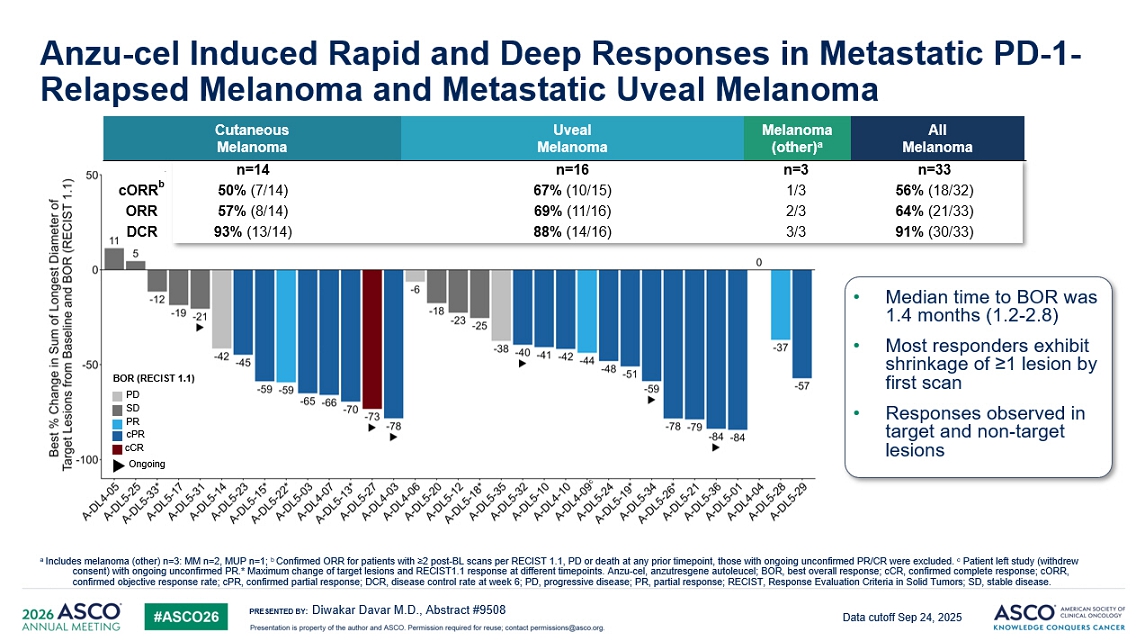
PRESENTED BY: Anzu - cel Induced Rapid and Deep Responses in Metastatic PD - 1 - Relapsed Melanoma and Metastatic Uveal Melanoma Diwakar Davar M.D., Abstract #9508 a Includes melanoma (other) n=3: MM n=2, MUP n=1; b Exploratory analysis of confirmed ORR for patients with ≥2 post - BL scans per RECIST 1.1, PD or death at any prior timepoint, tho se with ongoing unconfirmed PR/CR were excluded. c Patient left study (withdrew consent) with ongoing unconfirmed PR.* Maximum change of target lesions and RECIST1.1 response at different t ime points. Anzu - cel, a nzutresgene autoleucel ; BOR, best overall response; cCR , confirmed complete response; cORR , confirmed objective response rate; cPR , confirmed partial response; DCR, disease control rate at week 6; PD, progressive disease; PR, partial response; RECIST, Res pon se Evaluation Criteria in Solid Tumors; SD, stable disease. n=33 n=3 n=16 n=14 6 4 % (21/33) 2/3 6 9 % (11/16) 57% (8/14) ORR 5 6 % (18/3 2 ) 1/3 6 7 % (10/15) 5 0 % (7/1 4 ) cORR b 91% (30/33) 3/3 8 8 % (14/16) 9 3 % (13/14) DCR Cutaneous Melanoma Uveal Melanoma Melanoma (other) a All Melanoma • Median time to BOR was 1.4 months (1.2 - 2.8) • Most responders exhibit shrinkage of ≥1 lesion by first scan • Responses observed in target and non - target lesions Data cutoff Sep 24, 2025 BOR (RECIST 1.1) PD SD PR cPR cCR Ongoing
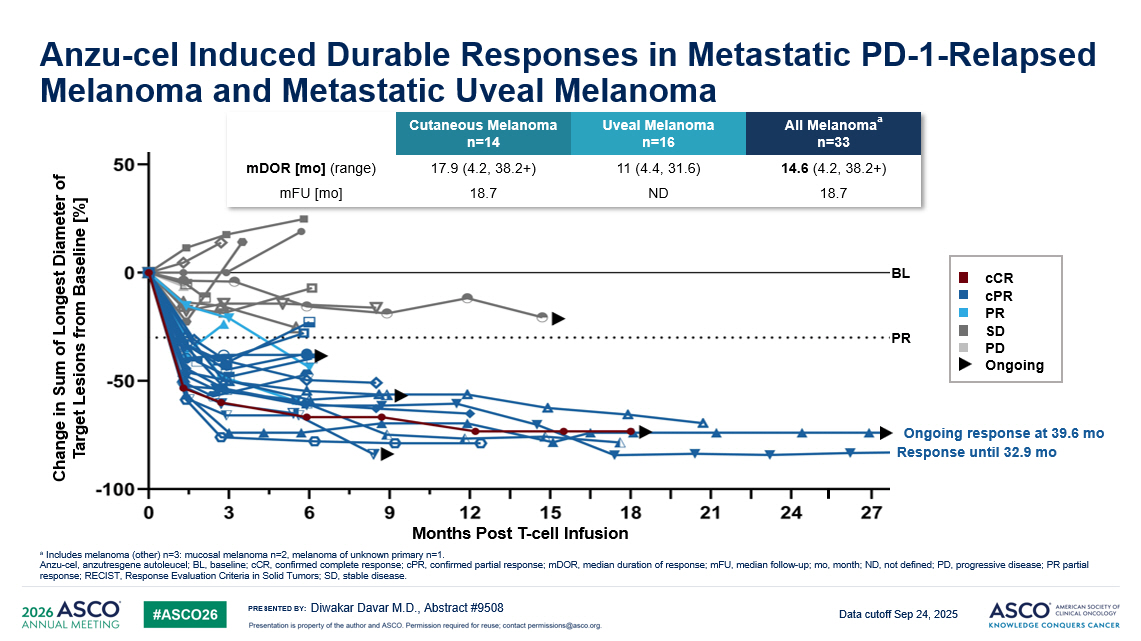
PRESENTED BY: Anzu - cel Induced Durable Responses in Metastatic PD - 1 - Relapsed Melanoma and Metastatic Uveal Melanoma Diwakar Davar M.D., Abstract #9508 a Includes melanoma (other) n=3: mucosal melanoma n=2, melanoma of unknown primary n=1. Anzu - cel, a nzutresgene autoleucel ; BL, baseline; cCR , confirmed complete response; cPR , confirmed partial response; mDOR , median duration of response; mFU , median follow - up; mo , month; ND, not defined; PD, progressive disease; PR partial response; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease. Data cutoff Sep 24, 2025 Change in Sum of Longest Diameter of Target Lesions from Baseline [%] Months Post T - cell Infusion Ongoing response at 39.6 mo Response until 32.9 mo BL PR All Melanoma a n=33 Uveal Melanoma n=16 Cutaneous Melanoma n=14 14.6 (4.2, 38.2+) 11 (4.4, 31.6) 17.9 (4.2, 38.2+) mDOR [ mo ] (range) 18.7 ND 18.7 mFU [ mo ] cCR cPR PR SD PD Ongoing
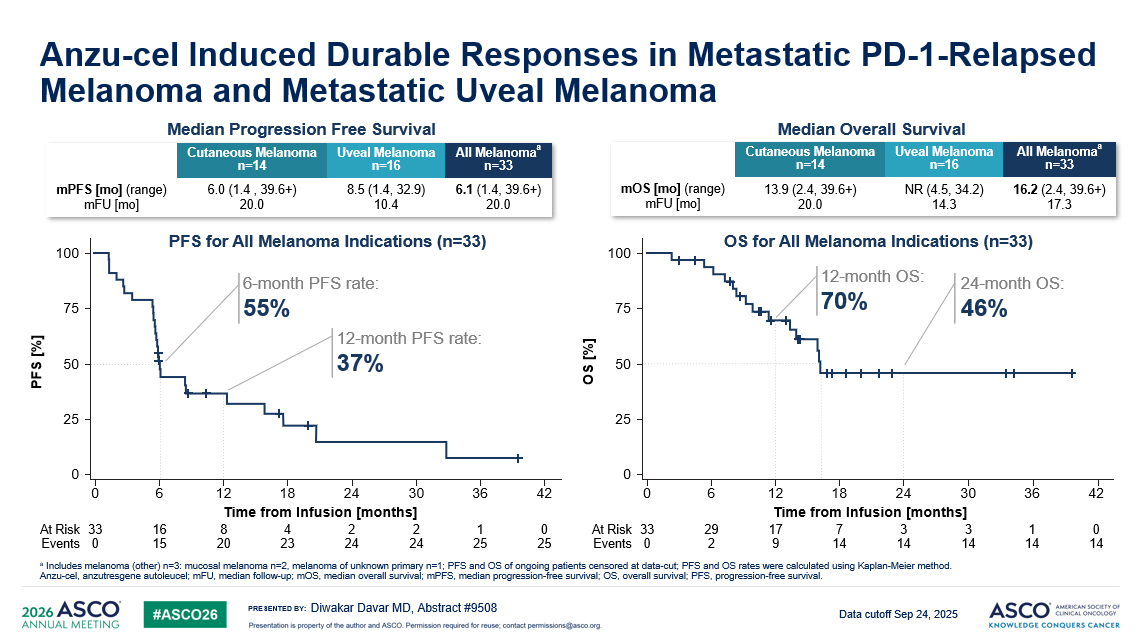
PRESENTED BY: Anzu - cel Induced Durable Responses in Metastatic PD - 1 - Relapsed Melanoma and Metastatic Uveal Melanoma Diwakar Davar MD, Abstract #9508 a Includes melanoma (other) n=3: mucosal melanoma n=2, melanoma of unknown primary n=1; PFS and OS of ongoing patients censored a t data - cut; PFS and OS rates were calculated using Kaplan - Meier method. Anzu - cel, a nzutresgene autoleucel ; mFU , median follow - up; mOS , median overall survival; mPFS , median progression - free survival; OS, overall survival; PFS, progression - free survival. Data cutoff Sep 24, 2025 Median Progression Free Survival Median Overall Survival All Melanoma a n=33 Uveal Melanoma n=16 Cutaneous Melanoma n=14 6.1 (1.4, 39.6+) 20.0 8.5 (1.4, 32.9) 10.4 6.0 (1.4 , 39.6+) 20.0 mPFS [ mo ] (range) mFU [ mo ] All Melanoma a n=33 Uveal Melanoma n=16 Cutaneous Melanoma n=14 16.2 (2.4, 39.6+) 17.3 NR (4.5, 34.2) 14.3 1 3 .9 (2.4, 39.6+) 20.0 mOS [ mo ] (range) mFU [ mo ] 6 - month PFS rate: 55% 100 PFS [%] 0 75 50 25 0 6 12 18 24 30 36 42 Time from Infusion [months] 33 16 8 4 2 2 1 0 0 15 20 23 24 24 25 25 At Risk Events PFS for All Melanoma Indications (n=33) 12 - month PFS rate: 37% 24 - month OS: 46% 100 OS [%] 0 75 50 25 0 6 12 18 24 30 36 42 Time from Infusion [months] 33 29 17 7 3 3 1 0 0 2 9 14 14 14 14 14 At Risk Events OS for All Melanoma Indications (n=33) 12 - month OS: 70%
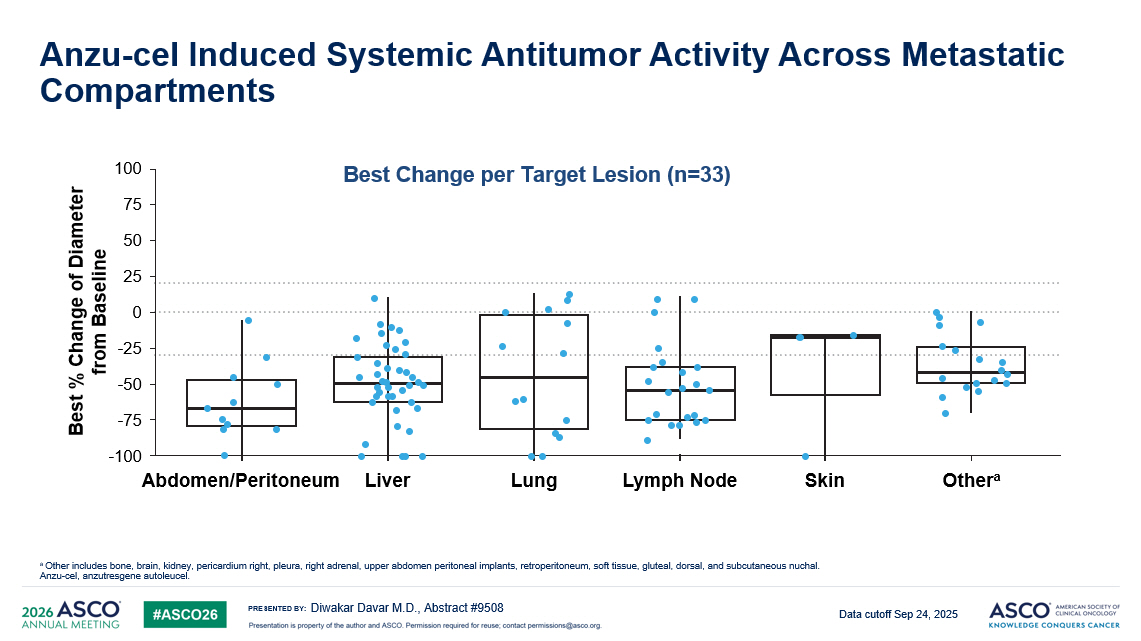
PRESENTED BY: Anzu - cel Induced Systemic Antitumor Activity Across Metastatic Compartments Diwakar Davar M.D., Abstract #9508 a Other includes bone, brain, kidney, pericardium right, pleura, right adrenal, upper abdomen peritoneal implants, retroperiton eum , soft tissue, gluteal, dorsal, and subcutaneous nuchal. Anzu - cel, a nzutresgene autoleucel . Best Change per Target L esion (n=33) Data cutoff Sep 24, 2025 100 75 50 25 0 - 25 - 50 - 75 - 100 Best % Change of Diameter from Baseline Abdomen/Peritoneum Liver Lung Lymph Node Skin Other a
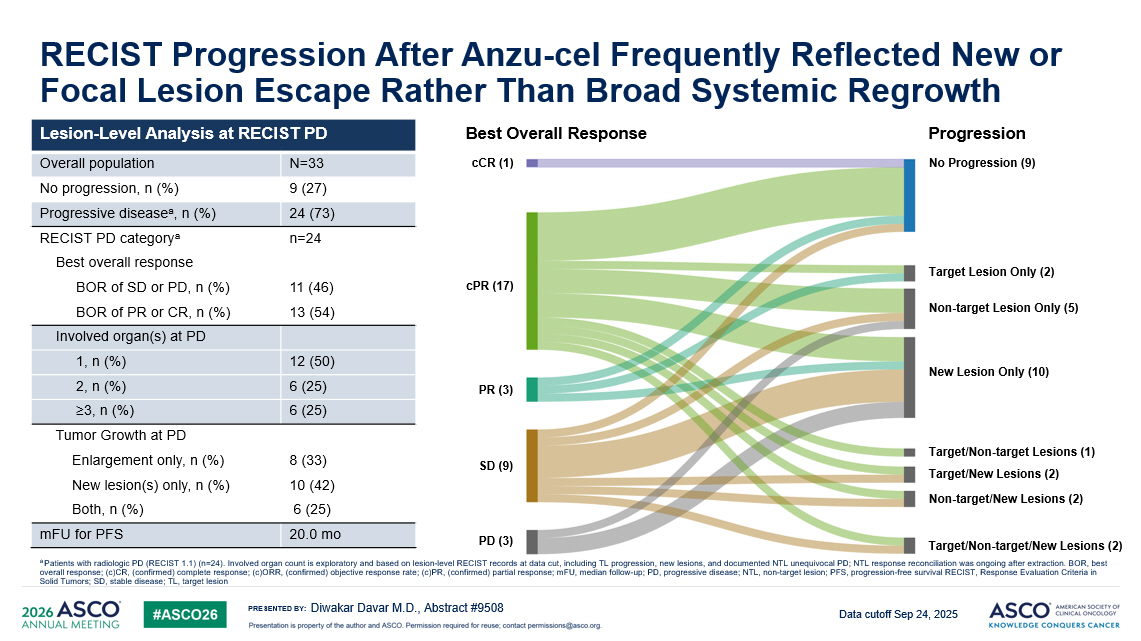
PRESENTED BY: RECIST Progression After Anzu - cel Frequently Reflected New or Focal Lesion Escape Rather Than Broad Systemic Regrowth Diwakar Davar M.D., Abstract #9508 cCR (1) cPR (17) PR (3) SD (9) PD (3) No Progression (9) Non - target Lesion Only (5) New Lesion Only (10) Target/Non - target Lesions (1) Target/New Lesions (2) Non - target/New Lesions (2) Target/Non - target/New Lesions (2) Target Lesion Only (2) Best Overall Response Progression Data cutoff Sep 24, 2025 Lesion - Level Analysis at RECIST PD N=33 Overall population 9 (27) No progression , n (%) 24 (73) Progressive disease a , n (%) n=24 RECIST PD category a Best overall response 11 (46) BOR of SD or PD , n (%) 13 (54) BOR of PR or CR , n (%) Involved organ(s) at PD 12 (50) 1, n (%) 6 (25) 2, n (%) 6 (25) ≥3, n (%) Tumor Growth at PD 8 (33) Enlargement only , n (%) 10 (42) New lesion(s) only , n (%) 6 (25) Both , n (%) 20.0 mo mFU for PFS a Patients with radiologic PD (RECIST 1.1) (n=24). Involved organ count is exploratory and based on lesion - level RECIST records at data cut, including TL progression, new lesions, and documented NTL unequivocal PD; NTL response reconciliation was ongoing a ft er extraction. BOR, best overall response; (c)CR, (confirmed) complete response; (c)ORR, (confirmed) objective response rate; (c)PR, (confirmed) parti al response; mFU , median follow - up; PD, progressive disease; NTL, non - target lesion; PFS, progression - free survival RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease; TL, target lesion
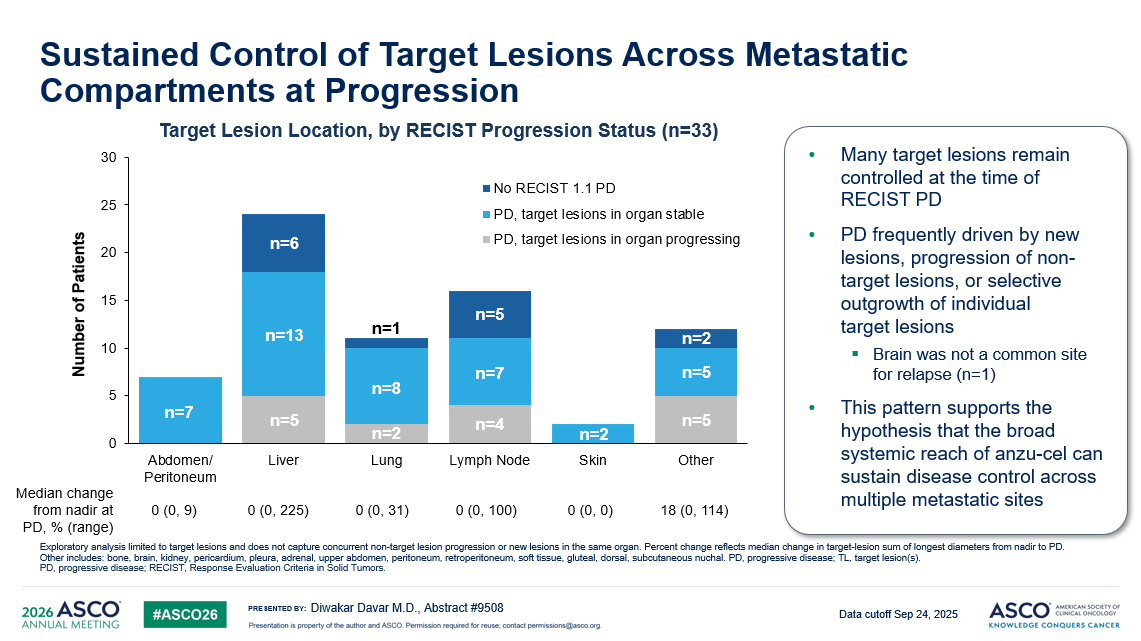
PRESENTED BY: Sustained Control of Target Lesions Across Metastatic Compartments at Progression Diwakar Davar M.D., Abstract #9508 Exploratory analysis limited to target lesions and does not capture concurrent non - target lesion progression or new lesions in t he same organ. Percent change reflects median change in target - lesion sum of longest diameters from nadir to PD. Other includes: bone, brain, kidney, pericardium, pleura, adrenal, upper abdomen, peritoneum, retroperitoneum, soft tissue, gluteal, dorsal, su bcutaneous nuchal. PD, progressive disease; TL, target lesion(s). PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors. • Many target lesions remain controlled at the time of RECIST PD • PD frequently driven by new lesions, progression of non - target lesions, or selective outgrowth of individual target lesions ▪ Brain was not a common site for relapse (n=1) • This pattern supports the hypothesis that the broad systemic reach of anzu - cel can sustain disease control across multiple metastatic sites Data cutoff Sep 24, 2025 18 (0, 114) 0 (0, 0) 0 (0, 100) 0 (0, 31) 0 (0, 225) 0 (0, 9) Median change from nadir at PD, % (range) 0 5 10 15 20 25 30 Abdomen/ Peritoneum Liver Lung Lymph Node Skin Other Number of Patients No RECIST 1.1 PD PD, target lesions in organ stable PD, target lesions in organ progressing Target Lesion Location, by RECIST Progression Status (n=33) n=7 n=6 n=13 n=5 n=1 n=8 n=2 n=5 n=7 n=4 n=2 n=2 n=5 n=5
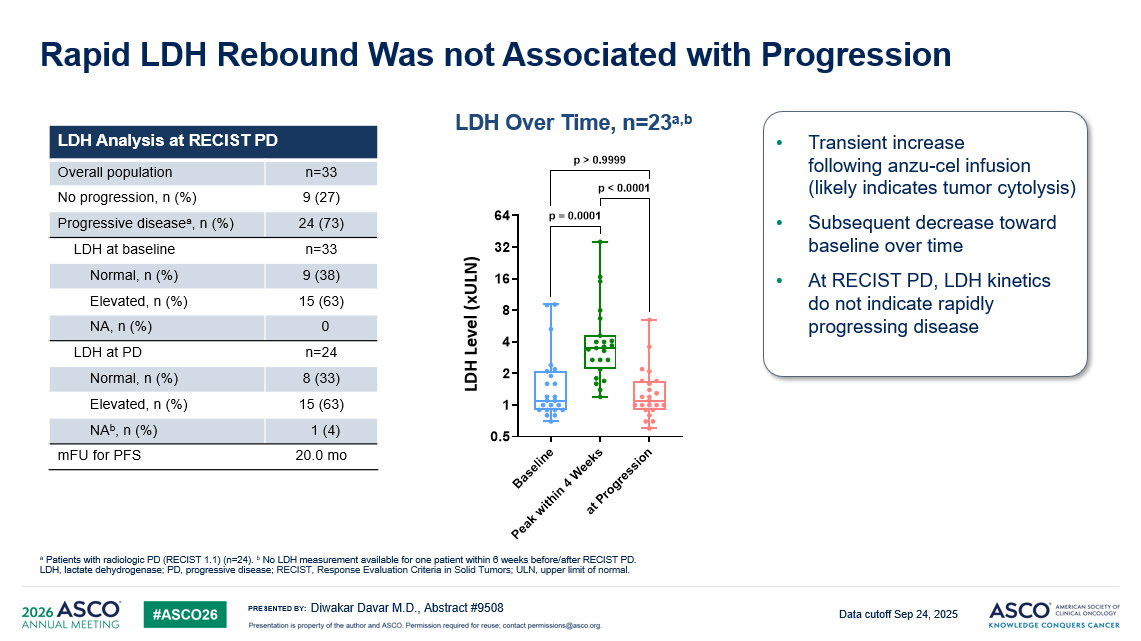
PRESENTED BY: Rapid LDH Rebound Was not Associated with Progression LDH Analysis at RECIST PD n=33 Overall population 9 (27) No progression , n (%) 24 (73) Progressive disease a , n (%) n=33 LDH at baseline 9 (38) Normal , n (%) 15 (63) Elevated , n (%) 0 NA , n (%) n=24 LDH at PD 8 (33) Normal , n (%) 15 (63) Elevated , n (%) 1 (4) NA b , n (%) 20.0 mo mFU for PFS Diwakar Davar M.D., Abstract #9508 a Patients with radiologic PD (RECIST 1.1) (n=24). b No LDH measurement available for one patient within 6 weeks before/after RECIST PD. LDH, lactate dehydrogenase; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors ; ULN, upper limit of normal . • Transient increase following anzu - cel infusion (likely indicates tumor cytolysis) • Subsequent decrease toward baseline over time • At RECIST PD, LDH kinetics do not indicate rapidly progressing disease B a s e l i n e P e a k w i t h i n 4 W e e k s a t P r o g r e s s i o n 0.5 1 2 4 8 16 32 64 L D H ( F o l d c h a n g e r e l a t i v e t o U L N ) p = 0.0001 p > 0.9999 p < 0.0001 LDH Level ( xULN ) LDH Over Time, n=23 a,b Data cutoff Sep 24, 2025
PRESENTED BY: Key Takeaways • TCR - based therapies enable immune recognition of intracellular tumor antigens presented by cell - surface HLA, expanding the therapeutic landscape beyond targets accessible to conventional immunotherapies • Anzutresgene autoleucel ( anzu - cel, IMA203) is a one - time autologous TCR T - cell therapy targeting the cancer - associated antigen PRAME, which is expressed in >50 cancers and represents a novel immunotherapy target for melanoma • Anzu - cel demonstrates a predictable and manageable tolerability profile and rapid, deep, and durable systemic antitumor activity in settings of high unmet need: metastatic PD - 1 - relapsed melanoma and metastatic uveal melanoma • Exploratory response analysis supports the hypothesis that the broad systemic reach of anzu - cel can sustain disease control across multiple metastatic sites • Findings support continued development of anzu - cel in melanoma, including the randomized Phase 3 SUPRAME trial (NCT06743126) Diwakar Davar M.D., Abstract #9508 Anzu - cel, anzutresgene autoleucel ; HLA, human leukocyte antigen; PRAME, preferentially expressed antigen in melanoma; TCR, T - cell receptor.
PRESENTED BY: 16 Anzu - cel (IMA203) Phase 1 Trial Sponsor: Immatics Thank You – Trial Participants & Caregivers 16 University of Pittsburgh Medical Center UT MD Anderson United States University of Miami University Hospital Dresden University Hospital Hamburg Charité Berlin Germany University Hospital Würzburg CCC Comprehensive Cancer Center Mainfranken University Hospital Bonn Diwakar Davar M.D., Abstract #9508
PRESENTED BY: Appendix Diwakar Davar M.D., Abstract #9508
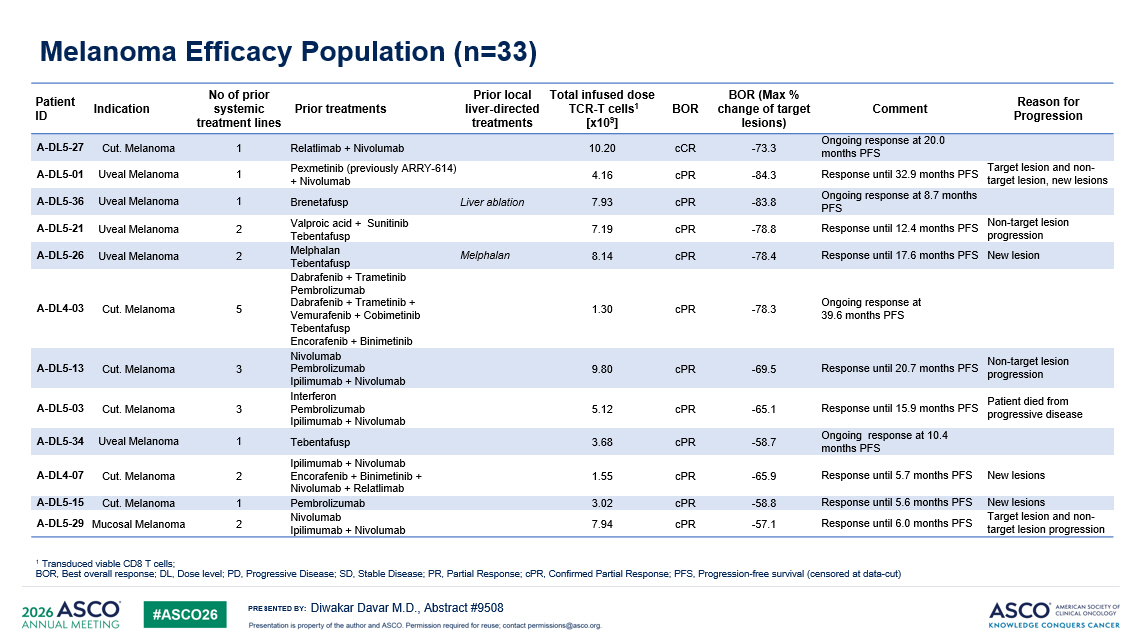
PRESENTED BY: Melanoma Efficacy Population (n=33) 1 Transduced viable CD8 T cells ; BOR, Best overall response ; DL, Dose level ; PD, Progressive Disease; SD, Stable Disease; PR, Partial Response; cPR , Confirmed Partial Response; PFS, Progression - free survival ( censored at data - cut ) Reason for Progression Comment BOR (Max % change of target lesions) BOR Total infused dose TCR - T cells 1 [x10 9 ] Prior local liver - directed treatments Prior treatments No of prior systemic treatment lines Indication Patient ID Ongoing response at 20.0 months PFS - 73.3 cCR 10.20 Relatlimab + Nivolumab 1 Cut. Melanoma A - DL5 - 27 Target lesion and non - target lesion, new lesions Response until 32.9 months PFS - 84.3 cPR 4.16 Pexmetinib (previously ARRY - 614) + Nivolumab 1 Uveal Melanoma A - DL5 - 01 Ongoing response at 8.7 months PFS - 83.8 cPR 7.93 Liver ablation Brenetafusp 1 Uveal Melanoma A - DL5 - 36 Non - target lesion progression Response until 12.4 months PFS - 78.8 cPR 7.19 Valproic acid + Sunitinib Tebentafusp 2 Uveal Melanoma A - DL5 - 21 New lesion Response until 17.6 months PFS - 78.4 cPR 8.14 Melphalan Melphalan Tebentafusp 2 Uveal Melanoma A - DL5 - 26 Ongoing response at 39.6 months PFS - 78.3 cPR 1.30 Dabrafenib + Trametinib Pembrolizumab Dabrafenib + Trametinib + Vemurafenib + Cobimetinib Tebentafusp Encorafenib + Binimetinib 5 Cut. Melanoma A - DL4 - 03 Non - target lesion progression Response until 20.7 months PFS - 69.5 cPR 9.80 Nivolumab Pembrolizumab Ipilimumab + Nivolumab 3 Cut. Melanoma A - DL5 - 13 Patient died from progressive disease Response until 15.9 months PFS - 65.1 cPR 5.12 Interferon Pembrolizumab Ipilimumab + Nivolumab 3 Cut. Melanoma A - DL5 - 03 Ongoing response at 10.4 months PFS - 58.7 cPR 3.68 Tebentafusp 1 Uveal Melanoma A - DL5 - 34 New lesions Response until 5.7 months PFS - 65.9 cPR 1.55 Ipilimumab + Nivolumab Encorafenib + Binimetinib + Nivolumab + Relatlimab 2 Cut. Melanoma A - DL4 - 07 New lesions Response until 5.6 months PFS - 58.8 cPR 3.02 Pembrolizumab 1 Cut. Melanoma A - DL5 - 15 Target lesion and non - target lesion progression Response until 6.0 months PFS - 57.1 cPR 7.94 Nivolumab Ipilimumab + Nivolumab 2 Mucosal Melanoma A - DL5 - 29 Diwakar Davar M.D., Abstract #9508
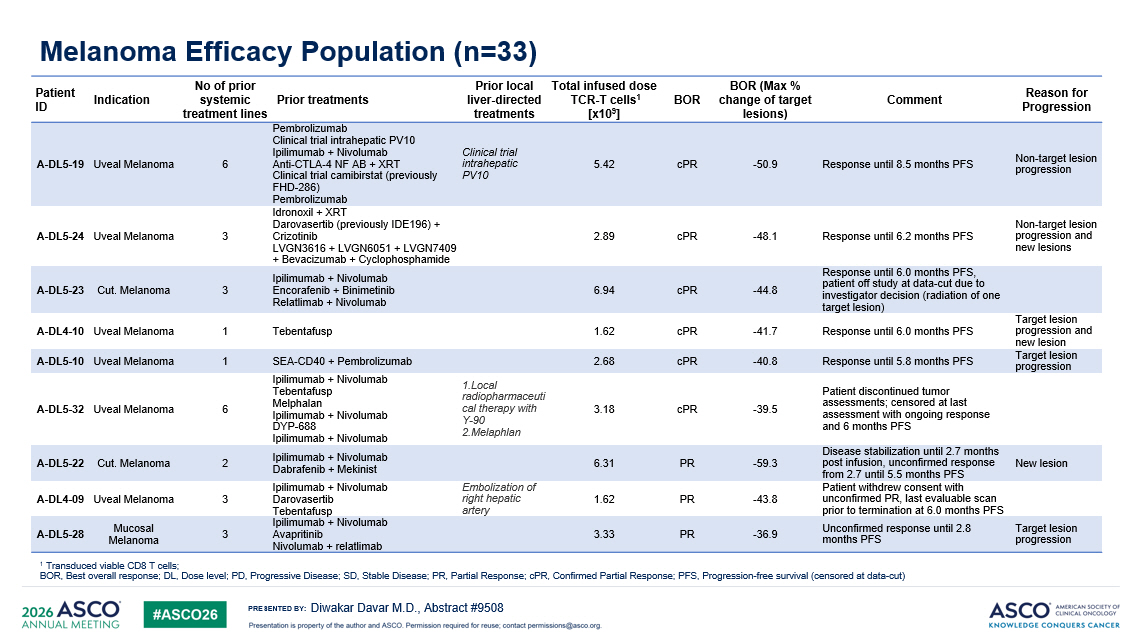
PRESENTED BY: Melanoma Efficacy Population (n=33) Reason for Progression Comment BOR (Max % change of target lesions) BOR Total infused dose TCR - T cells 1 [x10 9 ] Prior local liver - directed treatments Prior treatments No of prior systemic treatment lines Indication Patient ID Non - target lesion progression Response until 8.5 months PFS - 50.9 cPR 5.42 Clinical trial intrahepatic PV10 Pembrolizumab Clinical trial intrahepatic PV10 Ipilimumab + Nivolumab Anti - CTLA - 4 NF AB + XRT Clinical trial camibirstat (previously FHD - 286) Pembrolizumab 6 Uveal Melanoma A - DL5 - 19 Non - target lesion progression and new lesions Response until 6.2 months PFS - 48.1 cPR 2.89 Idronoxil + XRT Darovasertib (previously IDE196) + Crizotinib LVGN3616 + LVGN6051 + LVGN7409 + Bevacizumab + Cyclophosphamide 3 Uveal Melanoma A - DL5 - 24 Response until 6.0 months PFS, patient off study at data - cut due to investigator decision (radiation of one target lesion) - 44.8 cPR 6.94 Ipilimumab + Nivolumab Encorafenib + Binimetinib Relatlimab + Nivolumab 3 Cut. Melanoma A - DL5 - 23 Target lesion progression and new lesion Response until 6.0 months PFS - 41.7 cPR 1.62 Tebentafusp 1 Uveal Melanoma A - DL4 - 10 Target lesion progression Response until 5.8 months PFS - 40.8 cPR 2.68 SEA - CD40 + Pembrolizumab 1 Uveal Melanoma A - DL5 - 10 Patient discontinued tumor assessments; censored at last assessment with ongoing response and 6 months PFS - 39.5 cPR 3.18 1.Local radiopharmaceuti cal therapy with Y - 90 2.Melaphlan Ipilimumab + Nivolumab Tebentafusp Melphalan Ipilimumab + Nivolumab DYP - 688 Ipilimumab + Nivolumab 6 Uveal Melanoma A - DL5 - 32 New lesion Disease stabilization until 2.7 months post infusion, unconfirmed response from 2.7 until 5.5 months PFS - 59.3 PR 6.31 Ipilimumab + Nivolumab Dabrafenib + Mekinist 2 Cut. Melanoma A - DL5 - 22 Patient withdrew consent with unconfirmed PR, last evaluable scan prior to termination at 6.0 months PFS - 43.8 PR 1.62 Embolization of right hepatic artery Ipilimumab + Nivolumab Darovasertib Tebentafusp 3 Uveal Melanoma A - DL4 - 09 Target lesion progression Unconfirmed response until 2.8 months PFS - 36.9 PR 3.33 Ipilimumab + Nivolumab Avapritinib Nivolumab + relatlimab 3 Mucosal Melanoma A - DL5 - 28 1 Transduced viable CD8 T cells ; BOR, Best overall response ; DL, Dose level ; PD, Progressive Disease; SD, Stable Disease; PR, Partial Response; cPR , Confirmed Partial Response; PFS, Progression - free survival ( censored at data - cut ) Diwakar Davar M.D., Abstract #9508
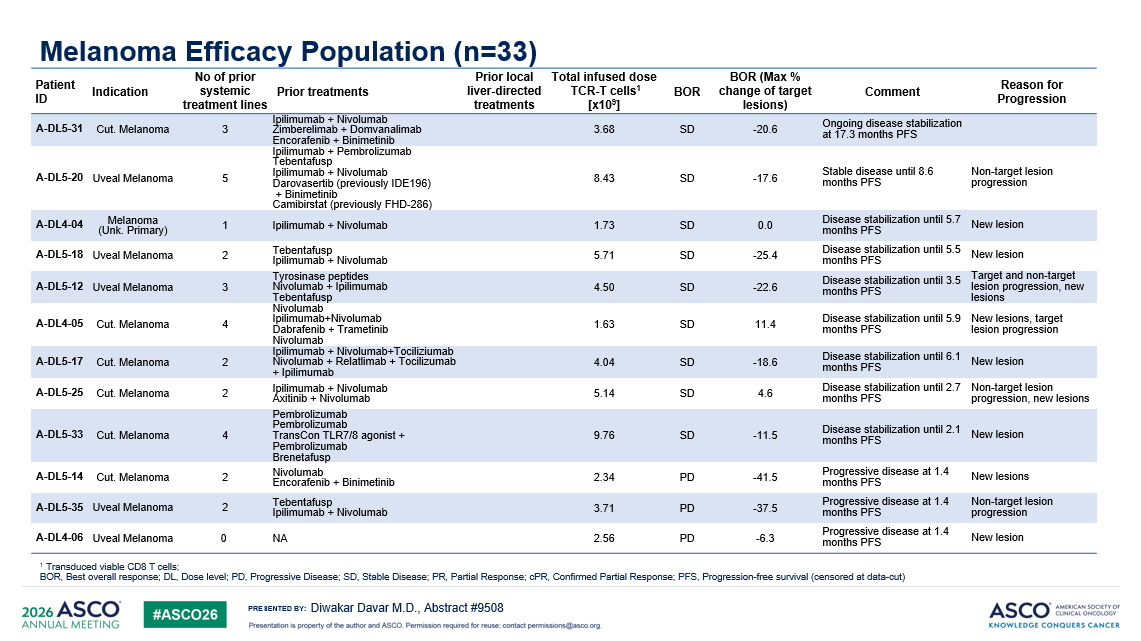
PRESENTED BY: Melanoma Efficacy Population (n=33) 1 Transduced viable CD8 T cells ; BOR, Best overall response ; DL, Dose level ; PD, Progressive Disease; SD, Stable Disease; PR, Partial Response; cPR , Confirmed Partial Response; PFS, Progression - free survival ( censored at data - cut ) Reason for Progression Comment BOR (Max % change of target lesions) BOR Total infused dose TCR - T cells 1 [x10 9 ] Prior local liver - directed treatments Prior treatments No of prior systemic treatment lines Indication Patient ID Ongoing disease stabilization at 17.3 months PFS - 20.6 SD 3.68 Ipilimumab + Nivolumab Zimberelimab + Domvanalimab Encorafenib + Binimetinib 3 Cut. Melanoma A - DL5 - 31 Non - target lesion progression Stable disease until 8.6 months PFS - 17.6 SD 8.43 Ipilimumab + Pembrolizumab Tebentafusp Ipilimumab + Nivolumab Darovasertib (previously IDE196) + Binimetinib Camibirstat (previously FHD - 286) 5 Uveal Melanoma A - DL5 - 20 New lesion Disease stabilization until 5.7 months PFS 0.0 SD 1.73 Ipilimumab + Nivolumab 1 Melanoma (Unk. Primary) A - DL4 - 04 New lesion Disease stabilization until 5.5 months PFS - 25.4 SD 5.71 Tebentafusp Ipilimumab + Nivolumab 2 Uveal Melanoma A - DL5 - 18 Target and non - target lesion progression, new lesions Disease stabilization until 3.5 months PFS - 22.6 SD 4.50 Tyrosinase peptides Nivolumab + Ipilimumab Tebentafusp 3 Uveal Melanoma A - DL5 - 12 New lesions, target lesion progression Disease stabilization until 5.9 months PFS 11.4 SD 1.63 Nivolumab Ipilimumab+Nivolumab Dabrafenib + Trametinib Nivolumab 4 Cut. Melanoma A - DL4 - 05 New lesion Disease stabilization until 6.1 months PFS - 18.6 SD 4.04 Ipilimumab + Nivolumab+Tociliziumab Nivolumab + Relatlimab + Tocilizumab + Ipilimumab 2 Cut. Melanoma A - DL5 - 17 Non - target lesion progression, new lesions Disease stabilization until 2.7 months PFS 4.6 SD 5.14 Ipilimumab + Nivolumab Axitinib + Nivolumab 2 Cut. Melanoma A - DL5 - 25 New lesion Disease stabilization until 2.1 months PFS - 11.5 SD 9.76 Pembrolizumab Pembrolizumab TransCon TLR7/8 agonist + Pembrolizumab Brenetafusp 4 Cut. Melanoma A - DL5 - 33 New lesions Progressive disease at 1.4 months PFS - 41.5 PD 2.34 Nivolumab Encorafenib + Binimetinib 2 Cut. Melanoma A - DL5 - 14 Non - target lesion progression Progressive disease at 1.4 months PFS - 37.5 PD 3.71 Tebentafusp Ipilimumab + Nivolumab 2 Uveal Melanoma A - DL5 - 35 New lesion Progressive disease at 1.4 months PFS - 6.3 PD 2.56 NA 0 Uveal Melanoma A - DL4 - 06 Diwakar Davar M.D., Abstract #9508