.2
Phase 3 Emerge Study Topline Data Readout

This presentation (the “Presentation”) has been prepared by Definium Therapeutics, Inc. (“Definium”, the “Company”, “we”, “ou r” or “us") solely for informational purposes. This Presentation does not constitute an offering of, or a solicitation of an off er to purchase, securities of Definium and under no circumstances is it to be construed as a prospectus or advertisement or public offering of securitie s. Any trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use shou ld not be construed as an endorsement of the products or services of Definium. Any amounts are in USD unless otherwise noted. Definium’s securities hav e not been approved or disapproved by the U.S. Securities and Exchange Commission (the "SEC") or by any state, provincial or oth er securities regulatory authority, nor has the SEC or any state, provincial or other securities regulatory authority passed on the accurac y o r adequacy of this Presentation. Any representation to the contrary is a criminal offense. Cautionary Note Regarding Forward - Looking Statements This Presentation contains, and our officers and representatives may from time to time make, “forward - looking statements” within the meaning of applicable securities laws and are prospective in nature. Forward - looking statements are not based on historical facts, but rather on current expectations and projections about future events and are therefore subject to risks and uncertainties which could cau se actual results to differ materially from the future results expressed or implied by the forward - looking statements. These sta tements generally can be identified by the use of forward - looking words such as “will”, “may", “should”, “could”, “intend”, “estimate”, “plan”, “antic ipate”, “expect”, “believe”, “potential”, “continue”, “budget”, “scheduled”, “forecasts”, “intends”, “anticipates”, “projects ” o r the negative thereof or similar variations. Forward - looking statements in this Presentation include, but are not limited to, statements regarding the an ticipated design, timing, progress and results of our investigational programs for DT120 oral disintegrating tablet (“ODT”), a p roprietary, pharmaceutically optimized form of lysergide tartrate for the treatment of generalized anxiety disorder, major depressive dis ord er and posttraumatic stress disorder (including the anticipated topline readouts for the Voyage, Panorama and Ascend studies) , D T402, also referred to as R( - ) - MDMA, and any other product candidates; potential expansion of our current pipeline; the success and timing of our de velopment activities; our ability to meet the milestones set forth herein; the likelihood of success of any clinical trials o r o f obtaining U.S. Food and Drug Administration (“FDA”) or other regulatory approvals; our beliefs regarding potential benefits of our product candidates ; o ur belief that DT120 ODT represents a best - in - class profile; the potential commercial opportunity for DT120 ODT, if approved, i ncluding total addressable market; our plans to continue to advance commercial readiness activities, including market access and provider ed uca tion; our cash position; and the potential for psychedelics as a class of treatment options in psychiatry. There are numerous risks and uncertainties that could cause actual results, plans and objectives to differ materially from th ose expressed in forward - looking statements, including history of negative cash flows, limited operating history, incurrence of fut ure losses, availability of additional capital, compliance with laws and regulations, difficulty associated with research and development, risks associat ed with clinical trials or studies, heightened regulatory scrutiny, early stage product development, clinical trial risks, regul ato ry approval processes, novelty of the psychedelic inspired medicines industry, our ability to maintain effective patent rights and other intellectua l p roperty protection for our product candidates, our expectations regarding the size of the eligible patient populations for ou r l ead product candidates, if approved and commercialized; our ability to identify third - party treatment sites to conduct our trials and our ability to identi fy and train appropriate qualified healthcare practitioners to administer our treatments; the pricing, coverage and reimburse men t of our lead product candidates, if approved and commercialized; the rate and degree of market acceptance and clinical utility of our lead product ca ndidates, in particular, and controlled substances, in general; as well as those risk factors described in the Company's Annu al Report on Form 10 - K for the fiscal year ended December 31, 2025, and the Company’s Quarterly Report on Form 10 - Q for the quarterly period ended March 31 , 2026, under headings such as “Special Note Regarding Forward - Looking Statements,” and “Risk Factors” and “Management's Discuss ion and Analysis of Financial Condition and Results of Operations” and other filings and furnishings made by the Company with the sec uri ties regulatory authorities in all provinces and territories of Canada which are available under the Company's profile on SED AR+ at www.sedarplus.ca and with the SEC on EDGAR at www.sec.gov. Any forward - looking statement made by Definium in this Presentation is based only on information currently available to the Comp any and speaks only as of the date on which it is made. Except as required by law, the Company undertakes no duty or obligati on to update any forward - looking statements contained in this Presentation as a result of new information, future events, changes in expectations or otherwise. Cautionary Note Regarding Regulatory Matters The United States federal government regulates drugs through the Controlled Substances Act. DT120 ODT is a proprietary, pharm ace utically optimized form of lysergide D - tartrate and DT402, or R( - ) - MDMA, is our proprietary form of the R - enantiomer of MDMA (3, 4 - methylenedioxymethamphetamine). Lysergide and MDMA are Schedule I substances under the Controlled Substances Act. While the C omp any is focused on programs using psychedelic or hallucinogenic compounds and non - hallucinogenic derivatives of these compounds, including in DT120 ODT, DT402 and its other product candidates, the Company does not have any direct or indirect involvement wit h the illegal selling, production or distribution of any substances in the jurisdictions in which it operates. The Company is a neuro - pharmaceutical drug development company and does not deal with psychedelic or hallucinogenic substances except within laboratory and clinica l t rial settings conducted within approved regulatory frameworks. The Company's products will not be commercialized prior to app lic able regulatory approval, which will only be granted if clinical evidence of safety and efficacy for the intended uses is successfully develo ped . Market and Industry Data This Presentation includes market and industry data that has been obtained from third party sources, including industry publi cat ions. Definium believes that the industry data is accurate and that the estimates and assumptions are reasonable, but there i s n o assurance as to the accuracy or completeness of this data. Third party sources generally state that the information contained therein has been ob tai ned from sources believed to be reliable, but there is no assurance as to the accuracy or completeness of included informatio n. Although the data is believed to be reliable, Definium has not independently verified any of the data from third party sources referred to in this Pr esentation or ascertained the underlying economic assumptions relied upon by such sources. References in this Presentation to re search reports or to articles and publications should not be construed as depicting the complete findings of the entire referenced report or artic le. Definium does not make any representation as to the accuracy of such information. Emerge Topline Results | June 2026 2 Disclaimer

Opening Remarks Rob Barrow Chief Executive Officer

Thank you to our study participants, investigators and partners who made Emerge possible
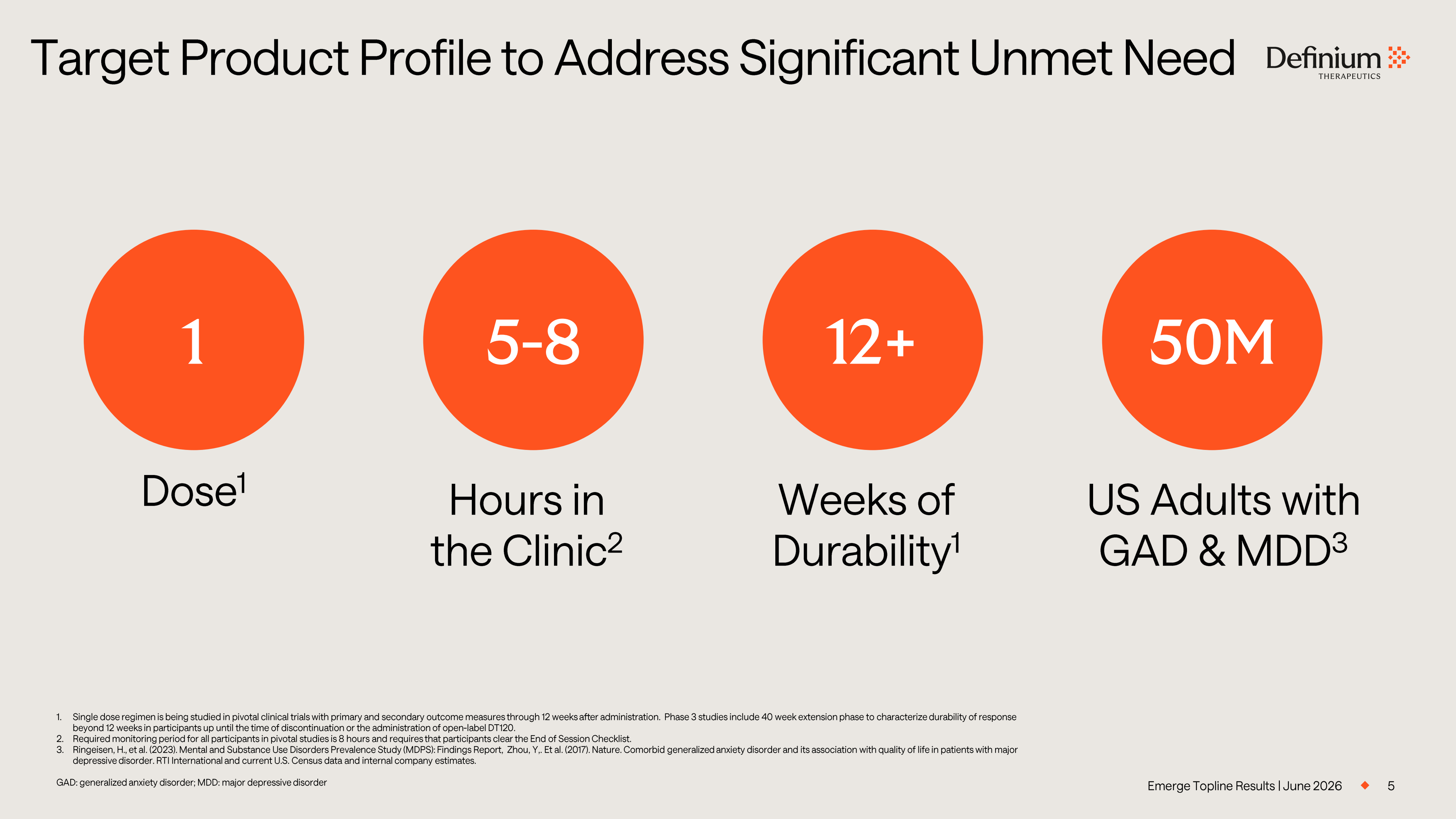
5 1. Single dose regimen is being studied in pivotal clinical trials with primary and secondary outcome measures through 12 weeks aft er administration. Phase 3 studies include 40 week extension phase to characterize durability of response beyond 12 weeks in participants up until the time of discontinuation or the administration of open - label DT120. 2. Required monitoring period for all participants in pivotal studies is 8 hours and requires that participants clear the End of Se ssion Checklist. 3. Ringeisen, H., et al. (2023). Mental and Substance Use Disorders Prevalence Study (MDPS): Findings Report, Zhou, Y,. Et al. (20 17). Nature. Comorbid generalized anxiety disorder and its association with quality of life in patients with major depressive disorder. RTI International and current U.S. Census data and internal company estimates. GAD: generalized anxiety disorder; MDD: major depressive disorder Target Product Profile to Address Significant Unmet Need Emerge Topline Results | June 2026 1 Dose 1 Weeks of Durability 1 Hours in the Clinic 2 US Adults with GAD & MDD 3 5 - 8 12+ 50M
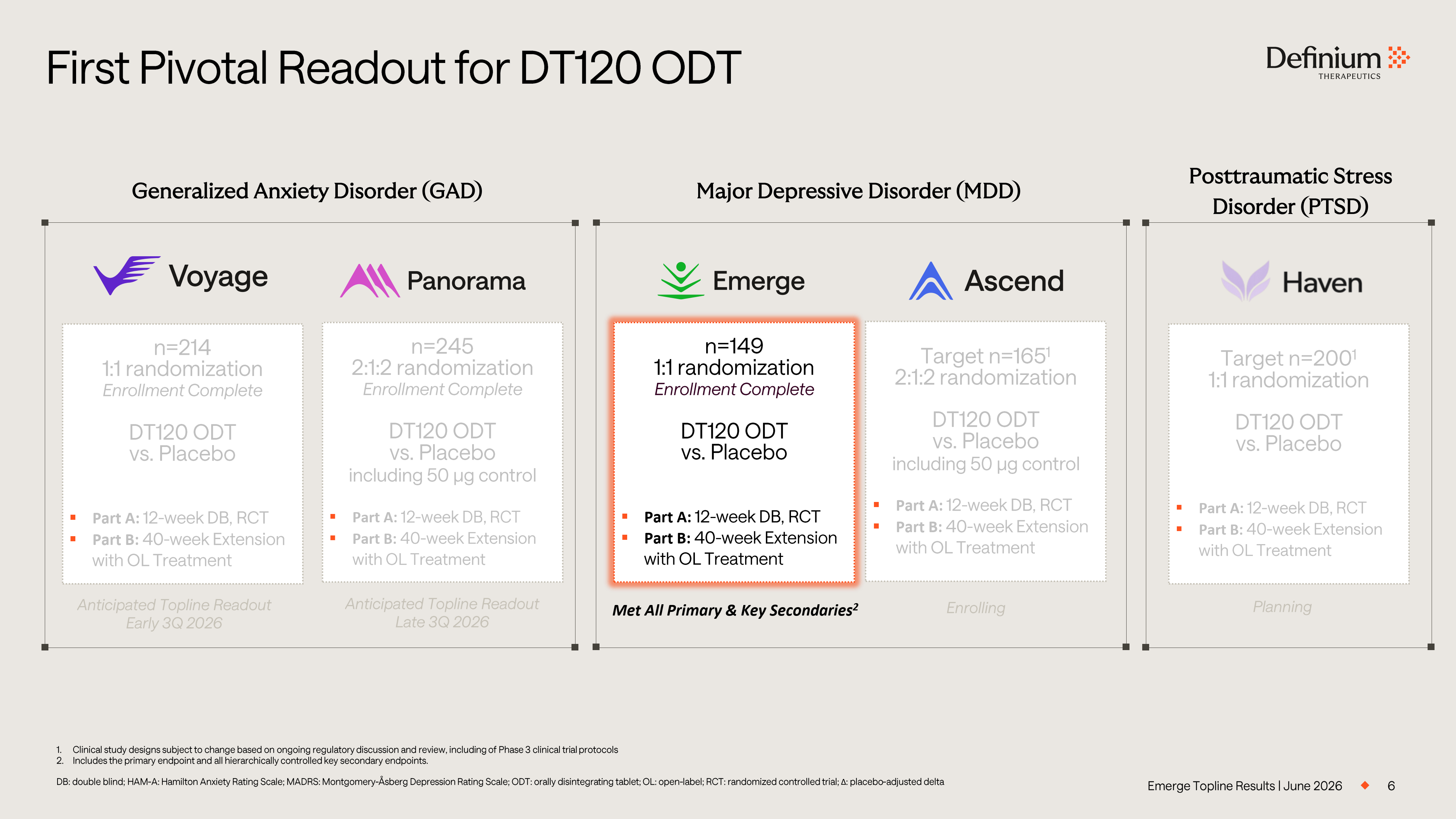
Emerge Topline Results | June 2026 6 First Pivotal Readout for DT120 ODT 1. Clinical study designs subject to change based on ongoing regulatory discussion and review, including of Phase 3 clinical tri al protocols 2. Includes the primary endpoint and all hierarchically controlled key secondary endpoints. DB: double blind; HAM - A: Hamilton Anxiety Rating Scale; MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegra ting tablet; OL: open - label; RCT: randomized controlled trial; Δ : placebo - adjusted delta Generalized Anxiety Disorder (GAD) Major Depressive Disorder (MDD) n=214 1 :1 randomization Enrollment Complete DT120 ODT vs. Placebo ▪ Part A: 12 - week DB, RCT ▪ Part B: 40 - week Extension with OL Treatment n=245 2:1:2 randomization Enrollment Complete DT120 ODT vs. Placebo including 50 µg control ▪ Part A: 12 - week DB, RCT ▪ Part B: 40 - week Extension with OL Treatment n=149 1:1 randomization Enrollment Complete DT120 ODT vs. Placebo ▪ Part A: 12 - week DB, RCT ▪ Part B: 40 - week Extension with OL Treatment Target n=165 1 2:1:2 randomization DT120 ODT vs. Placebo including 50 µg control ▪ Part A: 12 - week DB, RCT ▪ Part B: 40 - week Extension with OL Treatment Target n=200 1 1:1 randomization DT120 ODT vs. Placebo ▪ Part A: 12 - week DB, RCT ▪ Part B: 40 - week Extension with OL Treatment Posttraumatic Stress Disorder (PTSD) Anticipated Topline Readout Early 3Q 2026 Anticipated Topline Readout Late 3Q 2026 Met All Primary & Key Secondaries 2 Enrolling Planning
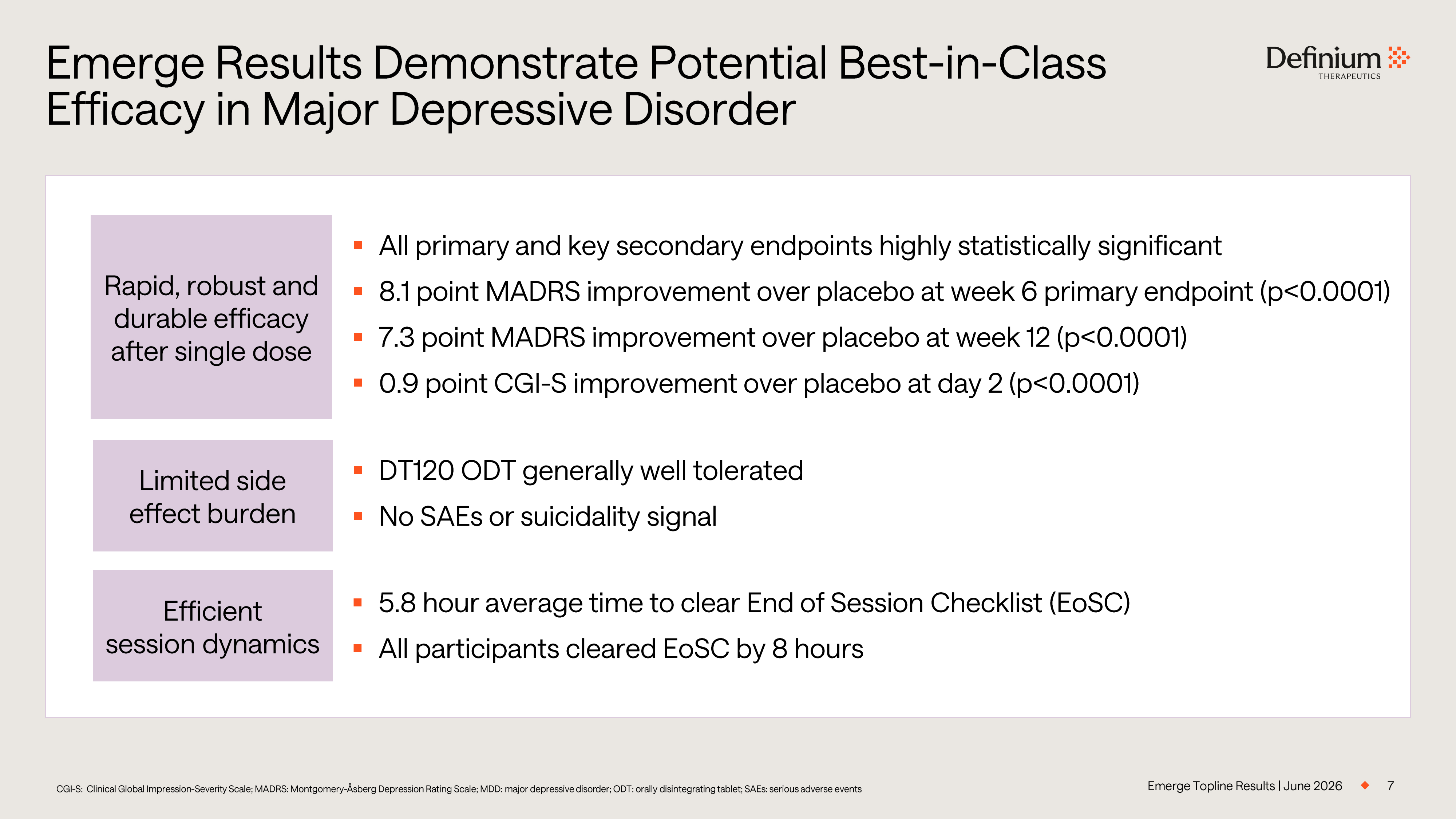
Emerge Topline Results | June 2026 7 Emerge Results Demonstrate Potential Best - in - Class Efficacy in Major Depressive Disorder Limited side effect burden Efficient session dynamics Rapid, robust and durable efficacy after single dose ▪ All primary and key secondary endpoints highly statistically significant ▪ 8.1 point MADRS improvement over placebo at week 6 primary endpoint (p<0.0001) ▪ 7.3 point MADRS improvement over placebo at week 12 (p<0.0001) ▪ 0.9 point CGI - S improvement over placebo at day 2 (p<0.0001) ▪ DT120 ODT generally well tolerated ▪ No SAEs or suicidality signal ▪ 5.8 hour average time to clear End of Session Checklist (EoSC) ▪ All participants cleared EoSC by 8 hours CGI - S: Clinical Global Impression - Severity Scale; MADRS: Montgomery - Åsberg Depression Rating Scale; MDD: major depressive disor der; ODT: orally disintegrating tablet; SAEs: serious adverse events
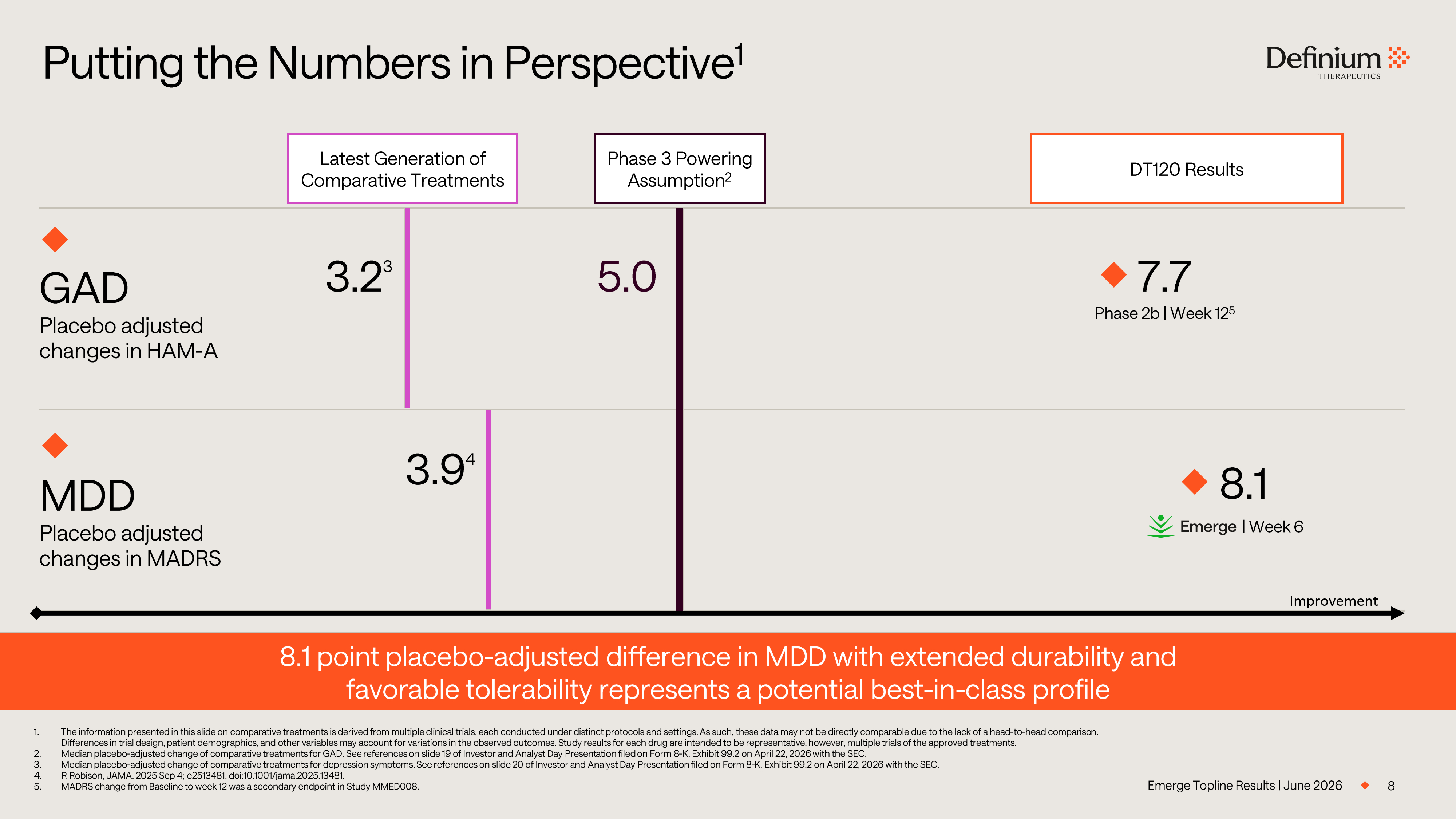
Emerge Topline Results | June 2026 Putting the Numbers in Perspective 1 8 GAD Placebo adjusted changes in HAM - A MDD Placebo adjusted changes in MADRS 1. The information presented in this slide on comparative treatments is derived from multiple clinical trials, each conducted un der distinct protocols and settings. As such, these data may not be directly comparable due to the lack of a head - to - head compariso n. Differences in trial design, patient demographics, and other variables may account for variations in the observed outcomes. S tud y results for each drug are intended to be representative, however, multiple trials of the approved treatments. 2. Median placebo - adjusted change of comparative treatments for GAD. See references on slide 19 of Investor and Analyst Day Present ation filed on Form 8 - K, .2 on April 22, 2026 with the SEC. 3. Median placebo - adjusted change of comparative treatments for depression symptoms. See references on slide 20 of Investor and Analyst Day Presentation filed on Form 8 - K, .2 on April 22, 2026 with the S EC. 4. R Robison, JAMA. 2025 Sep 4; e2513481. doi:10.1001/jama.2025.13481. 5. MADRS change from Baseline to week 12 was a secondary endpoint in Study MMED008. 5.0 3.2 3 7.7 3.9 4 Latest Generation of Comparative Treatments Phase 3 Powering Assumption 2 DT120 Results 8.1 point placebo - adjusted difference in MDD with extended durability and favorable tolerability represents a potential best - in - class profile Improvement 8.1 | Week 6 Phase 2b | Week 12 5
Phase 3 Emerge Study Results Part A – Topline Results Dan Karlin, MD Chief Medical Officer
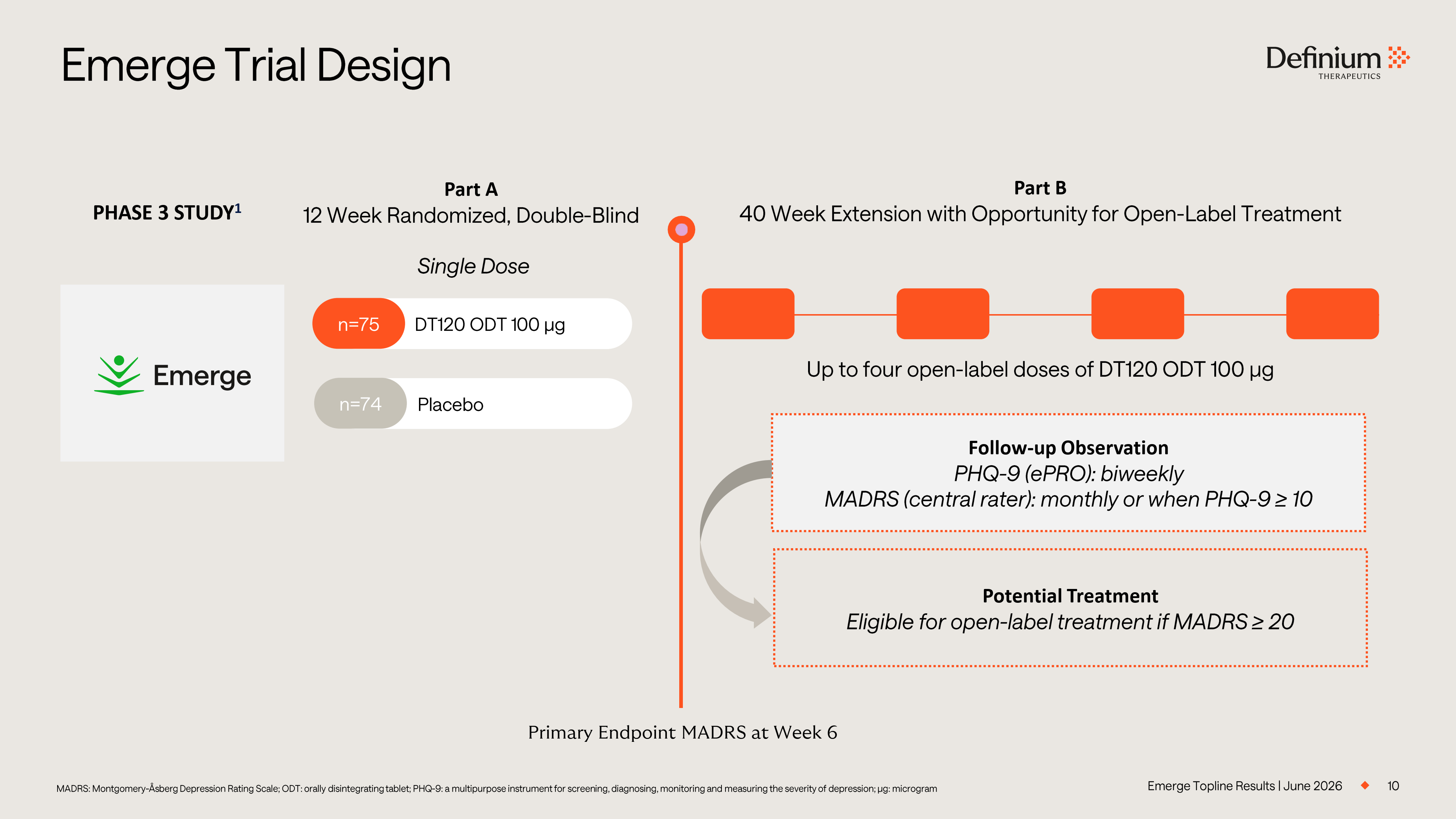
Emerge Trial Design MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegrating tablet; PHQ - 9: a multipurpose instrument for screen ing, diagnosing, monitoring and measuring the severity of depression; µg: microgram DT120 ODT 1 00 µg n=75 Placebo n=74 Part A 12 Week Randomized, Double - Blind Part B 40 Week Extension with Opportunity for Open - Label Treatment PHASE 3 STUDY 1 Single Dose Primary Endpoint MADRS at Week 6 Up to four open - label doses of DT120 ODT 1 00 µg Follow - up Observation PHQ - 9 (ePRO): biweekly MADRS (central rater): monthly or when PHQ - 9 ≥ 10 Potential Treatment Eligible for open - label treatment if MADRS ≥ 20 10 Emerge Topline Results | June 2026
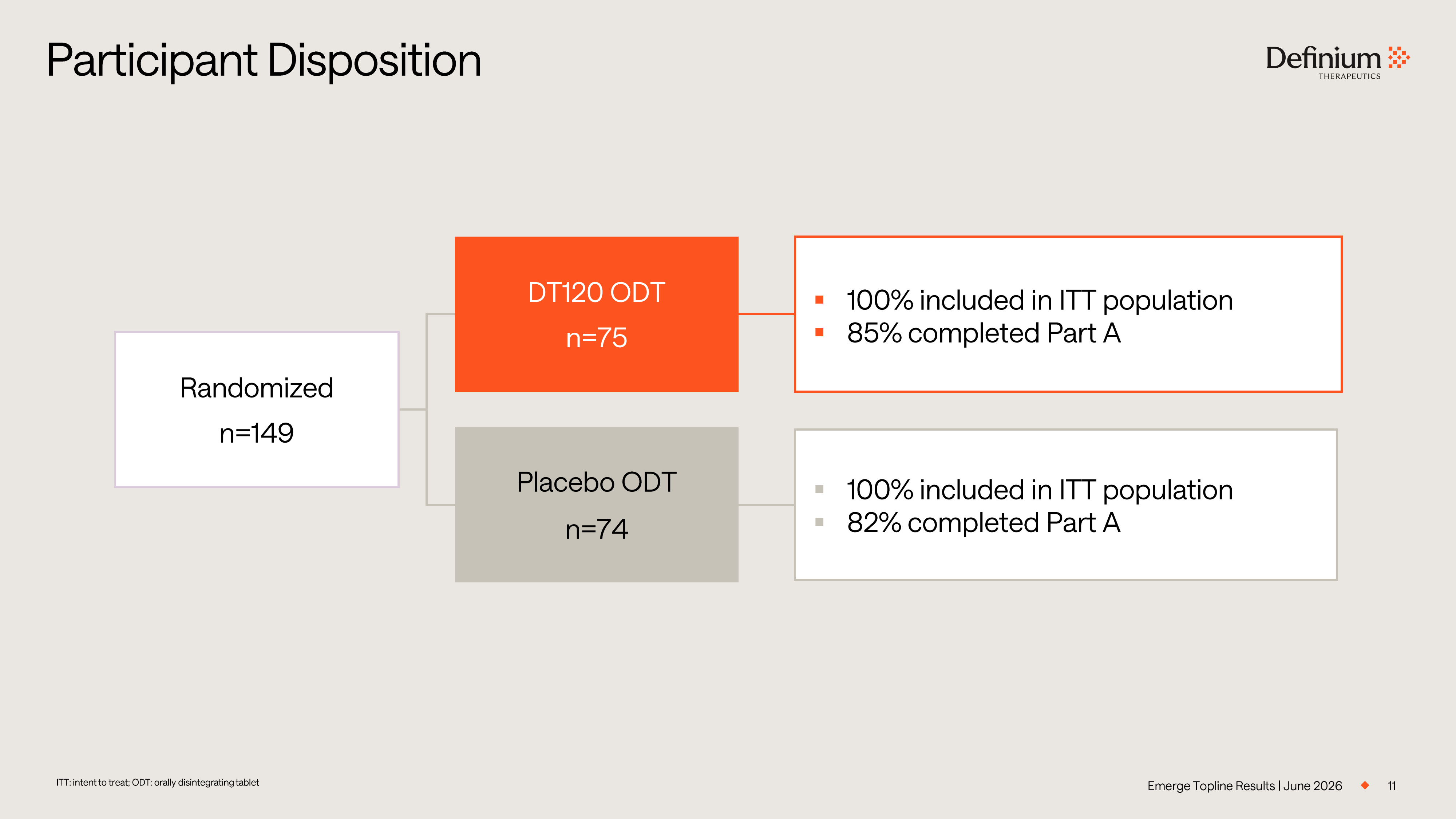
11 ITT: intent to treat; ODT: orally disintegrating tablet Participant Disposition Emerge Topline Results | June 2026 Randomized n=149 DT120 ODT n=75 Placebo ODT n=74 ▪ 100% included in ITT population ▪ 85% completed Part A ▪ 100% included in ITT population ▪ 82% completed Part A
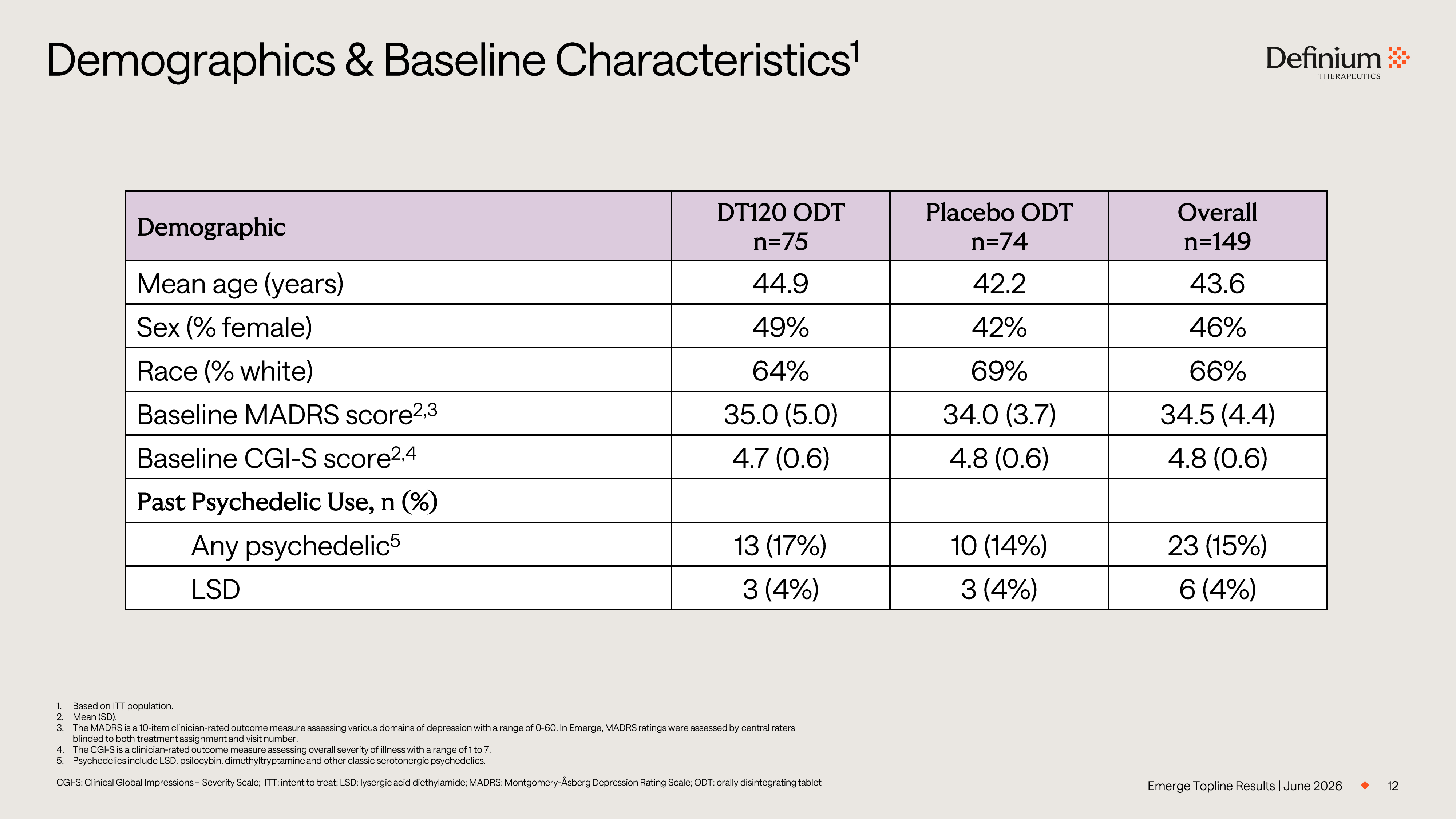
12 1. Based on ITT population. 2. Mean (SD). 3. The MADRS is a 10 - item clinician - rated outcome measure assessing various domains of depression with a range of 0 - 60. In Emerge, MADRS ratings were assessed by central raters blinded to both treatment assignment and visit number. 4. The CGI - S is a clinician - rated outcome measure assessing overall severity of illness with a range of 1 to 7. 5. Psychedelics include LSD, psilocybin, dimethyltryptamine and other classic serotonergic psychedelics. CGI - S: Clinical Global Impressions – Severity Scale; ITT: intent to treat; LSD: lysergic acid diethylamide; MADRS: Montgomery - Å sberg Depression Rating Scale; ODT: orally disintegrating tablet Demographics & Baseline Characteristics 1 Overall n=149 Placebo ODT n=74 DT120 ODT n=75 Demographic 43.6 42.2 44.9 Mean age (years) 46% 42% 49% Sex (% female) 66% 69% 64% Race (% white) 34.5 (4.4) 34.0 (3.7) 35.0 (5.0) Baseline MADRS score 2,3 4.8 (0.6) 4.8 (0.6) 4.7 (0.6) Baseline CGI - S score 2,4 Past Psychedelic Use, n (%) 23 (15%) 10 (14%) 13 (17%) Any psychedelic 5 6 (4%) 3 (4%) 3 (4%) LSD Emerge Topline Results | June 2026
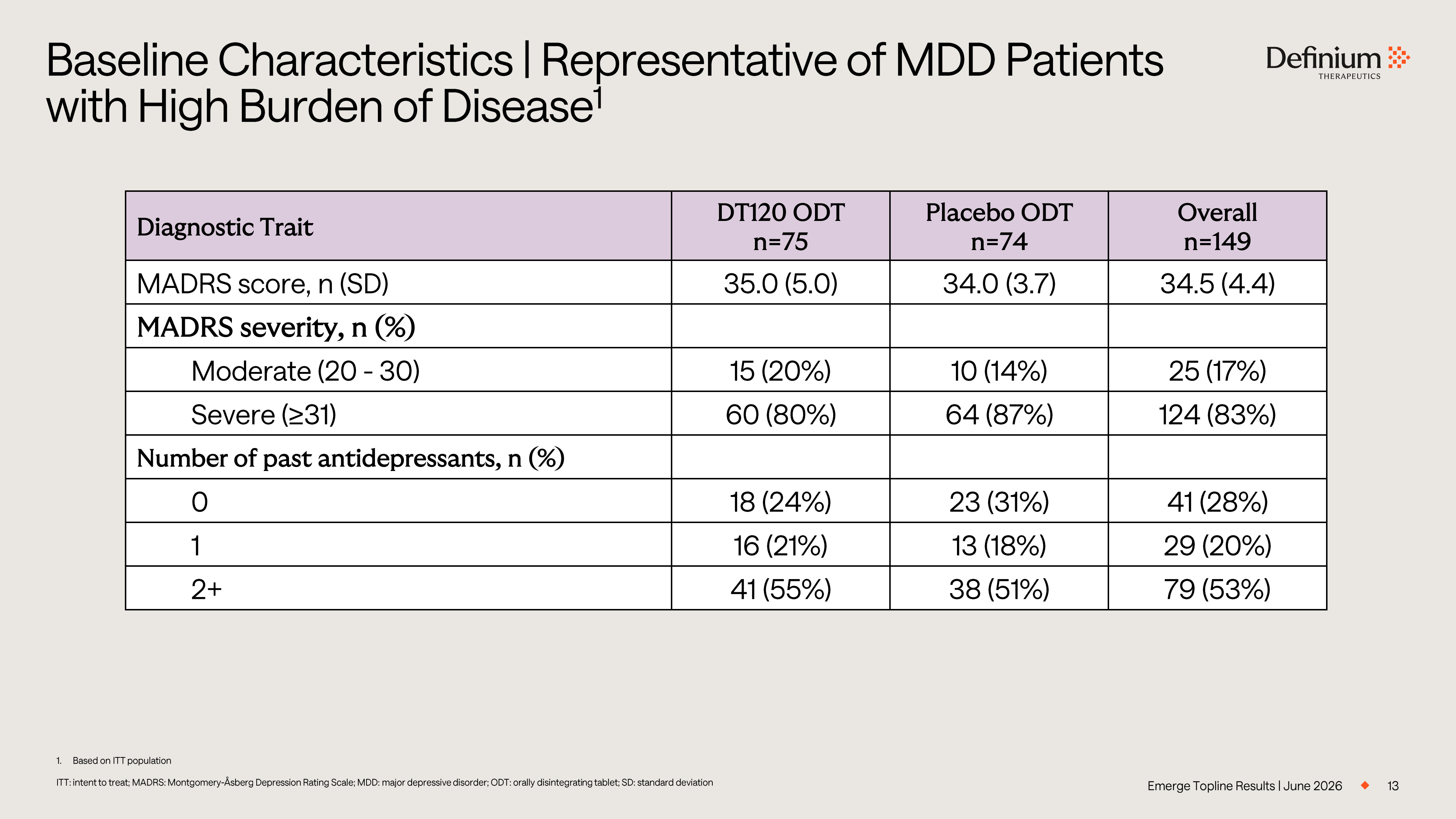
13 1. Based on ITT population ITT: intent to treat; MADRS: Montgomery - Åsberg Depression Rating Scale; MDD: major depressive disorder; ODT: orally disintegrati ng tablet; SD: standard deviation Baseline Characteristics | Representative of MDD Patients with High Burden of Disease 1 Emerge Topline Results | June 2026 Overall n=149 Placebo ODT n=74 DT120 ODT n=75 Diagnostic Trait 34.5 (4.4) 34.0 (3.7) 35.0 (5.0) MADRS score, n (SD) MADRS severity, n (%) 25 (17%) 10 (14%) 15 (20%) Moderate (20 - 30) 124 (83%) 64 (87%) 60 (80%) Severe (≥31) Number of past antidepressants, n (%) 41 (28%) 23 (31%) 18 (24%) 0 29 (20%) 13 (18%) 16 (21%) 1 79 (53%) 38 (51%) 41 (55%) 2+
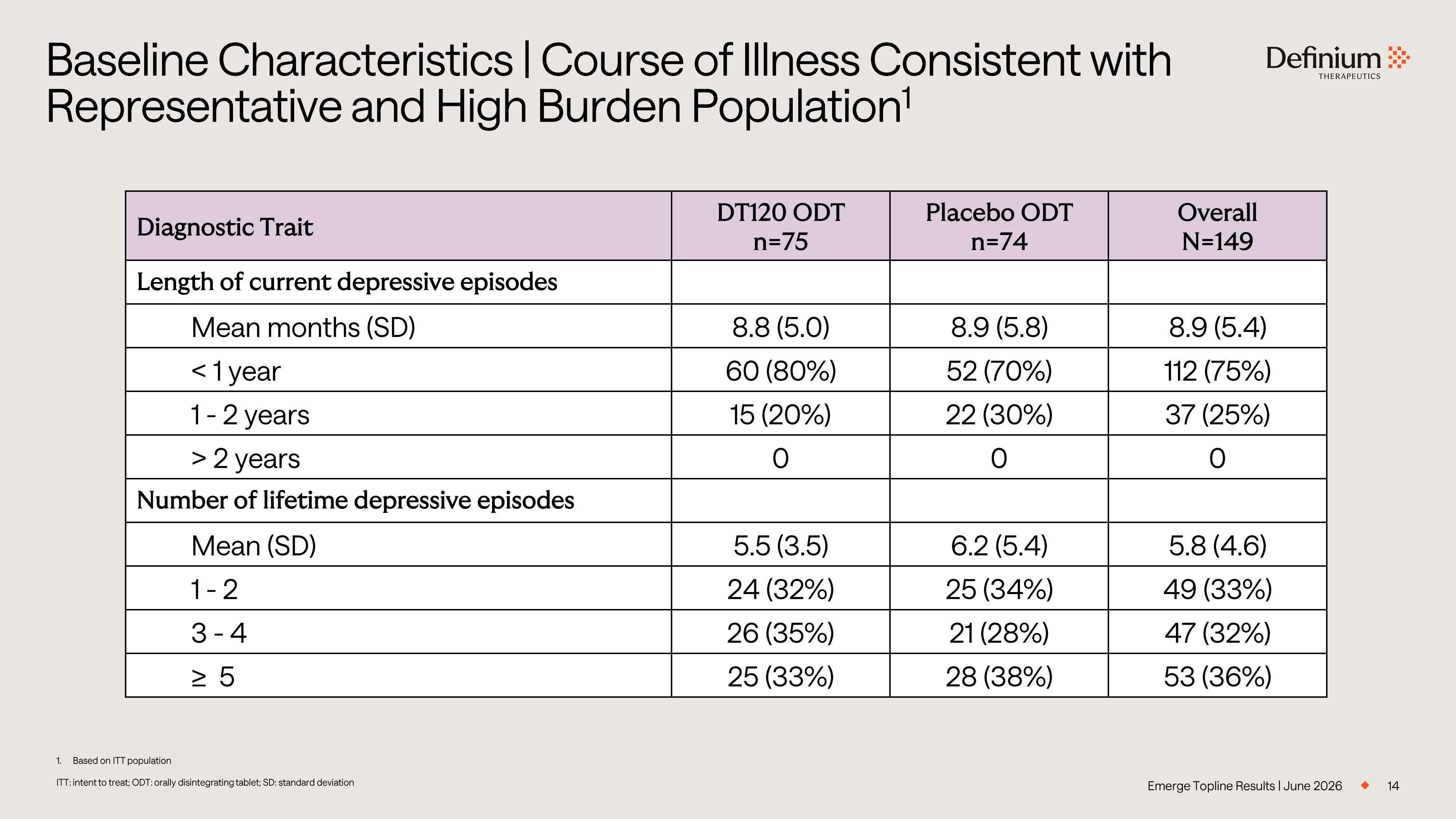
14 1. Based on ITT population ITT: intent to treat; ODT: orally disintegrating tablet; SD: standard deviation Baseline Characteristics | Course of Illness Consistent with Representative and High Burden Population 1 Emerge Topline Results | June 2026 Overall N=149 Placebo ODT n=74 DT120 ODT n=75 Diagnostic Trait Length of current depressive episodes 8.9 (5.4) 8.9 (5.8) 8.8 (5.0) Mean months (SD) 112 (75%) 52 (70%) 60 (80%) < 1 year 37 (25%) 22 (30%) 15 (20%) 1 - 2 years 0 0 0 > 2 years Number of lifetime depressive episodes 5.8 (4.6) 6.2 (5.4) 5.5 (3.5) Mean (SD) 49 (33%) 25 (34%) 24 (32%) 1 - 2 47 (32%) 21 (28%) 26 (35%) 3 - 4 53 (36%) 28 (38%) 25 (33%) ≥ 5
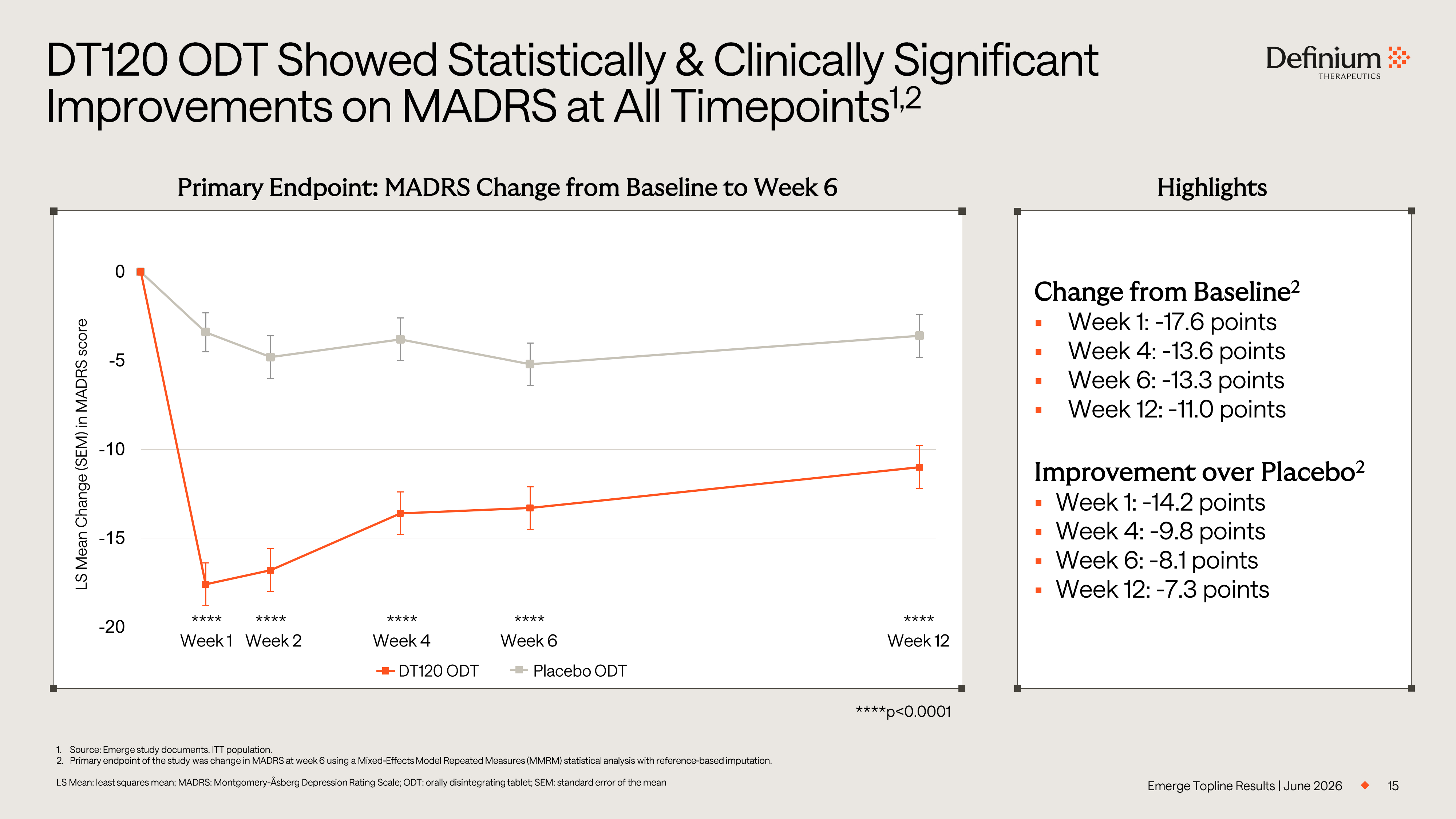
Primary Endpoint: MADRS Change from Baseline to Week 6 15 1. Source: Emerge study documents. ITT population. 2. Primary endpoint of the study was change in MADRS at week 6 using a Mixed - Effects Model Repeated Measures (MMRM) statistical ana lysis with reference - based imputation. LS Mean: least squares mean; MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegrating tablet; SEM: standard error of the mean DT120 ODT Showed Statistically & Clinically Significant Improvements on MADRS at All Timepoints 1,2 Emerge Topline Results | June 2026 -20 -15 -10 -5 0 LS Mean Change (SEM) in MADRS score **** **** **** **** **** Week 1 Week 2 Week 4 Week 6 Week 12 Change from Baseline 2 ▪ Week 1: - 17.6 points ▪ Week 4: - 13.6 points ▪ Week 6: - 13.3 points ▪ Week 12: - 11.0 points Improvement over Placebo 2 ▪ Week 1: - 14.2 points ▪ Week 4: - 9.8 points ▪ Week 6: - 8.1 points ▪ Week 12: - 7.3 points ****p<0.0001 Placebo ODT DT120 ODT Highlights
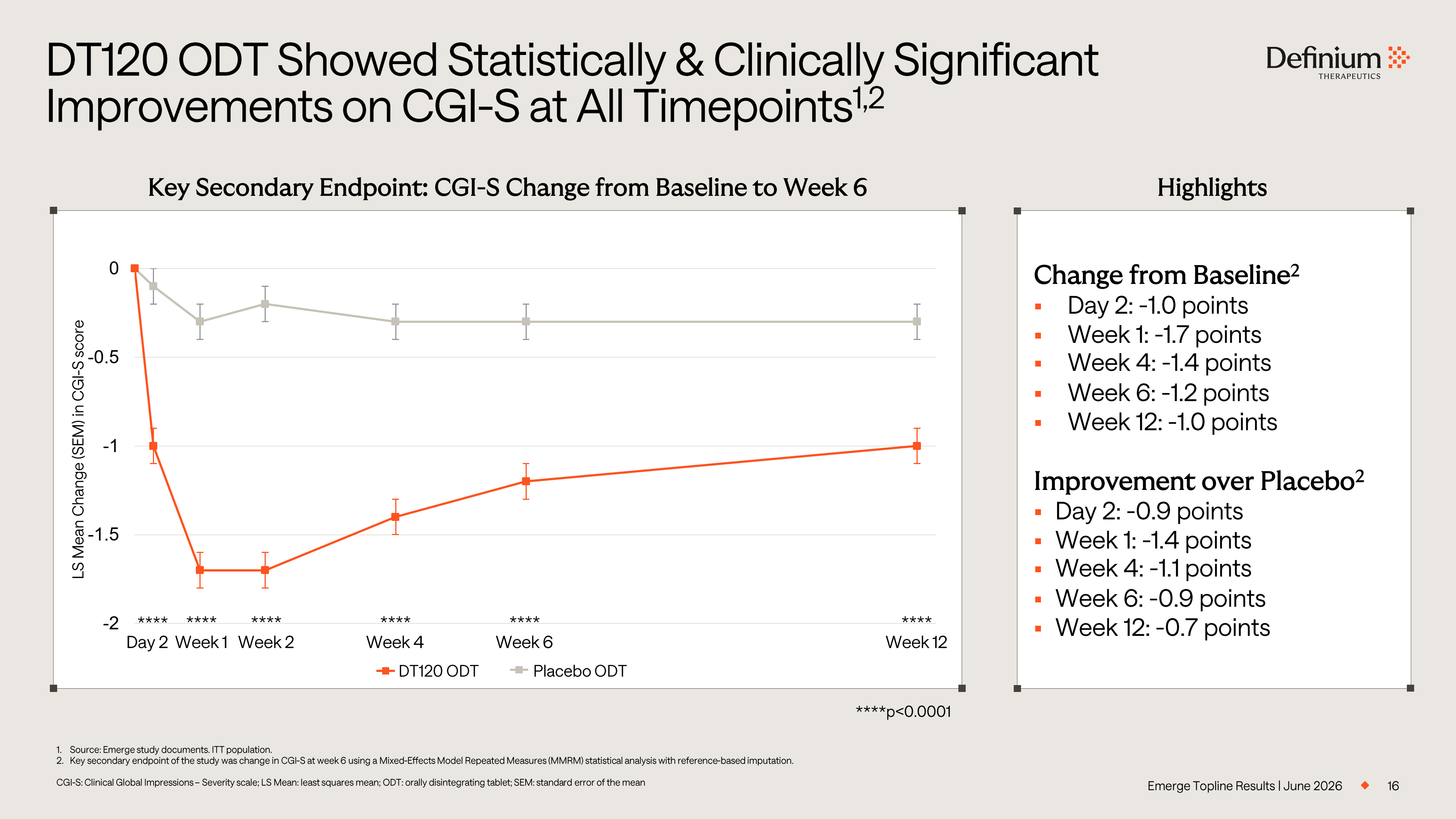
16 1. Source: Emerge study documents. ITT population. 2. Key secondary endpoint of the study was change in CGI - S at week 6 using a Mixed - Effects Model Repeated Measures (MMRM) statistic al analysis with reference - based imputation. CGI - S: Clinical Global Impressions – Severity scale; LS Mean: least squares mean; ODT: orally disintegrating tablet; SEM: standa rd error of the mean DT120 ODT Showed Statistically & Clinically Significant Improvements on CGI - S at All Timepoints 1,2 Emerge Topline Results | June 2026 Change from Baseline 2 ▪ Day 2: - 1.0 points ▪ Week 1: - 1.7 points ▪ Week 4: - 1.4 points ▪ Week 6: - 1.2 points ▪ Week 12: - 1.0 points Improvement over Placebo 2 ▪ Day 2: - 0.9 points ▪ Week 1: - 1.4 points ▪ Week 4: - 1.1 points ▪ Week 6: - 0.9 points ▪ Week 12: - 0.7 points -2 -1.5 -1 -0.5 0 LS Mean Change (SEM) in CGI - S score Placebo ODT DT120 ODT **** **** **** **** **** Week 1 Week 2 Week 4 Week 6 Week 12 **** Day 2 Key Secondary Endpoint: CGI - S Change from Baseline to Week 6 Highlights ****p<0.0001
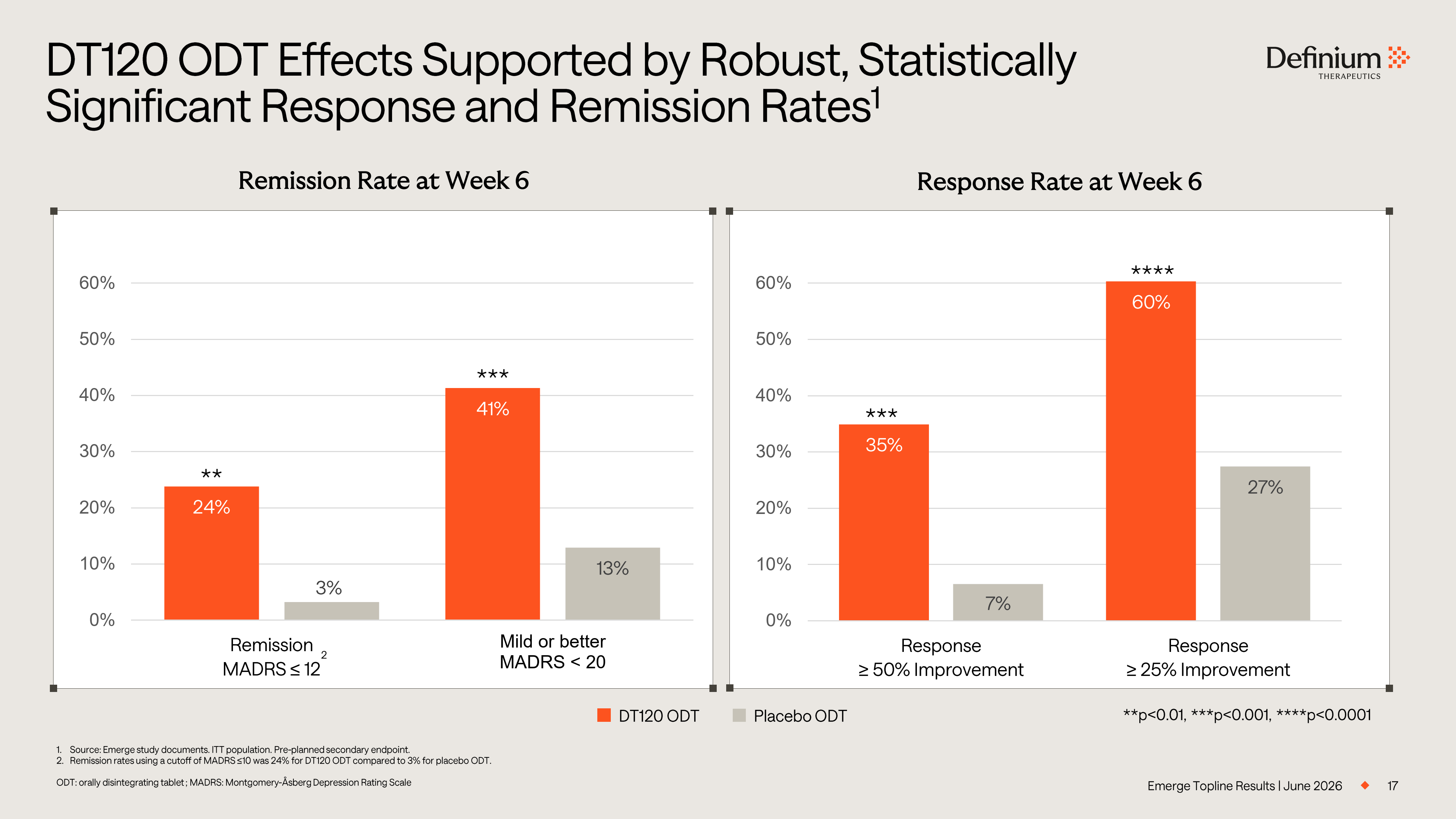
17 DT120 ODT Effects Supported by Robust, Statistically Significant Response and Remission Rates 1 Emerge Topline Results | June 2026 24% 41% 3% 13% 0% 10% 20% 30% 40% 50% 60% Remission MADRS ≤ 12 Mild or better MADRS < 20 Remission Rate at Week 6 35% 60% 7% 27% 0% 10% 20% 30% 40% 50% 60% Response ≥ 50% Improvement Response ≥ 25% Improvement Response Rate at Week 6 1. Source: Emerge study documents. ITT population. Pre - planned secondary endpoint. 2. Remission rates using a cutoff of MADRS ≤10 was 24% for DT120 ODT compared to 3% for placebo ODT. ODT: orally disintegrating tablet ; MADRS: Montgomery - Åsberg Depression Rating Scale **p<0.01, ***p<0.001, ****p<0.0001 **** *** ** *** Placebo ODT DT120 ODT 2
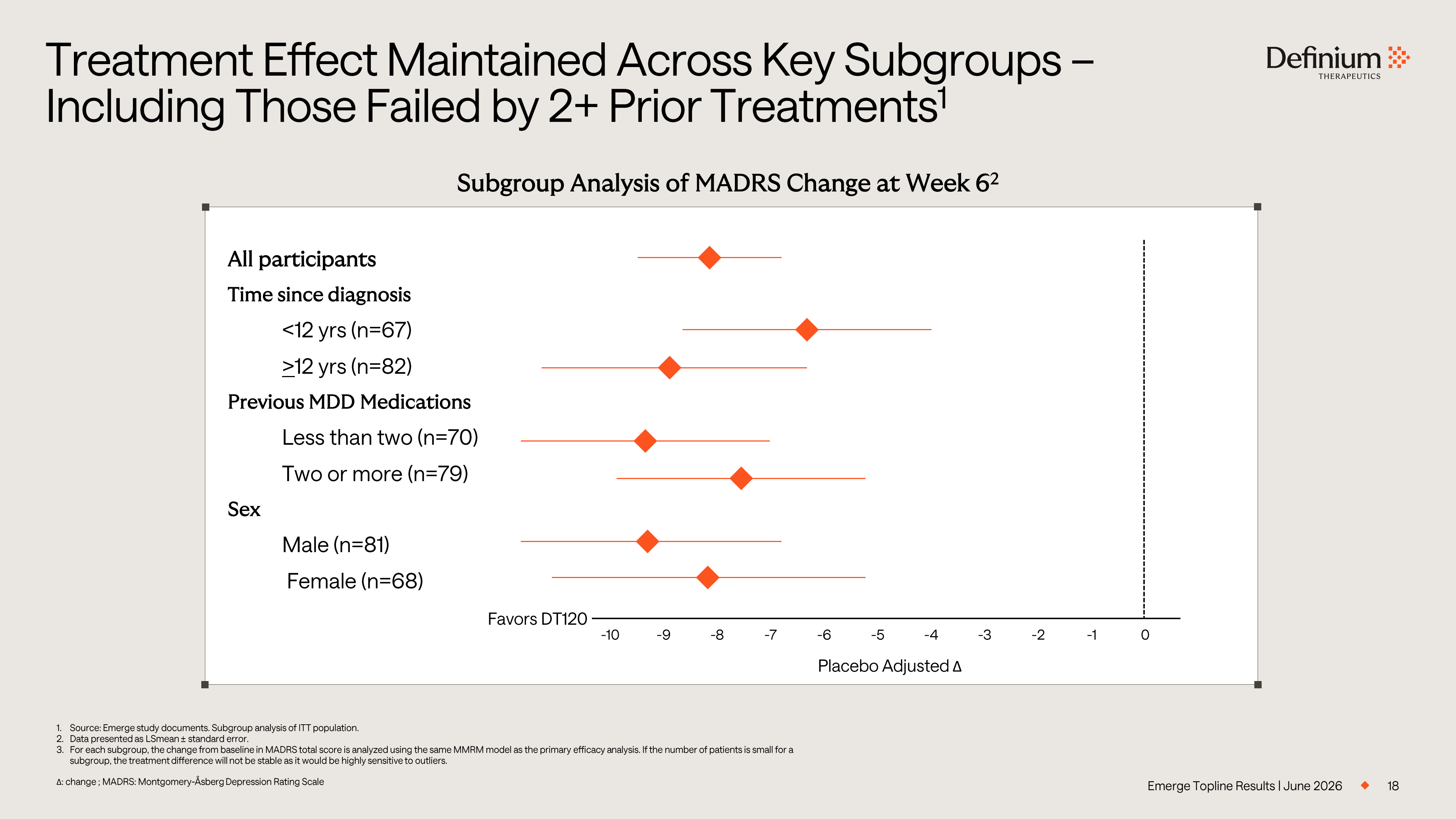
18 1. Source: Emerge study documents. Subgroup analysis of ITT population. 2. Data presented as LSmean ± standard error. 3. For each subgroup, the change from baseline in MADRS total score is analyzed using the same MMRM model as the primary efficac y a nalysis. If the number of patients is small for a subgroup, the treatment difference will not be stable as it would be highly sensitive to outliers. Δ : change ; MADRS: Montgomery - Åsberg Depression Rating Scale Treatment Effect Maintained Across Key Subgroups – Including Those Failed by 2+ Prior Treatments 1 Emerge Topline Results | June 2026 Placebo Adjusted Δ Subgroup Analysis of MADRS Change at Week 6 2 0 - 1 - 2 - 3 - 4 - 5 - 6 - 7 - 8 - 9 - 10 All participants Time since diagnosis <12 yrs (n=67) > 12 yrs (n=82) Previous MDD Medications Less than two (n=70) Two or more (n=79) Sex Male (n=81) Female (n=68) Favors DT120
DT120 ODT was Generally Well - Tolerated and Consistent with Known Pharmacology 1 1. Source: Emerge study documents. Safety population in study part A (through week 12). 2. The one severe adverse event that occurred was a recurrence of chronic back pain occurring approximately 6 weeks after dosing . 3. No serious adverse events have been observed in the Emerge study at the time of the data analysis. At the time of the analys is, a total of 4 serious adverse events have been recorded across all studies of DT120 ODT, including an SAE deemed treatment - related, resulting in an SAE rate of approximately 0.6% acros s studies and populations. 4. Suicidality assessment based on changes in C - SSRS. AE: adverse event; ODT: orally disintegrating tablet; SAE: serious adverse event; TEAE: treatment - emergent adverse event ▪ AE profile consistent with prior studies of DT120 ▪ 99% of adverse events (AEs) were mild - to - moderate in severity 2 ▪ Most treatment emergent AEs (TEAEs) occurred and resolved on dosing day ▪ No TEAEs led to study withdrawal Favorable tolerability profile No SAEs 3 No suicidal behavior or suicidality signal 4 ▪ No serious adverse events (SAEs) ▪ No suicidal or self - injurious behavior ▪ No indication of increased suicidal ideation or suicide - related risk 19 Emerge Topline Results | June 2026
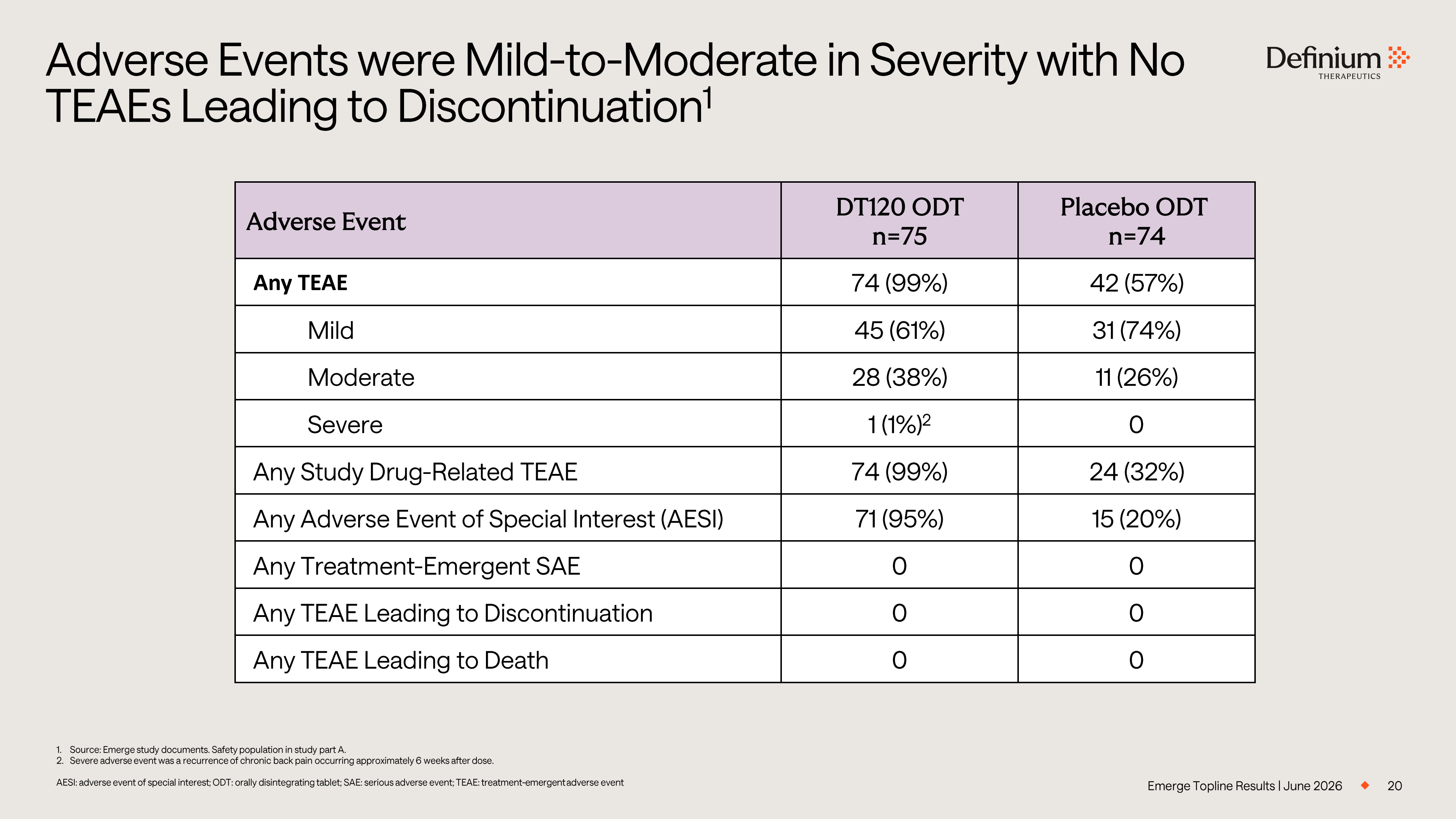
Emerge Topline Results | June 2026 20 Adverse Events were Mild - to - Moderate in Severity with No TEAEs Leading to Discontinuation 1 Placebo ODT n=74 DT120 ODT n=75 Adverse Event 42 (57%) 74 (99%) Any TEAE 31 (74%) 45 (61%) Mild 11 (26%) 28 (38%) Moderate 0 1 (1%) 2 Severe 24 (32%) 74 (99%) Any Study Drug - Related TEAE 15 (20%) 71 (95%) Any Adverse Event of Special Interest (AESI) 0 0 Any Treatment - Emergent SAE 0 0 Any TEAE Leading to Discontinuation 0 0 Any TEAE Leading to Death 1. Source: Emerge study documents. Safety population in study part A. 2. Severe adverse event was a recurrence of chronic back pain occurring approximately 6 weeks after dose. AESI: adverse event of special interest; ODT: orally disintegrating tablet; SAE: serious adverse event; TEAE: treatment - emergent adverse event
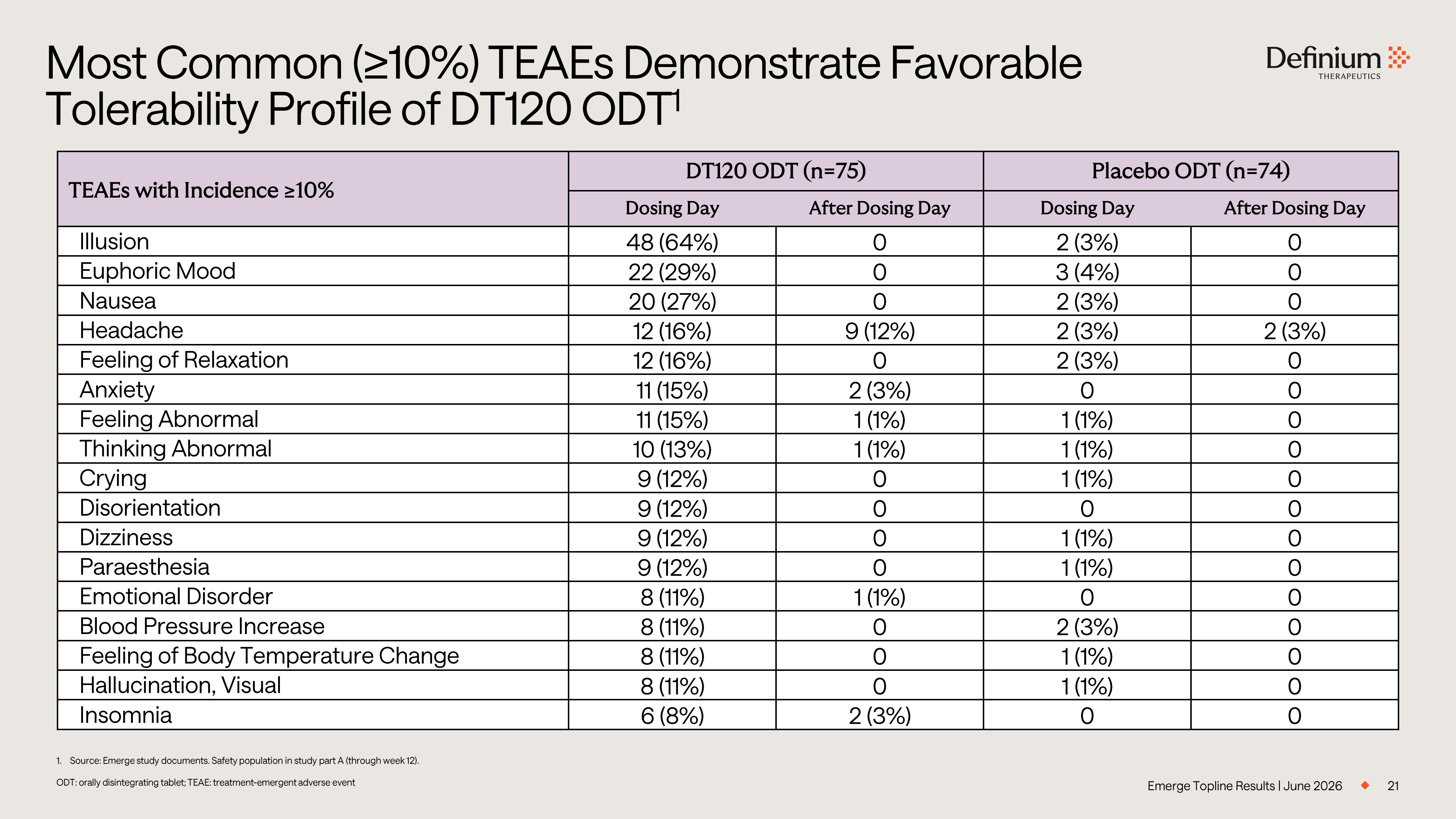
21 Most Common (≥10%) TEAEs Demonstrate Favorable Tolerability Profile of DT120 ODT 1 Emerge Topline Results | June 2026 Placebo ODT (n=74) DT120 ODT (n=75) TEAEs with Incidence ≥10% After Dosing Day Dosing Day After Dosing Day Dosing Day 0 2 (3%) 0 48 (64%) Illusion 0 3 (4%) 0 22 (29%) Euphoric Mood 0 2 (3%) 0 20 (27%) Nausea 2 (3%) 2 (3%) 9 (12%) 12 (16%) Headache 0 2 (3%) 0 12 (16%) Feeling of Relaxation 0 0 2 (3%) 11 (15%) Anxiety 0 1 (1%) 1 (1%) 11 (15%) Feeling Abnormal 0 1 (1%) 1 (1%) 10 (13%) Thinking Abnormal 0 1 (1%) 0 9 (12%) Crying 0 0 0 9 (12%) Disorientation 0 1 (1%) 0 9 (12%) Dizziness 0 1 (1%) 0 9 (12%) Paraesthesia 0 0 1 (1%) 8 (11%) Emotional Disorder 0 2 (3%) 0 8 (11%) Blood Pressure Increase 0 1 (1%) 0 8 (11%) Feeling of Body Temperature Change 0 1 (1%) 0 8 (11%) Hallucination, Visual 0 0 2 (3%) 6 (8%) Insomnia 1. Source: Emerge study documents. Safety population in study part A (through week 12). ODT: orally disintegrating tablet; TEAE: treatment - emergent adverse event
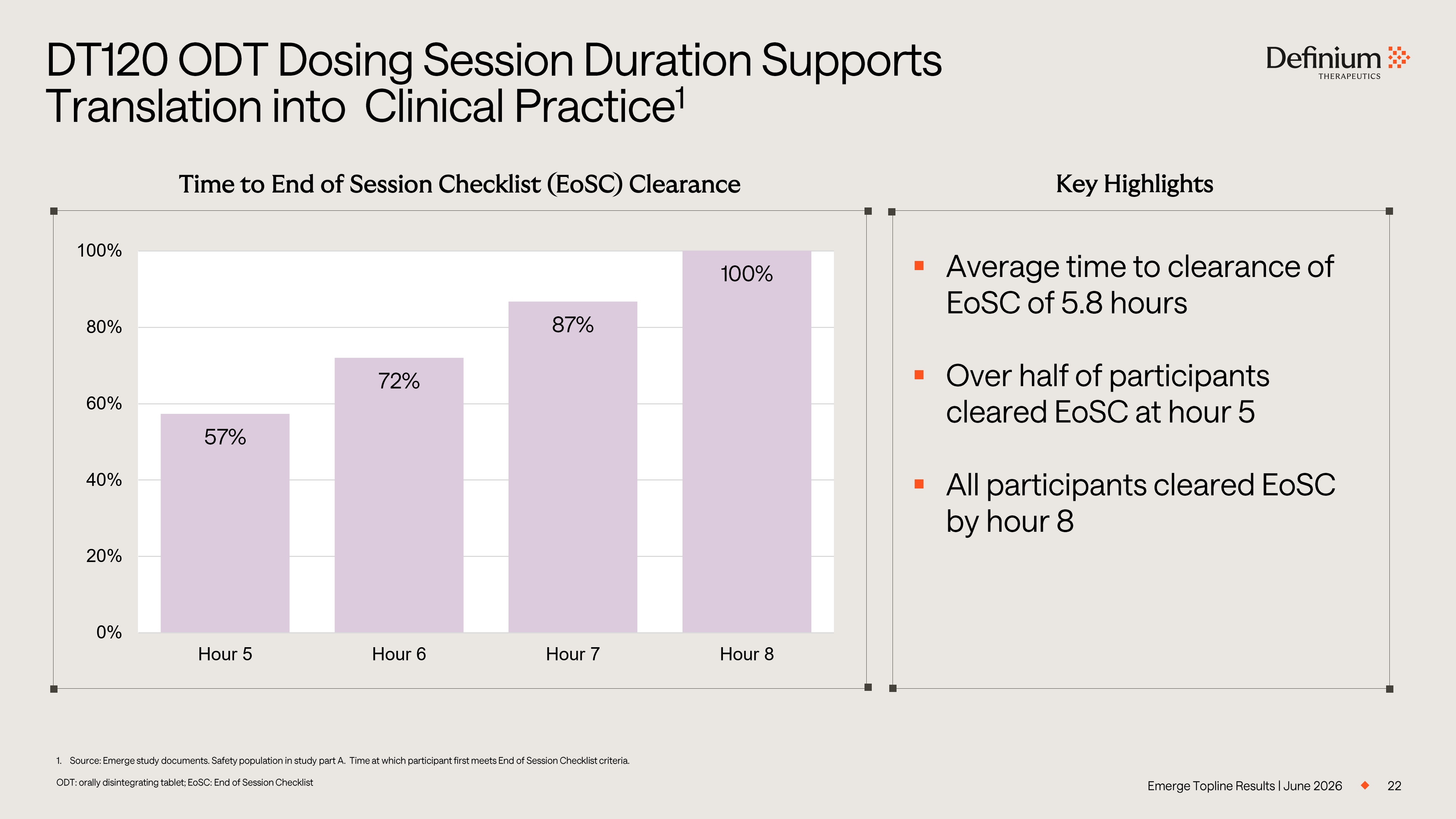
22 1. Source: Emerge study documents. Safety population in study part A. Time at which participant first meets End of Session Chec kli st criteria. ODT: orally disintegrating tablet; EoSC: End of Session Checklist DT120 ODT Dosing Session Duration Supports Translation into Clinical Practice 1 Emerge Topline Results | June 2026 57% 72% 87% 100% 0% 20% 40% 60% 80% 100% Hour 5 Hour 6 Hour 7 Hour 8 Time to End of Session Checklist (EoSC) Clearance Key Highlights ▪ Average time to clearance of EoSC of 5.8 hours ▪ Over half of participants cleared EoSC at hour 5 ▪ All participants cleared EoSC by hour 8
Phase 3 Emerge Topline Results Part B – Interim Analysis Dan Karlin, MD Chief Medical Officer
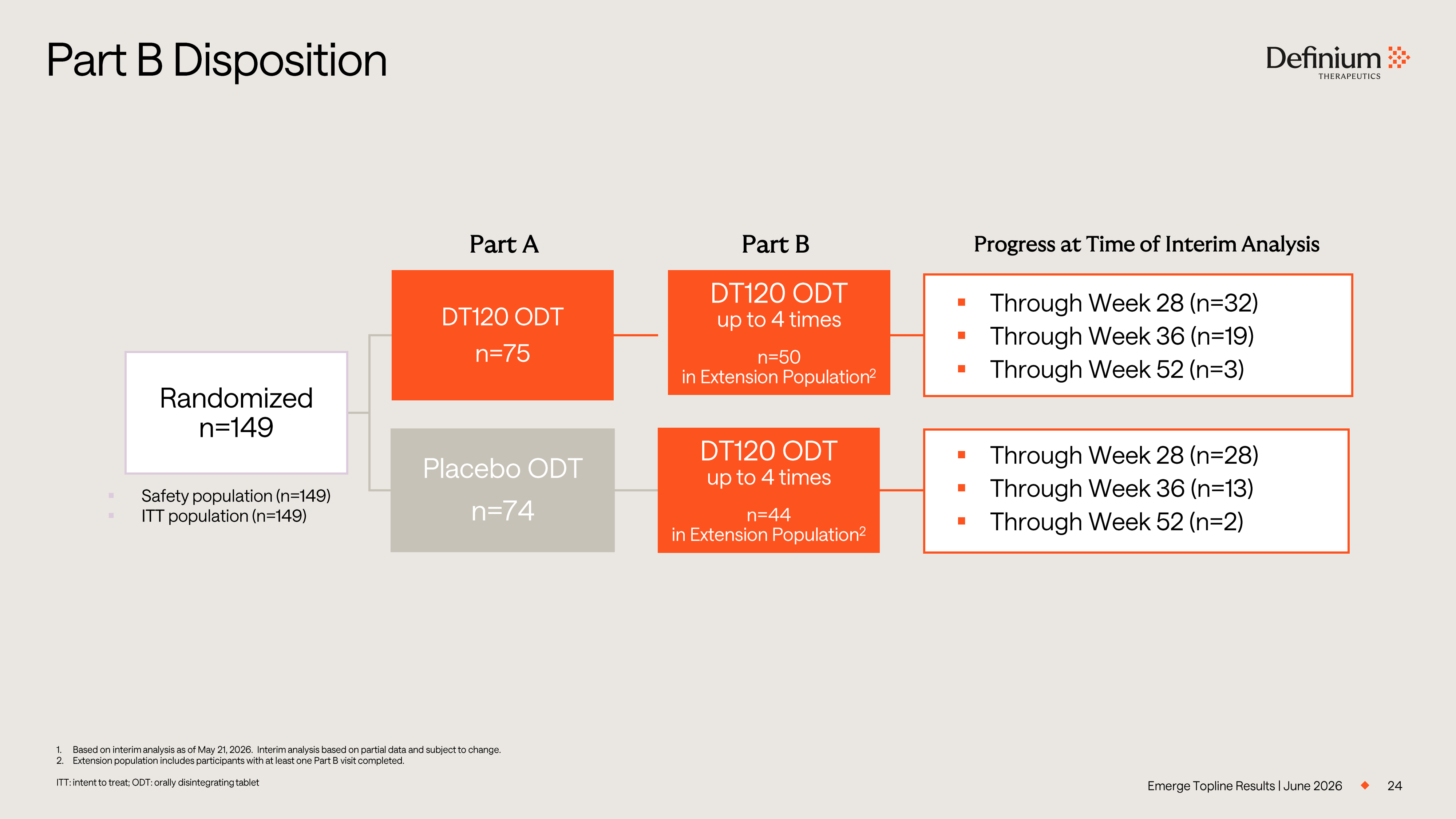
24 1. Based on interim analysis as of May 21, 2026. Interim analysis based on partial data and subject to change. 2. Extension population includes participants with at least one Part B visit completed. ITT: intent to treat; ODT: orally disintegrating tablet Part B Disposition Emerge Topline Results | June 2026 ▪ Safety population (n=149) ▪ ITT population (n=149) Part A Progress at Time of Interim Analysis Part B Randomized n=149 DT120 ODT n=75 Placebo ODT n=74 DT120 ODT up to 4 times n=44 in Extension Population 2 ▪ Through Week 28 (n=32) ▪ Through Week 36 (n=19) ▪ Through Week 52 (n=3) ▪ Through Week 28 (n=28) ▪ Through Week 36 (n=13) ▪ Through Week 52 (n=2) DT120 ODT up to 4 times n=50 in Extension Population 2
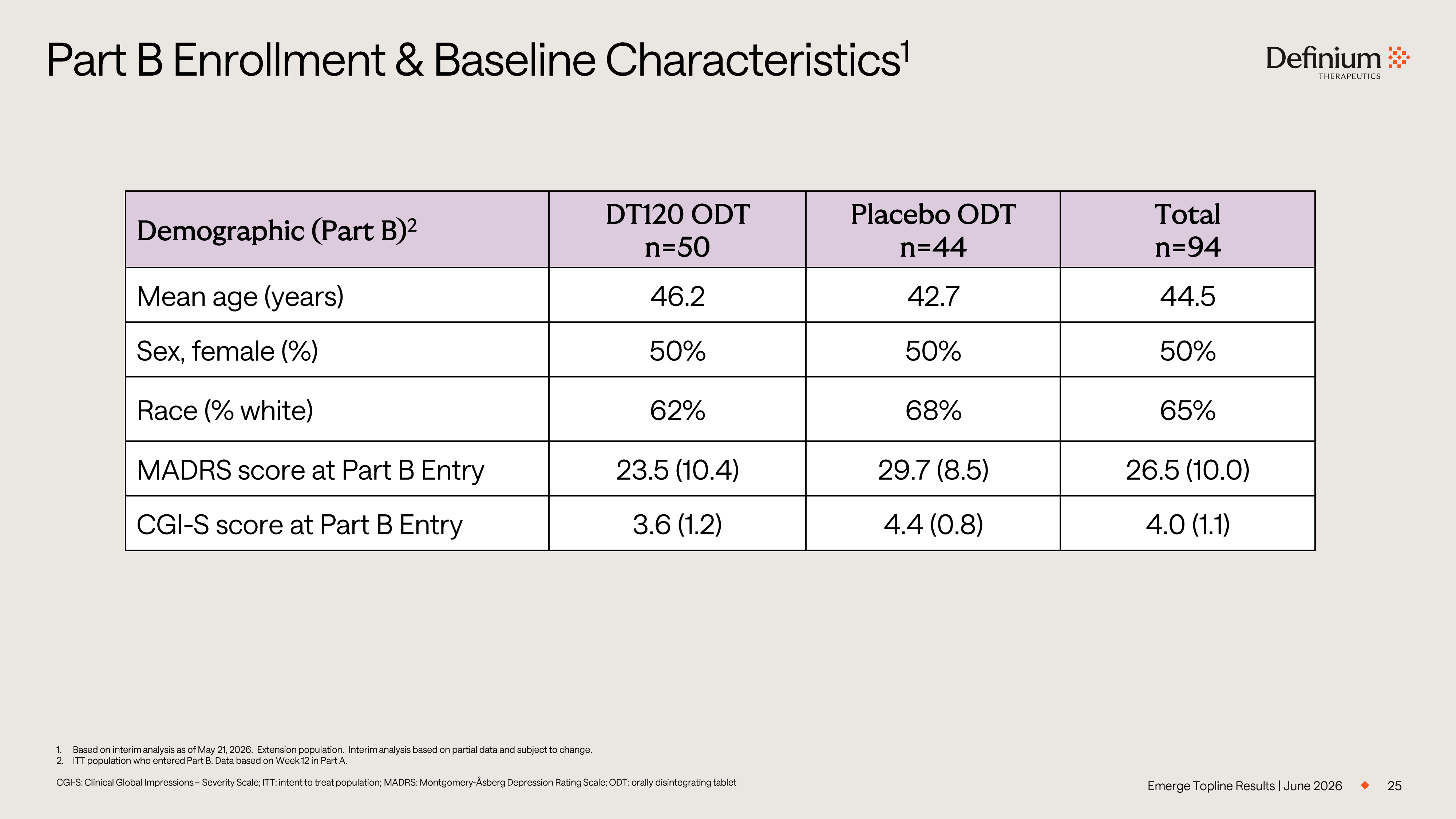
25 1. Based on interim analysis as of May 21, 2026. Extension population. Interim analysis based on partial data and subject to c han ge. 2. ITT population who entered Part B. Data based on Week 12 in Part A. CGI - S: Clinical Global Impressions – Severity Scale; ITT: intent to treat population; MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegrating tablet Part B Enrollment & Baseline Characteristics 1 Emerge Topline Results | June 2026 Total n=94 Placebo ODT n=44 DT120 ODT n=50 Demographic (Part B) 2 44.5 42.7 46.2 Mean age (years) 50% 50% 50% Sex, female (%) 65% 68% 62% Race (% white) 26.5 (10.0) 29.7 (8.5) 23.5 (10.4) MADRS score at Part B Entry 4.0 (1.1) 4.4 (0.8) 3.6 (1.2) CGI - S score at Part B Entry
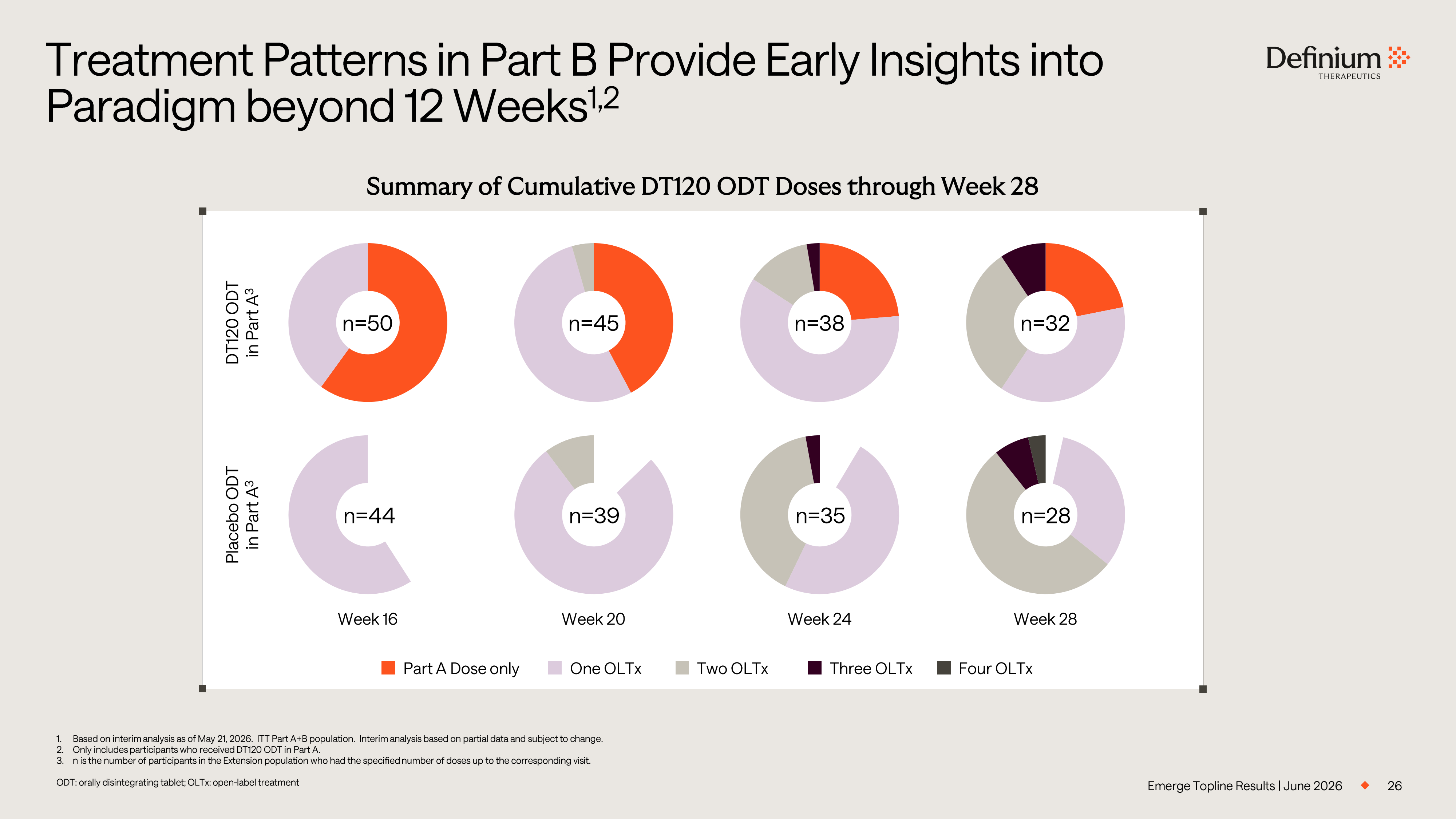
26 1. Based on interim analysis as of May 21, 2026. ITT Part A+B population. Interim analysis based on partial data and subject t o c hange. 2. Only includes participants who received DT120 ODT in Part A. 3. n is the number of participants in the Extension population who had the specified number of doses up to the corresponding vis it. ODT: orally disintegrating tablet; OLTx: open - label treatment Treatment Patterns in Part B Provide Early Insights into Paradigm beyond 12 Weeks 1,2 Emerge Topline Results | June 2026 Summary of Cumulative DT120 ODT Doses through Week 28 Week 28 Week 24 Week 20 Week 16 n=50 n=45 n=38 n=32 DT120 ODT in Part A 3 n=44 n=39 n=35 n=28 Placebo ODT in Part A 3 Part A Dose only One OLTx Two OLTx Three OLTx Four OLTx
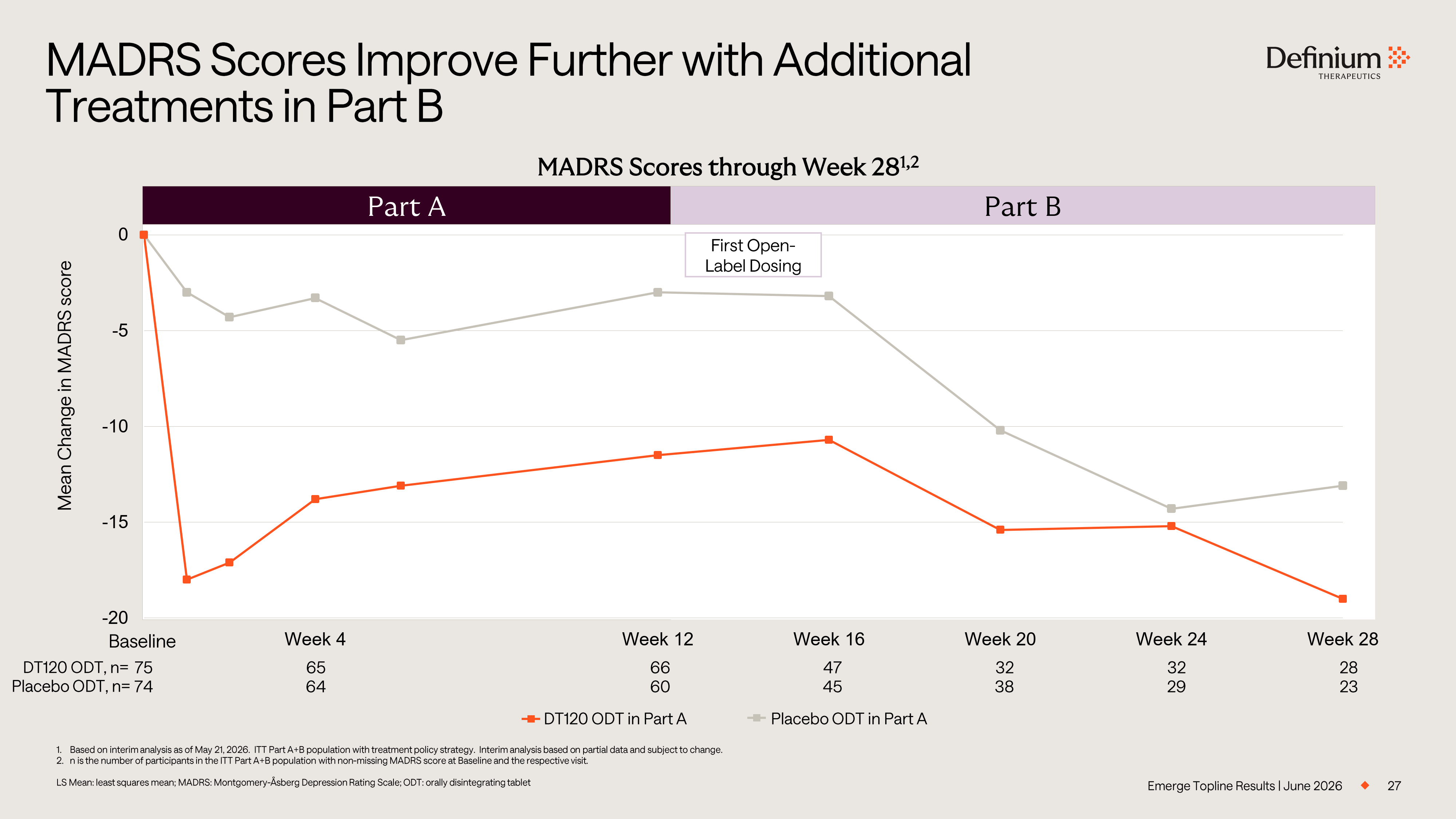
27 1. Based on interim analysis as of May 21, 2026. ITT Part A+B population with treatment policy strategy. Interim analysis base d o n partial data and subject to change. 2. n is the number of participants in the ITT Part A+B population with non - missing MADRS score at Baseline and the respective visit . LS Mean: least squares mean; MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegrating tablet MADRS Scores Improve Further with Additional Treatments in Part B Emerge Topline Results | June 2026 -20 -15 -10 -5 0 Week 0 Week 4 Week 8 Week 12 Week 16 Week 20 Week 24 Week 28 Mean Change in MADRS score MADRS Scores through Week 28 1,2 DT120 ODT in Part A Placebo ODT in Part A Part A Part B 28 32 32 47 66 65 75 23 29 38 45 60 64 74 DT120 ODT, n= Baseline Placebo ODT, n= First Open - Label Dosing
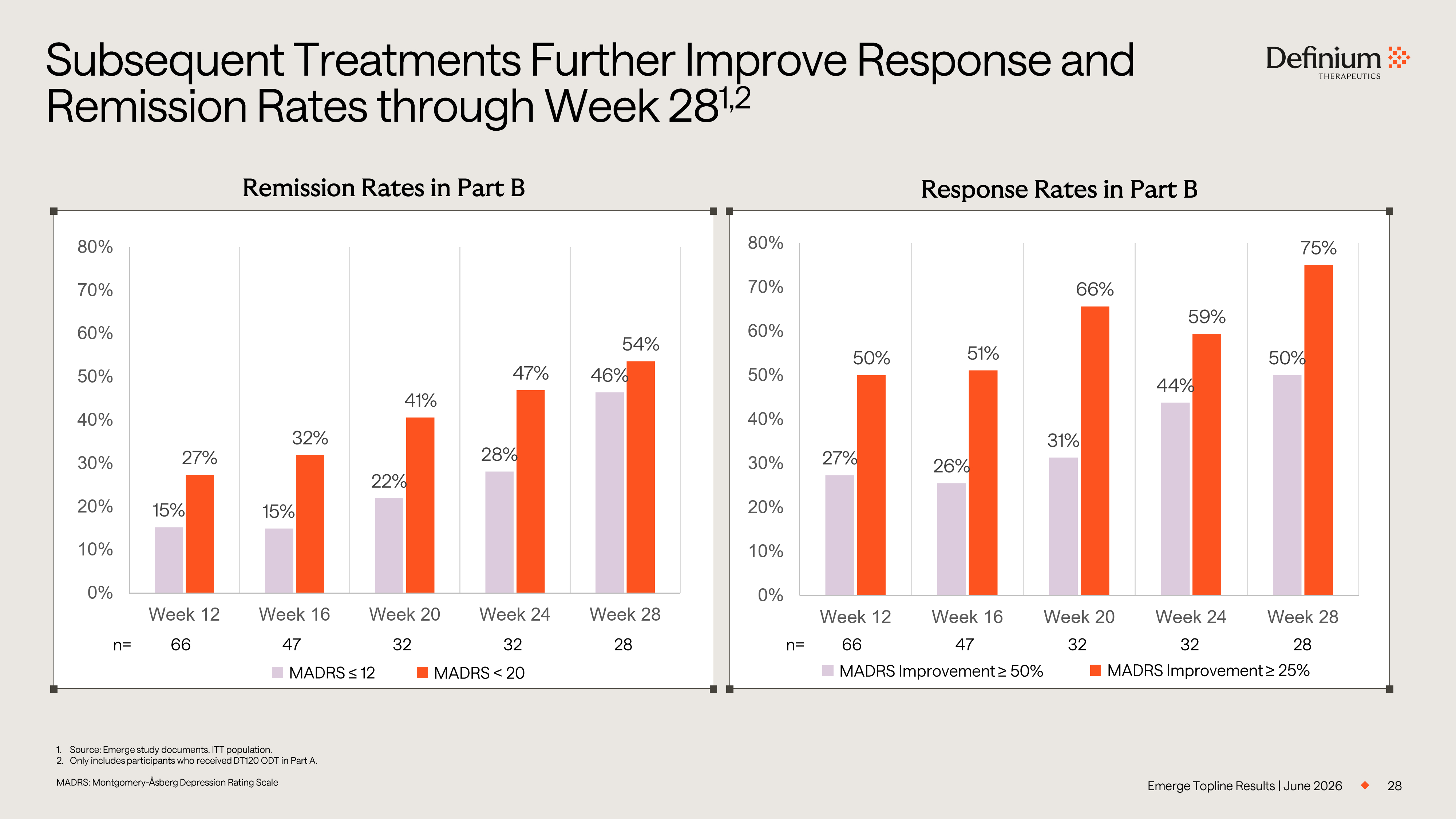
28 Subsequent Treatments Further Improve Response and Remission Rates through Week 28 1,2 Emerge Topline Results | June 2026 Remission Rates in Part B Response Rates in Part B 1. Source: Emerge study documents. ITT population. 2. Only includes participants who received DT120 ODT in Part A. MADRS: Montgomery - Åsberg Depression Rating Scale MADRS Improvement ≥ 50% MADRS Improvement ≥ 25% 27% 26% 31% 44% 50% 50% 51% 66% 59% 75% 0% 10% 20% 30% 40% 50% 60% 70% 80% Week 12 Week 16 Week 20 Week 24 Week 28 15% 15% 22% 28% 46% 27% 32% 41% 47% 54% 0% 10% 20% 30% 40% 50% 60% 70% 80% Week 12 Week 16 Week 20 Week 24 Week 28 MADRS ≤ 12 MADRS < 20 28 32 32 47 66 n= 28 32 32 47 66 n=
Next Steps Rob Barrow Chief Executive Officer
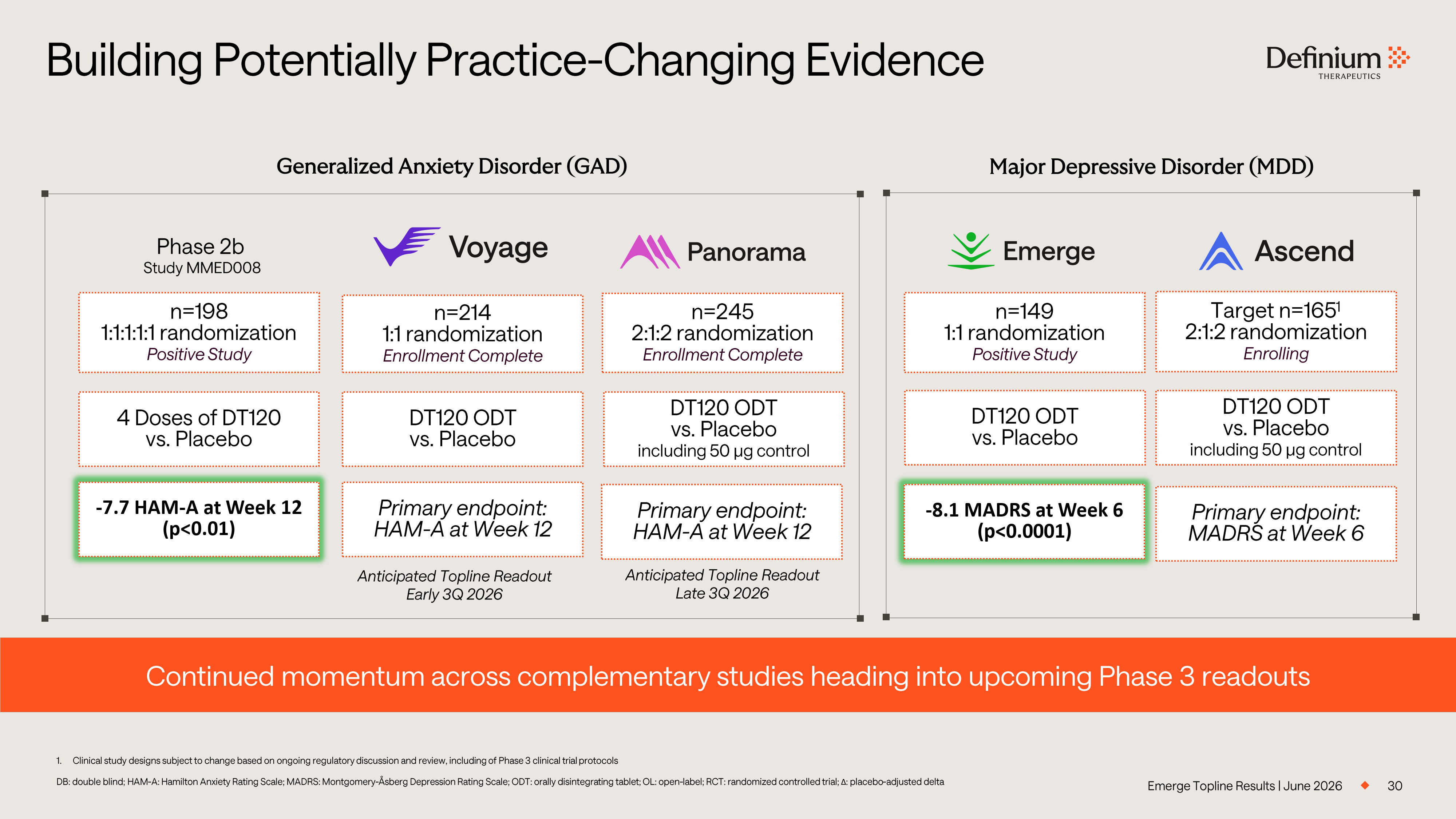
Emerge Topline Results | June 2026 30 Building Potentially Practice - Changing Evidence 1. Clinical study designs subject to change based on ongoing regulatory discussion and review, including of Phase 3 clinical tri al protocols DB: double blind; HAM - A: Hamilton Anxiety Rating Scale; MADRS: Montgomery - Åsberg Depression Rating Scale; ODT: orally disintegra ting tablet; OL: open - label; RCT: randomized controlled trial; Δ : placebo - adjusted delta Generalized Anxiety Disorder (GAD) Major Depressive Disorder (MDD) n=214 1 :1 randomization Enrollment Complete n=245 2:1:2 randomization Enrollment Complete n=149 1:1 randomization Positive Study Target n=165 1 2:1:2 randomization Enrolling Anticipated Topline Readout Early 3Q 2026 Anticipated Topline Readout Late 3Q 2026 n=198 1 :1:1:1:1 randomization Positive Study Phase 2b 4 Doses of DT120 vs. Placebo DT120 ODT vs. Placebo - 7.7 HAM - A at Week 12 (p<0.01) Continued momentum across complementary studies heading into upcoming Phase 3 readouts Primary endpoint: HAM - A at Week 12 Primary endpoint: HAM - A at Week 12 DT120 ODT vs. Placebo including 50 µg control - 8.1 MADRS at Week 6 (p<0.0001) DT120 ODT vs. Placebo DT120 ODT vs. Placebo including 50 µg control Primary endpoint: MADRS at Week 6 Study MMED008
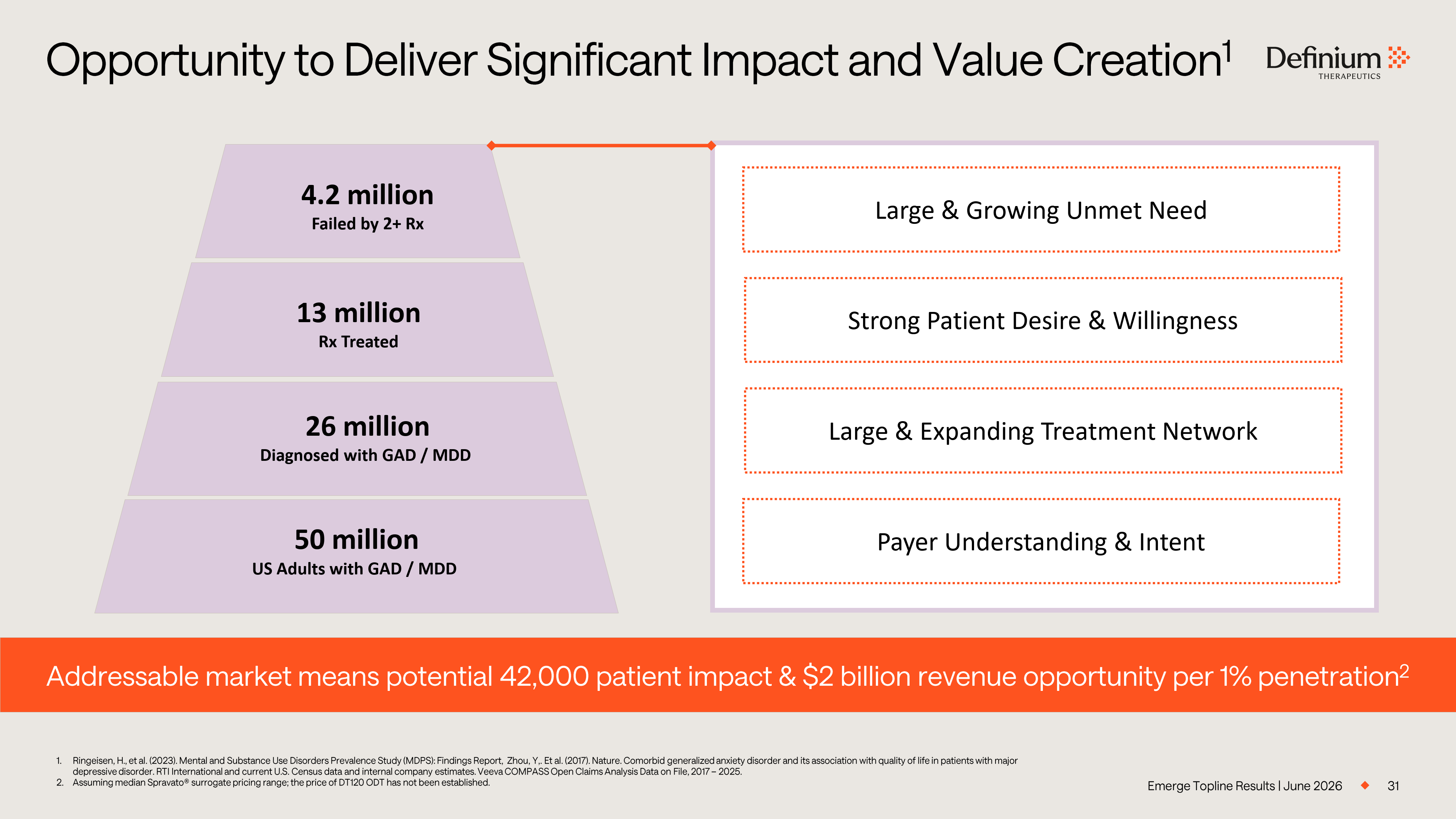
Emerge Topline Results | June 2026 31 Opportunity to Deliver Significant Impact and Value Creation 1 1. Ringeisen, H., et al. (2023). Mental and Substance Use Disorders Prevalence Study (MDPS): Findings Report, Zhou, Y,. Et al. (20 17). Nature. Comorbid generalized anxiety disorder and its association with quality of life in patients with major depressive disorder. RTI International and current U.S. Census data and internal company estimates. Veeva COMPASS Open Claims An alysis Data on File, 2017 – 2025. 2. Assuming median Spravato® surrogate pricing range; the price of DT120 ODT has not been established. Addressable market means potential 42,000 patient impact & $2 billion revenue opportunity per 1% penetration 2 50 million US Adults with GAD / MDD 26 million Diagnosed with GAD / MDD 13 million Rx Treated 4.2 million Failed by 2+ Rx Strong Patient Desire & Willingness Large & Expanding Treatment Network Payer Understanding & Intent Large & Growing Unmet Need
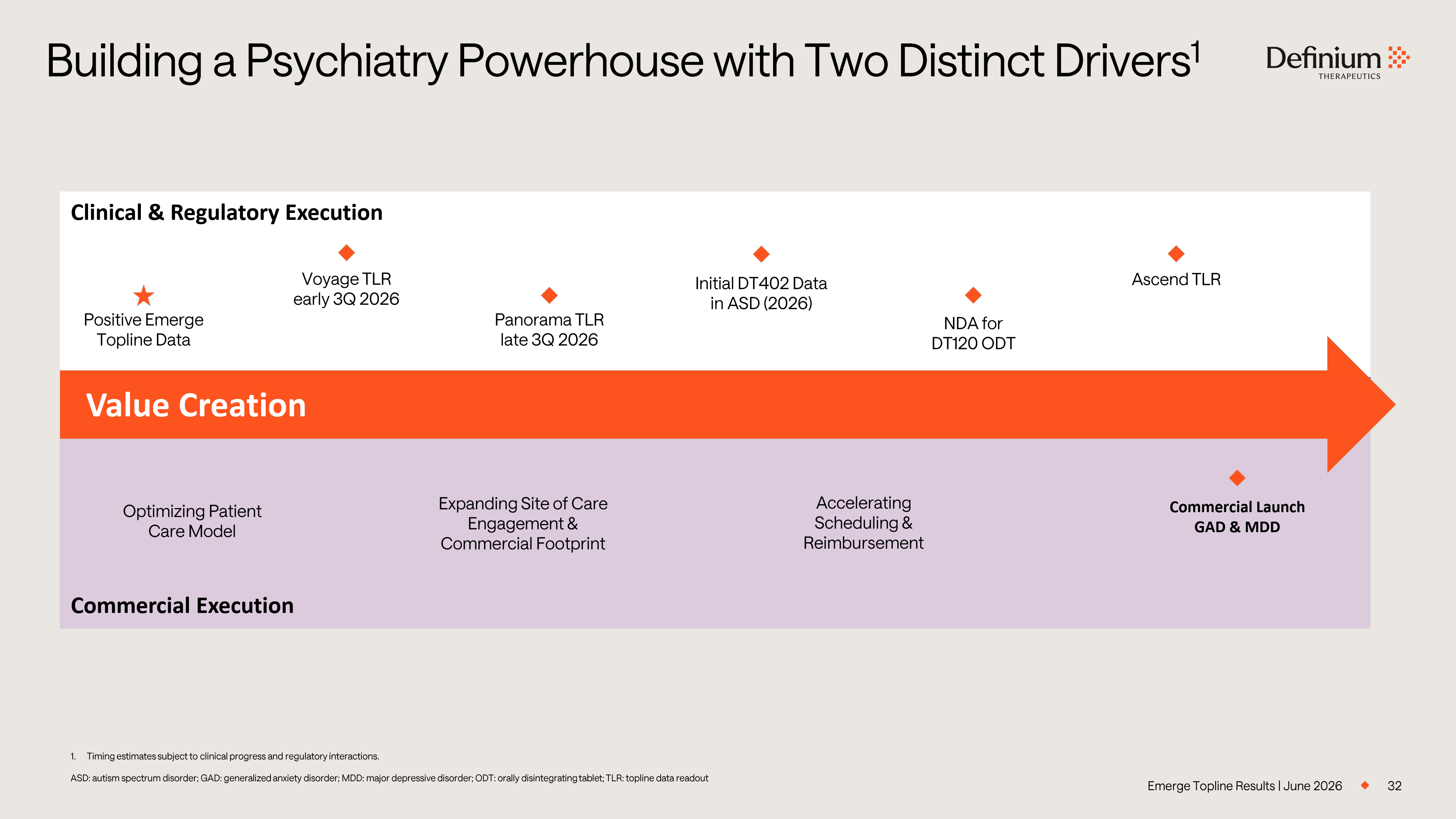
32 Building a Psychiatry Powerhouse with Two Distinct Drivers 1 1. Timing estimates subject to clinical progress and regulatory interactions. ASD: autism spectrum disorder; GAD: generalized anxiety disorder; MDD: major depressive disorder; ODT: orally disintegrating tab let; TLR: topline data readout Clinical & Regulatory Execution 2028 2027 2026 Commercial Execution Value Creation Expanding Site of Care Engagement & Commercial Footprint Accelerating Scheduling & Reimbursement Optimizing Patient Care Model Voyage TLR early 3Q 2026 Initial DT402 Data in ASD (2026) Panorama TLR late 3Q 2026 NDA for DT120 ODT Ascend TLR Commercial Launch GAD & MDD Emerge Topline Results | June 2026 Positive Emerge Topline Data