.2
© 2026 | Proprietary | MoonLake TX MoonLake Immunotherapeutics Investor Day June 22nd, 2026

© 2026 | Proprietary | MoonLake TX Source: Welcome to our Investor Day MoonLake Corporate Strategy Agenda Sub-topics Topic Speaker Timing Proposed Label Update on BLA progress BLA strategy Jorge 20 mins Welcome MLTX & SLK summary Introduction Jorge 10 mins Final Week 52 Phase 3 VELA data Update on VELA-TEEN data Final data from the VELA program in HS Kristian 30 mins Date: June 22nd, 2026 Time: 8.00 am EST Update on HS market view Why MLTX can win commercially in HS Commercializing SLK in HS Matthias 10 mins 2 Closing remarks Jorge 5 mins Summary & Guidance on H2 2026 Expectations for IZAR-1 readout The presentation will be followed by a short Q&A session – please submit your questions via the dedicated Q&A function in the portal, in case of issues please e-mail ir@moonlaketx.com
Source: © 2026 | Proprietary | MoonLake TX MoonLake Legal 3 Disclaimer Forward Looking Statements Certain statements in this presentation may constitute "forward-looking statements" within the meaning of the U.S. Private Securities Litigation Reform Act of 1995. Forward-looking statements include, but are not limited to, statements regarding our expectations, hopes, beliefs, intentions or strategies regarding the future including, without limitation, statements regarding: plans for clinical trials and regulatory submissions, including expected BLA submissions for SLK; the anticipated timing of the results from those trials; the anticipated timing of BLA submission, review and approval; the proposed FDA label and anticipated differentiation potential for the FDA label for SLK; potential market opportunities, estimates of market size, and estimates of market growth; potential indications; the timing of regulatory meetings; the occurrence and timing of market engagement; expectations regarding the time period over which our capital resources will be sufficient to fund our anticipated operations; the timing and likelihood of success, plans and objectives of management for future operations and future results of anticipated product development and commercialization efforts; and effects on liquidity and capital resources, including cash position. In addition, any statements that refer to projections, forecasts, or other characterizations of future events or circumstances, including any underlying assumptions, are forward-looking statements. The words "anticipate", "believe", continue", "could", "estimate", "expect", "intend", "may", "might", "plan", "possible", "potential", "predict", "project", "should", " strive", "would" and similar expressions may identify forward-looking statements, but the absence of these words does not mean that such statement is not forward looking. Forward-looking statements are based on current expectations and assumptions that, while we and our management consider reasonable, as the case may be, are inherently uncertain. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Factors that may cause actual results to differ materially from current expectations include, but are not limited to, various factors beyond management's control including general economic conditions and other risks, uncertainties and factors set forth in the section entitled "Risk Factors" and "Note on Forward-Looking Statements" in our Annual Report on Form 10-K that was filed with the U.S. Securities and Exchange Commission (the "SEC") on February 25, 2026, Quarterly Report on Form 10-Q for the quarter ended March 31, 2026, as filed with the SEC on May 11, 2026, as well as factors associated with companies, such as MoonLake Immunotherapeutics, that operate in the biopharma industry. Nothing in this presentation should be regarded as a representation by any person that the forward-looking statements set forth herein will be achieved or that any of the contemplated results of such forward-looking statements will be achieved. You should not place undue reliance on forward-looking statements in this presentation, which speak only as of the date they are made and are qualified in their entirety by reference to the cautionary statements herein. We neither undertake nor accept any duty to release publicly any updates or revisions to any forward-looking statements to reflect any change in our expectations or in the events, conditions or circumstances on which any such statement is based. This presentation does not purport to summarize all of the conditions, risks and other attributes of MoonLake Immunotherapeutics. Industry and Market Data Certain information contained in this presentation relates to or is based on studies, publications, surveys and our own internal estimates and research. In this presentation, we rely on, and refer to, publicly available information and statistics regarding market participants in the sector in which we compete and other industry data. Any comparison of us to any other entity assumes the reliability of the information available to us. We obtained this information and statistics from third-party sources, including reports by market research firms and company filings. In addition, all of the market data included in this presentation involve a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our internal research is reliable, such research has not been verified by any independent source and we have not independently verified the information. Trademarks This presentation may contain trademarks, service marks, trade names and copyrights of other companies, which are the property of their respective owners. Solely for convenience, some of the trademarks, service marks, trade names and copyrights referred to in this presentation may be listed without the TM, SM © or ® symbols, but we will assert, to the fullest extent under applicable law, the rights of the applicable owners, if any, to these trademarks, service marks, trade names and copyrights.
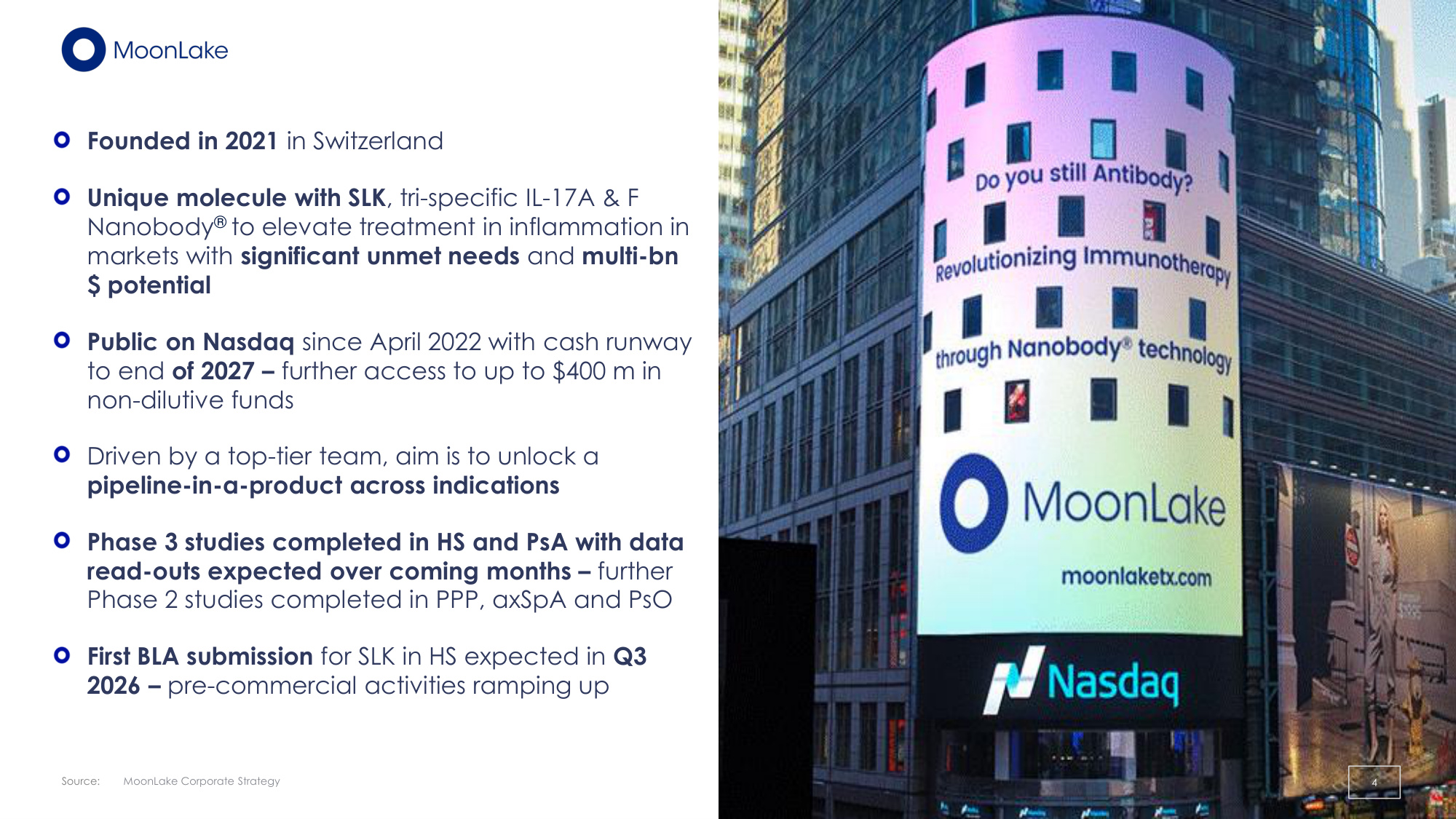
© 2026 | Proprietary | MoonLake TX Source: Founded in 2021 in Switzerland Unique molecule with SLK, tri-specific IL-17A & F Nanobody® to elevate treatment in inflammation in markets with significant unmet needs and multi-bn $ potential Public on Nasdaq since April 2022 with cash runway to end of 2027 – further access to up to $400 m in non-dilutive funds Driven by a top-tier team, aim is to unlock a pipeline-in-a-product across indications Phase 3 studies completed in HS and PsA with data read-outs expected over coming months – further Phase 2 studies completed in PPP, axSpA and PsO First BLA submission for SLK in HS expected in Q3 2026 – pre-commercial activities ramping up MoonLake Corporate Strategy 4
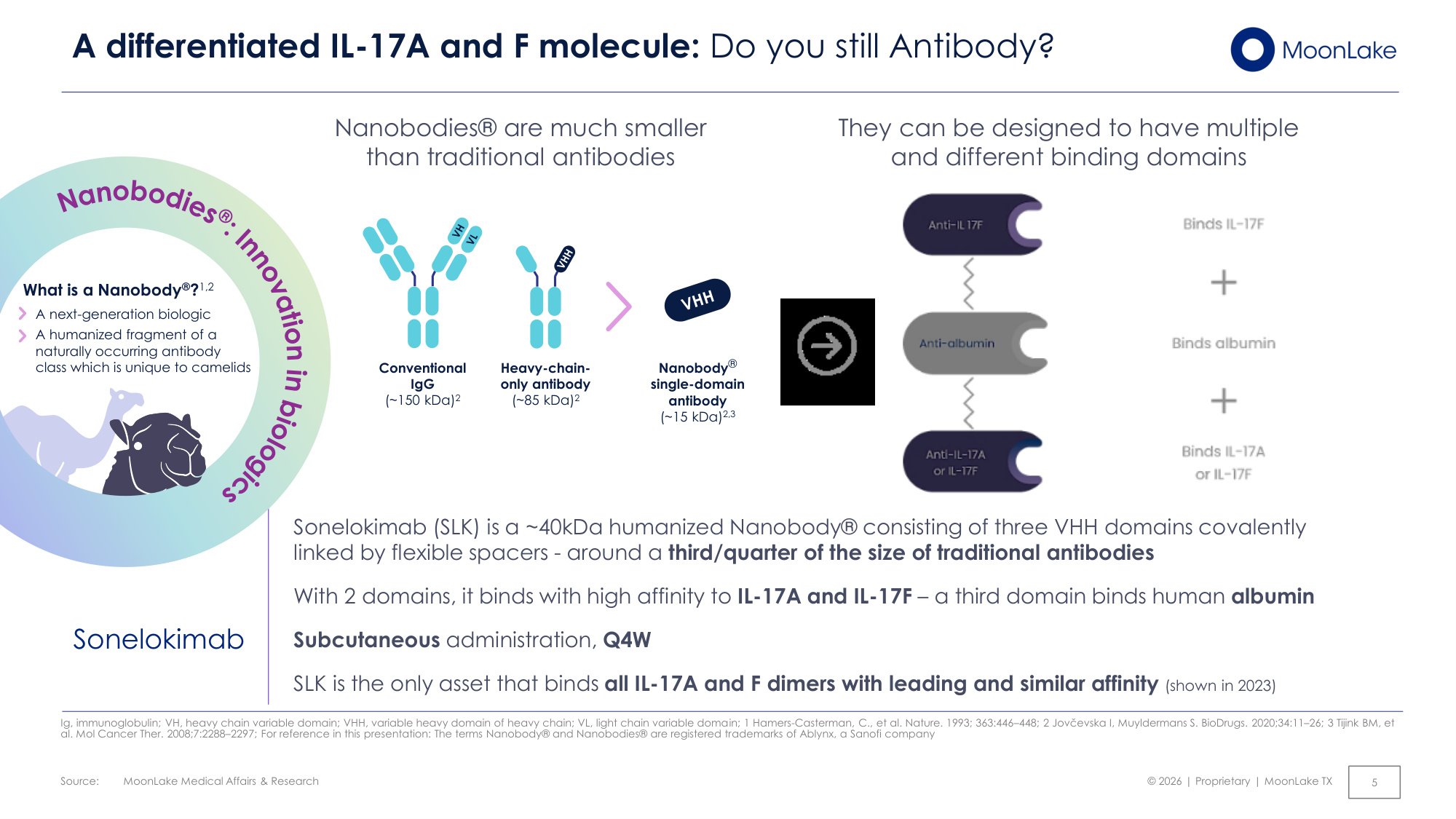
Source: © 2026 | Proprietary | MoonLake TX 5 A differentiated IL-17A and F molecule: Do you still Antibody? Ig, immunoglobulin; VH, heavy chain variable domain; VHH, variable heavy domain of heavy chain; VL, light chain variable domain; 1 Hamers-Casterman, C., et al. Nature. 1993; 363:446–448; 2 Jovčevska I, Muyldermans S. BioDrugs. 2020;34:11–26; 3 Tijink BM, et al. Mol Cancer Ther. 2008;7:2288–2297; For reference in this presentation: The terms Nanobody® and Nanobodies® are registered trademarks of Ablynx, a Sanofi company Nanobodies® are much smaller than traditional antibodies They can be designed to have multiple and different binding domains Sonelokimab (SLK) is a ~40kDa humanized Nanobody® consisting of three VHH domains covalently linked by flexible spacers - around a third/quarter of the size of traditional antibodies With 2 domains, it binds with high affinity to IL-17A and IL-17F – a third domain binds human albumin Subcutaneous administration, Q4W SLK is the only asset that binds all IL-17A and F dimers with leading and similar affinity (shown in 2023) Sonelokimab What is a Nanobody®?1,2 A next-generation biologic A humanized fragment of a naturally occurring antibody class which is unique to camelids Conventional IgG (~150 kDa)2 Heavy-chain- only antibody (~85 kDa)2 Nanobody® single-domain antibody (~15 kDa)2,3 MoonLake Medical Affairs & Research
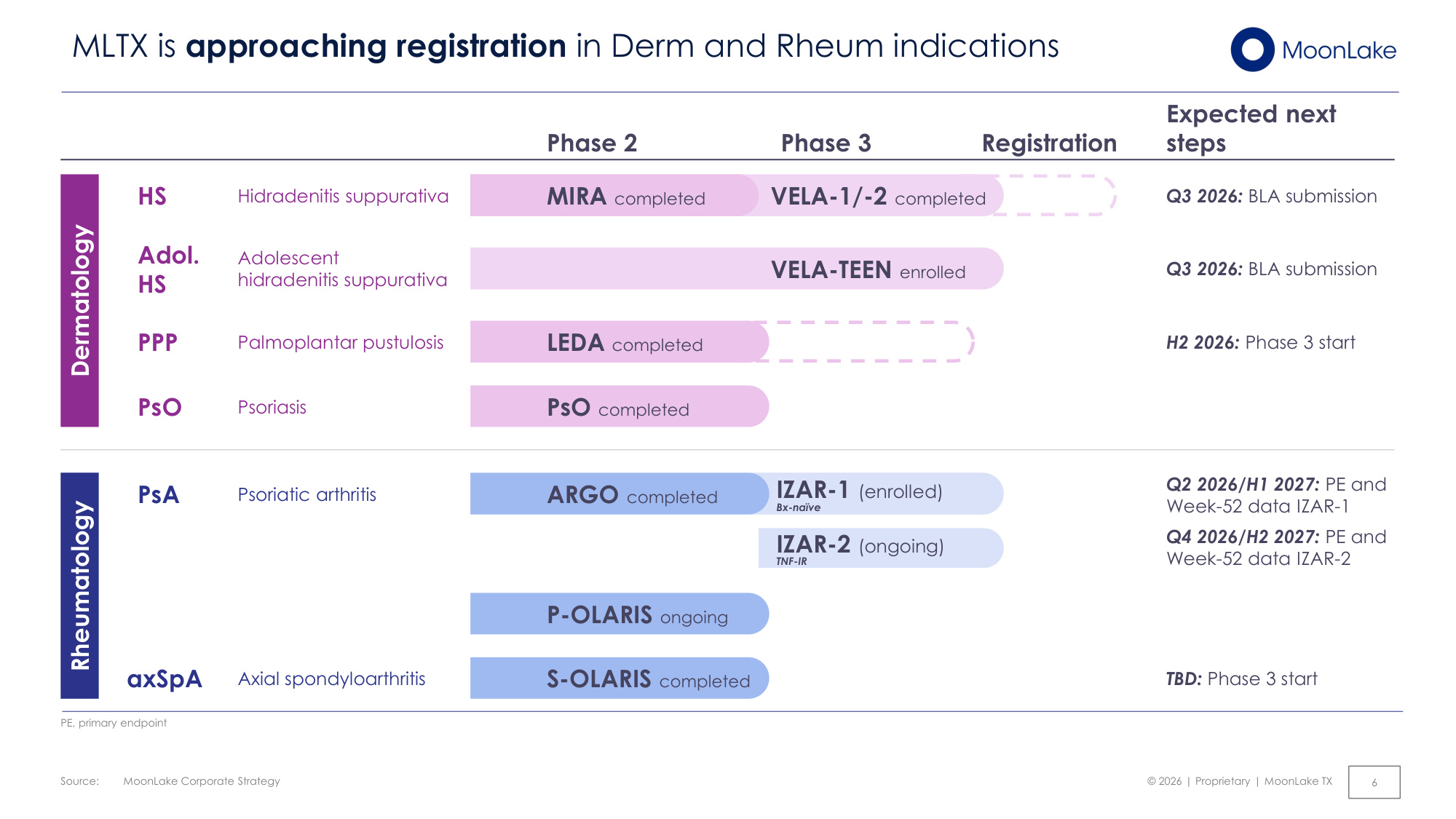
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 6 MLTX is approaching registration in Derm and Rheum indications Dermatology Rheumatology Phase 2 P-OLARIS ongoing Phase 3 Registration Psoriasis PsO completed PsO Expected next steps Hidradenitis suppurativa MIRA completed VELA-1/-2 completed HS Q3 2026: BLA submission Palmoplantar pustulosis LEDA completed PPP H2 2026: Phase 3 start Adolescent hidradenitis suppurativa VELA-TEEN enrolled Adol. HS Q3 2026: BLA submission Axial spondyloarthritis S-OLARIS completed axSpA TBD: Phase 3 start PE, primary endpoint ARGO completed Psoriatic arthritis PsA Q2 2026/H1 2027: PE and Week-52 data IZAR-1 Q4 2026/H2 2027: PE and Week-52 data IZAR-2 IZAR-1 (enrolled) Bx-naïve IZAR-2 (ongoing) TNF-IR
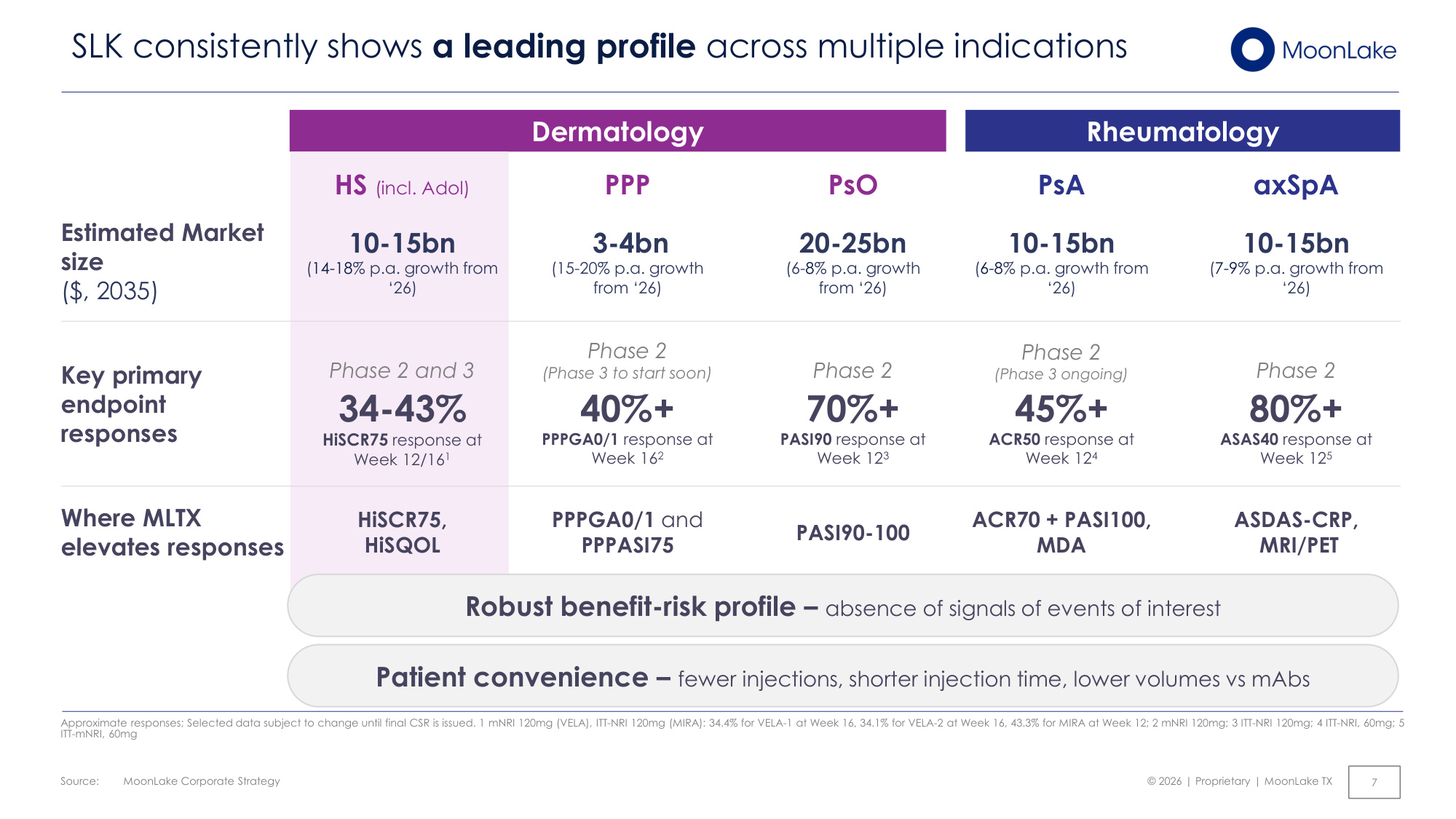
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 7 SLK consistently shows a leading profile across multiple indications Approximate responses; Selected data subject to change until final CSR is issued. 1 mNRI 120mg (VELA), ITT-NRI 120mg (MIRA): 34.4% for VELA-1 at Week 16, 34.1% for VELA-2 at Week 16, 43.3% for MIRA at Week 12; 2 mNRI 120mg; 3 ITT-NRI 120mg; 4 ITT-NRI, 60mg; 5 ITT-mNRI, 60mg Rheumatology Dermatology 10-15bn (6-8% p.a. growth from '26) Phase 2 (Phase 3 ongoing) 45%+ ACR50 response at Week 124 ACR70 + PASI100, MDA 3-4bn (15-20% p.a. growth from '26) 40%+ PPPGA0/1 response at Week 162 Phase 2 (Phase 3 to start soon) PPPGA0/1 and PPPASI75 20-25bn (6-8% p.a. growth from '26) 70%+ PASI90 response at Week 123 Phase 2 PASI90-100 10-15bn (7-9% p.a. growth from '26) 80%+ ASAS40 response at Week 125 Phase 2 ASDAS-CRP, MRI/PET 10-15bn (14-18% p.a. growth from '26) 34-43% HiSCR75 response at Week 12/161 Phase 2 and 3 HiSCR75, HiSQOL Estimated Market size ($, 2035) Key primary endpoint responses Where MLTX elevates responses Robust benefit-risk profile – absence of signals of events of interest Patient convenience – fewer injections, shorter injection time, lower volumes vs mAbs PsA axSpA PPP PsO HS (incl. Adol)
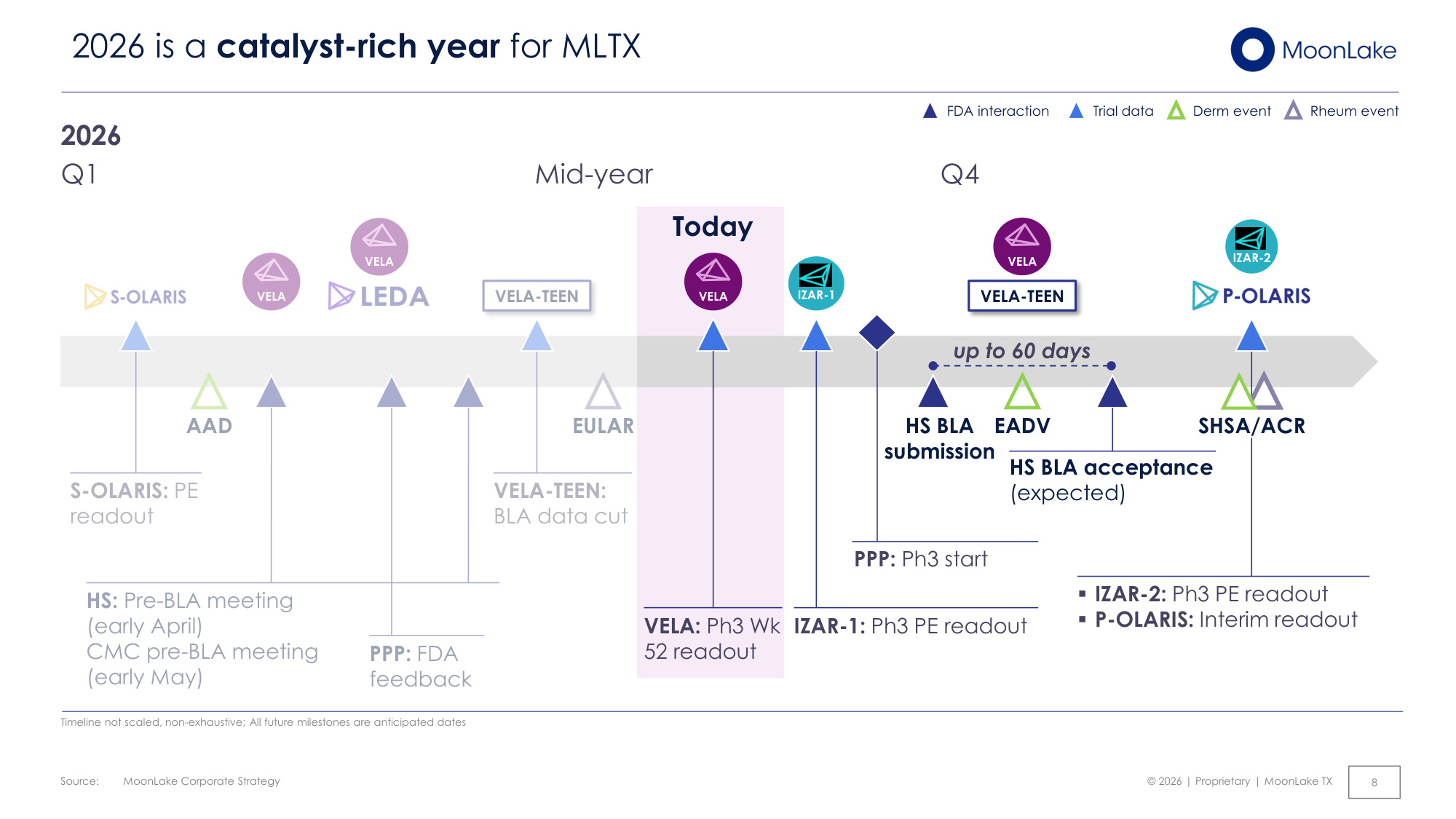
Source: © 2026 | Proprietary | MoonLake TX Today MoonLake Corporate Strategy 8 2026 is a catalyst-rich year for MLTX FDA interaction Trial data Timeline not scaled, non-exhaustive; All future milestones are anticipated dates 2026 up to 60 days ▪IZAR-2: Ph3 PE readout ▪P-OLARIS: Interim readout IZAR-1: Ph3 PE readout Q1 Q4 IZAR-2 Derm event Rheum event AAD VELA HS: Pre-BLA meeting (early April) CMC pre-BLA meeting (early May) PPP: FDA feedback EADV HS BLA submission VELA-TEEN VELA SHSA/ACR VELA-TEEN VELA-TEEN: BLA data cut S-OLARIS: PE readout IZAR-1 EULAR VELA VELA: Ph3 Wk 52 readout VELA Mid-year HS BLA acceptance (expected) PPP: Ph3 start
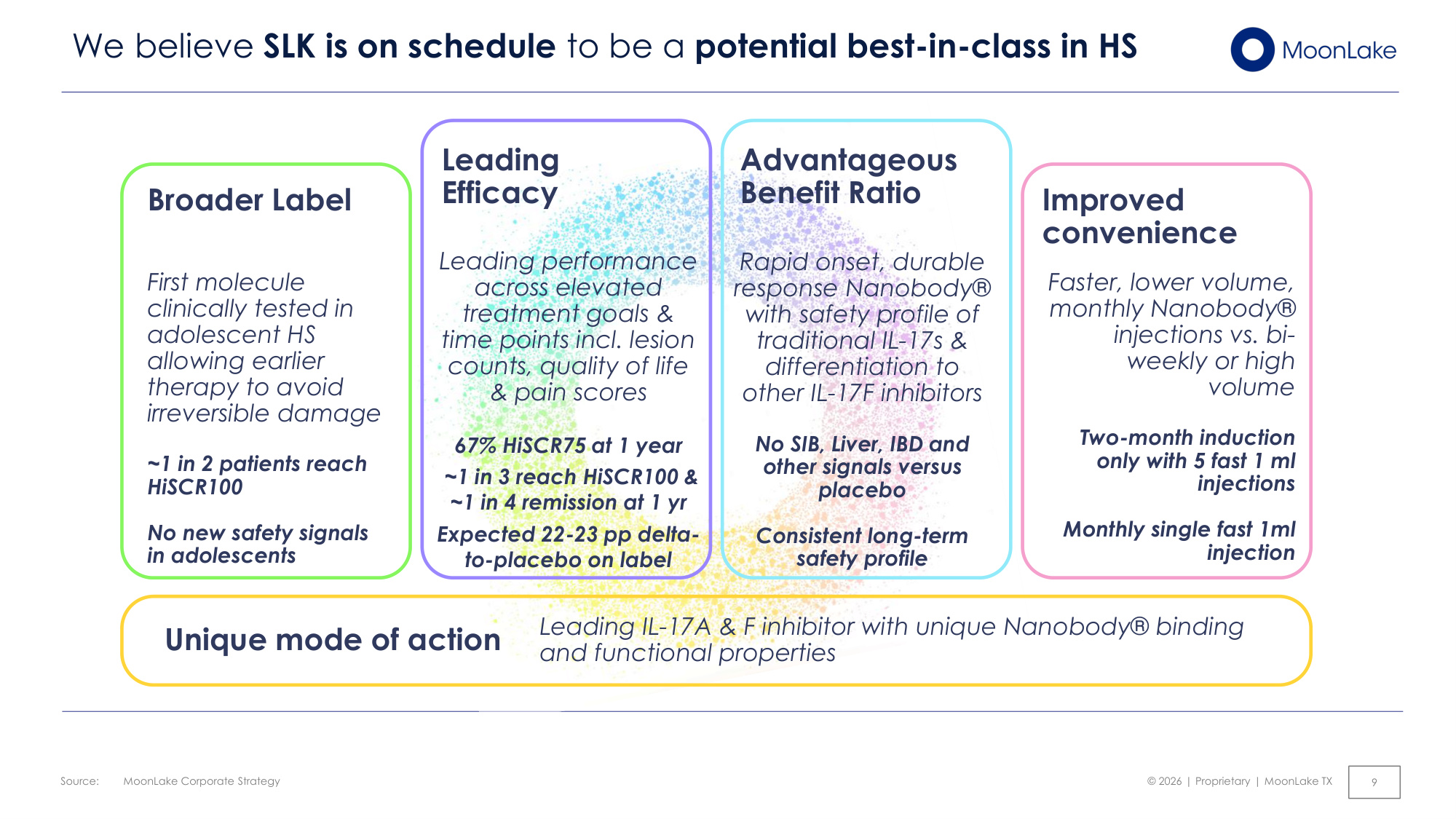
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 9 We believe SLK is on schedule to be a potential best-in-class in HS Leading Efficacy Leading performance across elevated treatment goals & time points incl. lesion counts, quality of life & pain scores 67% HiSCR75 at 1 year ~1 in 3 reach HiSCR100 & ~1 in 4 remission at 1 yr Expected 22-23 pp delta- to-placebo on label Advantageous Benefit Ratio Rapid onset, durable response Nanobody® with safety profile of traditional IL-17s & differentiation to other IL-17F inhibitors No SIB, Liver, IBD and other signals versus placebo Consistent long-term safety profile Broader Label First molecule clinically tested in adolescent HS allowing earlier therapy to avoid irreversible damage ~1 in 2 patients reach HiSCR100 No new safety signals in adolescents Faster, lower volume, monthly Nanobody® injections vs. bi- weekly or high volume Two-month induction only with 5 fast 1 ml injections Monthly single fast 1ml injection Improved convenience Unique mode of action Leading IL-17A & F inhibitor with unique Nanobody® binding and functional properties
© 2026 | Proprietary | MoonLake TX Final data from the VELA program in HS 10
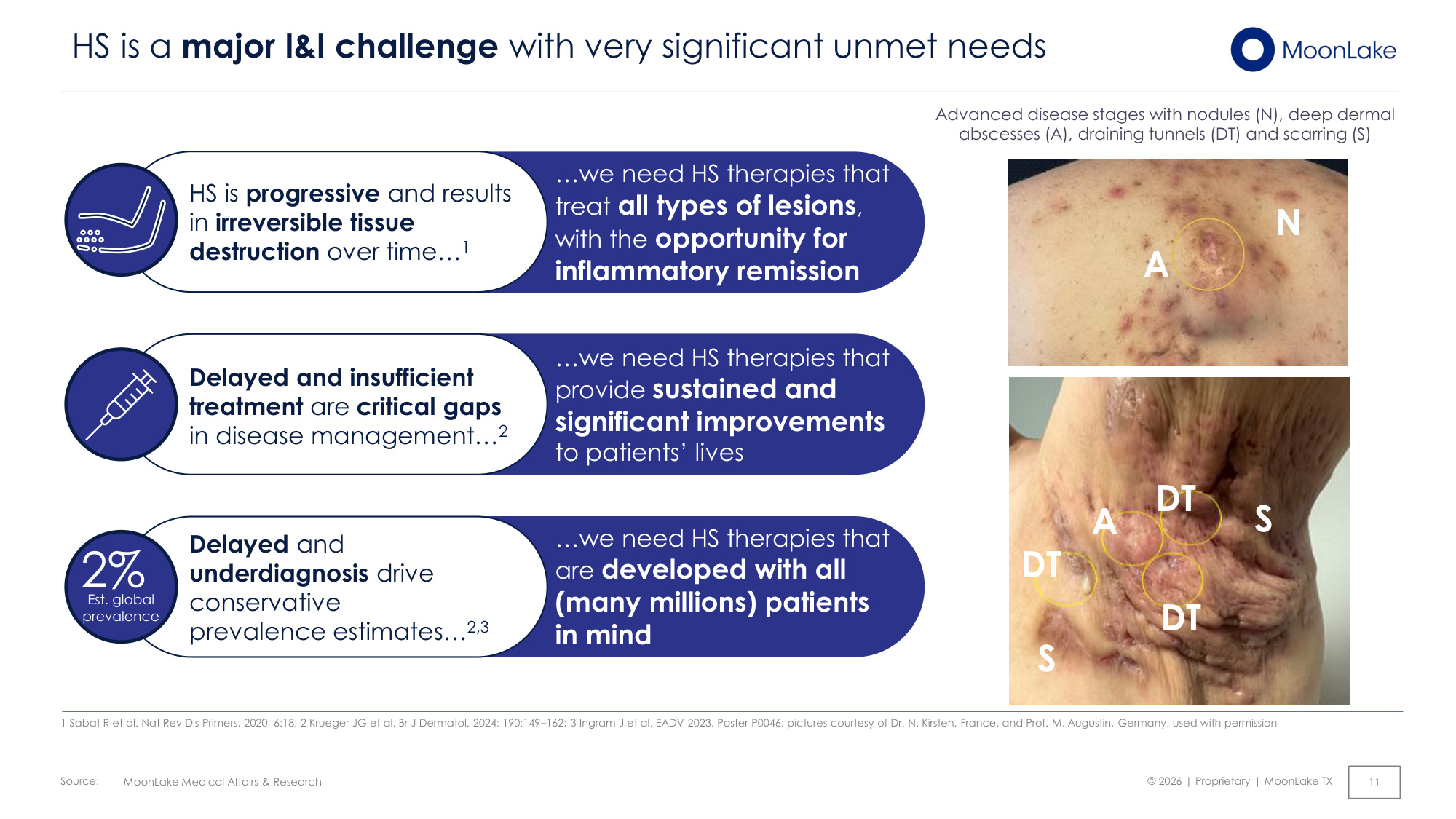
Source: © 2026 | Proprietary | MoonLake TX MoonLake Medical Affairs & Research 11 HS is a major I&I challenge with very significant unmet needs ...we need HS therapies that treat all types of lesions, with the opportunity for inflammatory remission HS is progressive and results in irreversible tissue destruction over time...1 ...we need HS therapies that provide sustained and significant improvements to patients' lives Delayed and insufficient treatment are critical gaps in disease management...2 ...we need HS therapies that are developed with all (many millions) patients in mind Delayed and underdiagnosis drive conservative prevalence estimates...2,3 2% Est. global prevalence 1 Sabat R et al. Nat Rev Dis Primers. 2020; 6:18; 2 Krueger JG et al. Br J Dermatol. 2024; 190:149–162; 3 Ingram J et al. EADV 2023, Poster P0046; pictures courtesy of Dr. N. Kirsten, France, and Prof. M. Augustin, Germany, used with permission Advanced disease stages with nodules (N), deep dermal abscesses (A), draining tunnels (DT) and scarring (S) A T T T DT DT A DT S S N
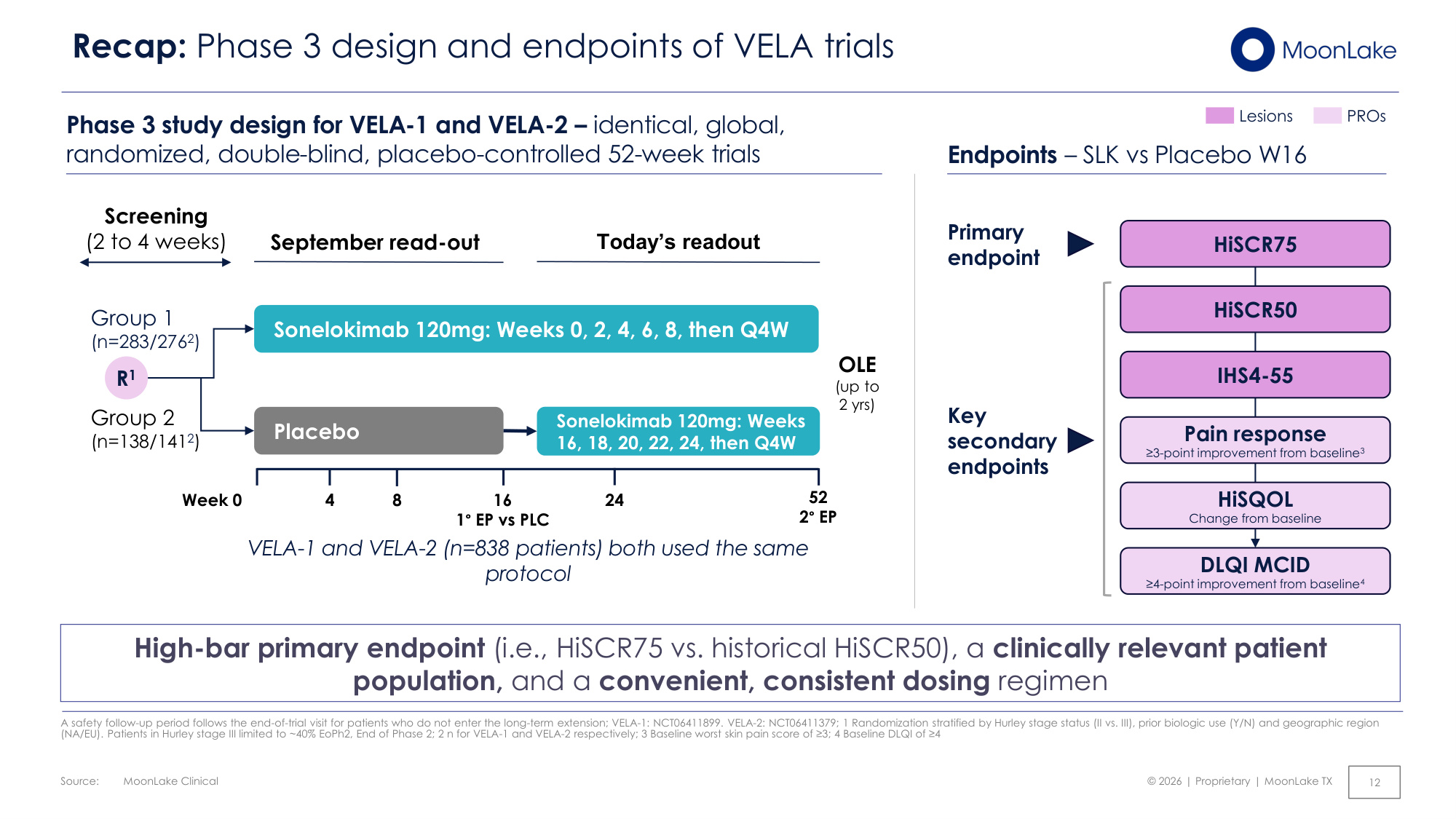
Source: © 2026 | Proprietary | MoonLake TX MoonLake Clinical 12 Recap: Phase 3 design and endpoints of VELA trials Lesions PROs Phase 3 study design for VELA-1 and VELA-2 – identical, global, randomized, double-blind, placebo-controlled 52-week trials Placebo Group 1 (n=283/2762) Group 2 (n=138/1412) Screening (2 to 4 weeks) September read-out Today's readout Sonelokimab 120mg: Weeks 0, 2, 4, 6, 8, then Q4W Sonelokimab 120mg: Weeks 16, 18, 20, 22, 24, then Q4W OLE (up to 2 yrs) R1 Week 0 4 16 1° EP vs PLC 52 2° EP 8 24 VELA-1 and VELA-2 (n=838 patients) both used the same protocol HiSCR75 HiSCR50 IHS4-55 Pain response ≥3-point improvement from baseline3 HiSQOL Change from baseline DLQI MCID ≥4-point improvement from baseline4 Primary endpoint Key secondary endpoints Endpoints – SLK vs Placebo W16 High-bar primary endpoint (i.e., HiSCR75 vs. historical HiSCR50), a clinically relevant patient population, and a convenient, consistent dosing regimen A safety follow-up period follows the end-of-trial visit for patients who do not enter the long-term extension; VELA-1: NCT06411899. VELA-2: NCT06411379; 1 Randomization stratified by Hurley stage status (II vs. III), prior biologic use (Y/N) and geographic region (NA/EU). Patients in Hurley stage III limited to ~40% EoPh2, End of Phase 2; 2 n for VELA-1 and VELA-2 respectively; 3 Baseline worst skin pain score of ≥3; 4 Baseline DLQI of ≥4
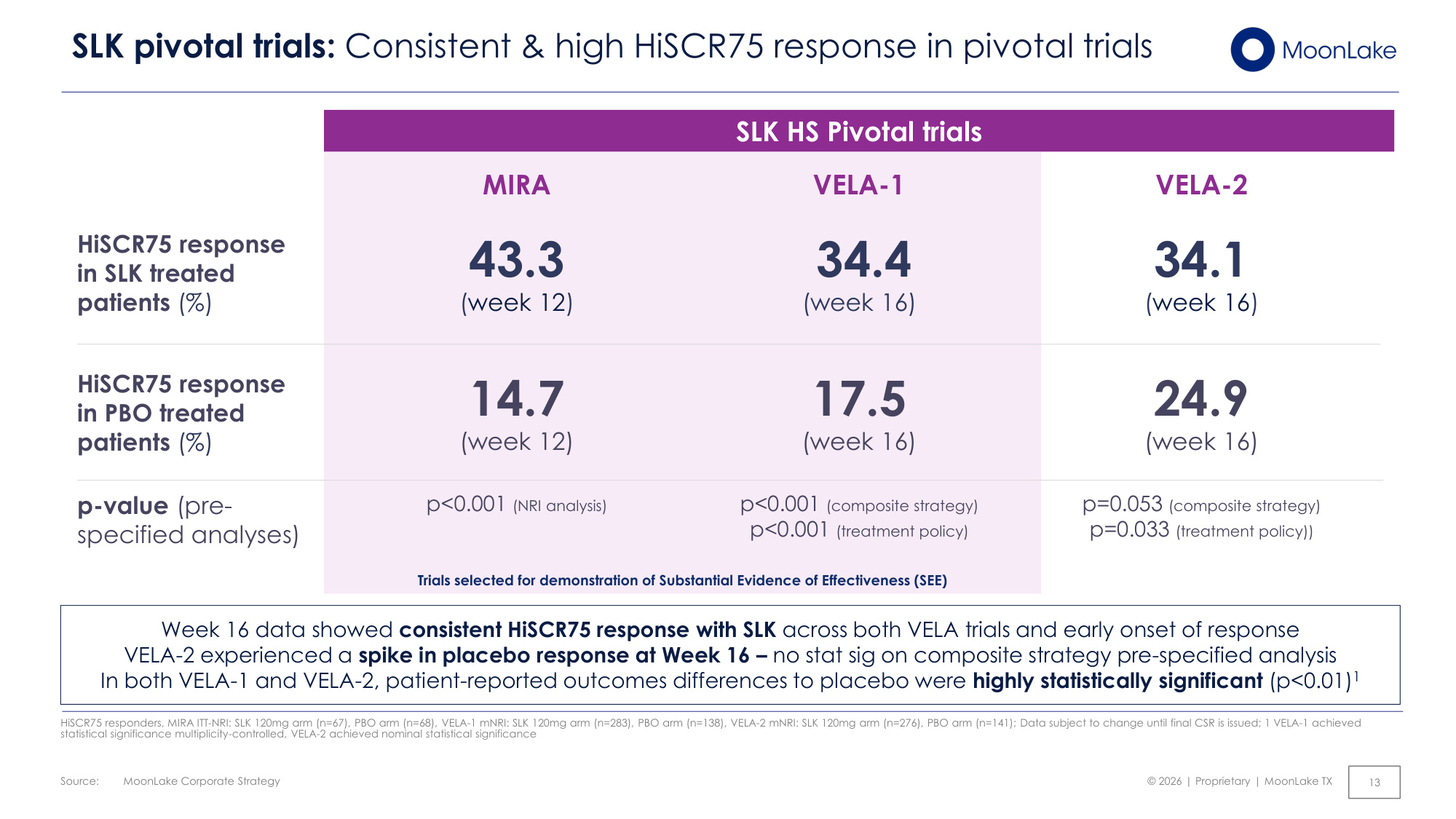
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 13 SLK pivotal trials: Consistent & high HiSCR75 response in pivotal trials SLK HS Pivotal trials HiSCR75 response in SLK treated patients (%) HiSCR75 response in PBO treated patients (%) VELA-1 34.4 (week 16) 17.5 (week 16) p<0.001 (composite strategy) p<0.001 (treatment policy) VELA-2 34.1 (week 16) 24.9 (week 16) p=0.053 (composite strategy) p=0.033 (treatment policy)) MIRA 43.3 (week 12) 14.7 (week 12) p<0.001 (NRI analysis) p-value (pre- specified analyses) HiSCR75 responders, MIRA ITT-NRI: SLK 120mg arm (n=67), PBO arm (n=68), VELA-1 mNRI: SLK 120mg arm (n=283), PBO arm (n=138), VELA-2 mNRI: SLK 120mg arm (n=276), PBO arm (n=141); Data subject to change until final CSR is issued; 1 VELA-1 achieved statistical significance multiplicity-controlled, VELA-2 achieved nominal statistical significance Week 16 data showed consistent HiSCR75 response with SLK across both VELA trials and early onset of response VELA-2 experienced a spike in placebo response at Week 16 – no stat sig on composite strategy pre-specified analysis In both VELA-1 and VELA-2, patient-reported outcomes differences to placebo were highly statistically significant (p<0.01)1 Trials selected for demonstration of Substantial Evidence of Effectiveness (SEE)
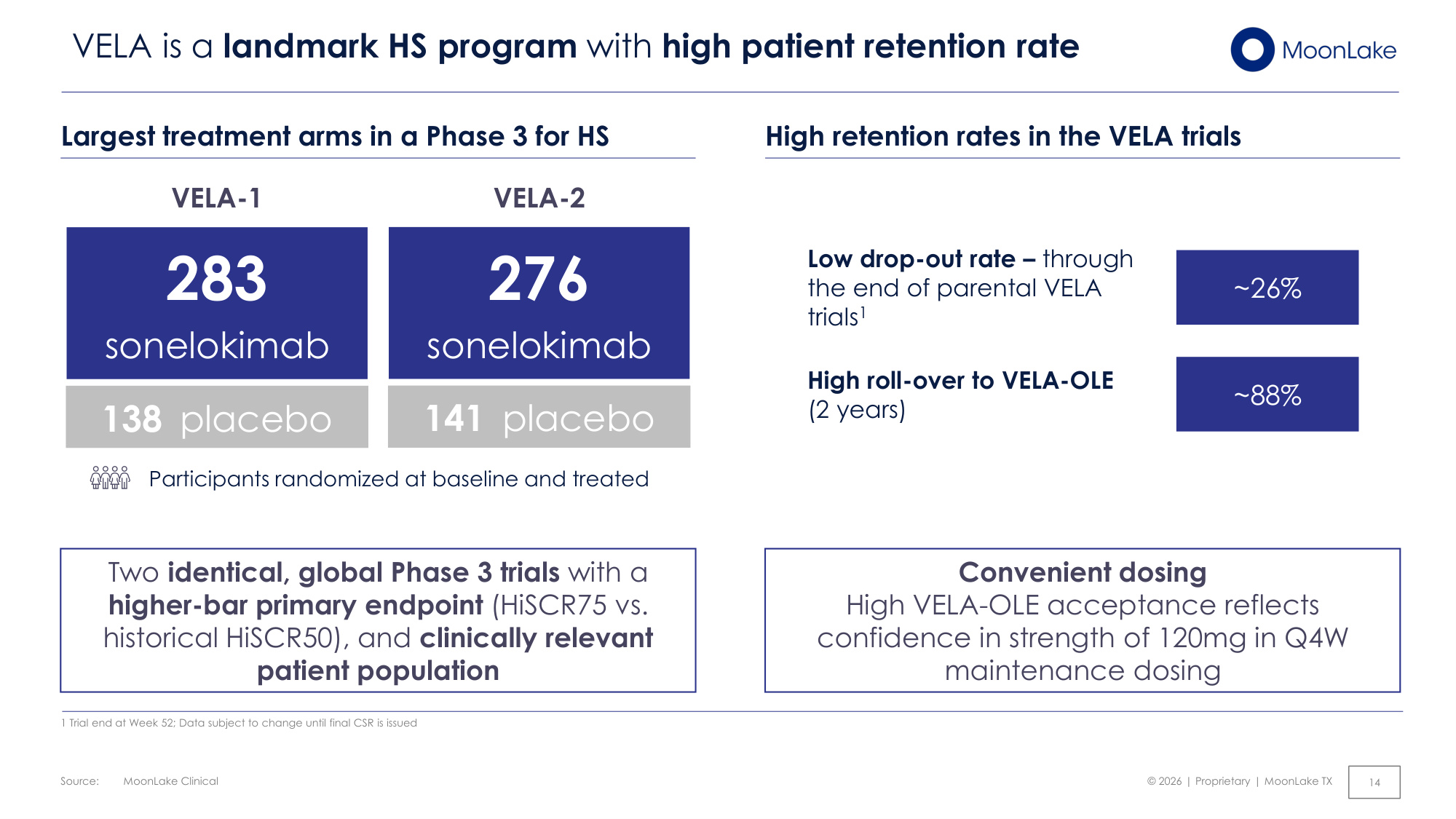
Source: © 2026 | Proprietary | MoonLake TX MoonLake Clinical 14 VELA is a landmark HS program with high patient retention rate Convenient dosing High VELA-OLE acceptance reflects confidence in strength of 120mg in Q4W maintenance dosing High retention rates in the VELA trials ~26% Low drop-out rate – through the end of parental VELA trials1 ~88% High roll-over to VELA-OLE (2 years) VELA-2 VELA-1 Participants randomized at baseline and treated 138 placebo 283 sonelokimab 141 placebo 276 sonelokimab Largest treatment arms in a Phase 3 for HS Two identical, global Phase 3 trials with a higher-bar primary endpoint (HiSCR75 vs. historical HiSCR50), and clinically relevant patient population 1 Trial end at Week 52; Data subject to change until final CSR is issued
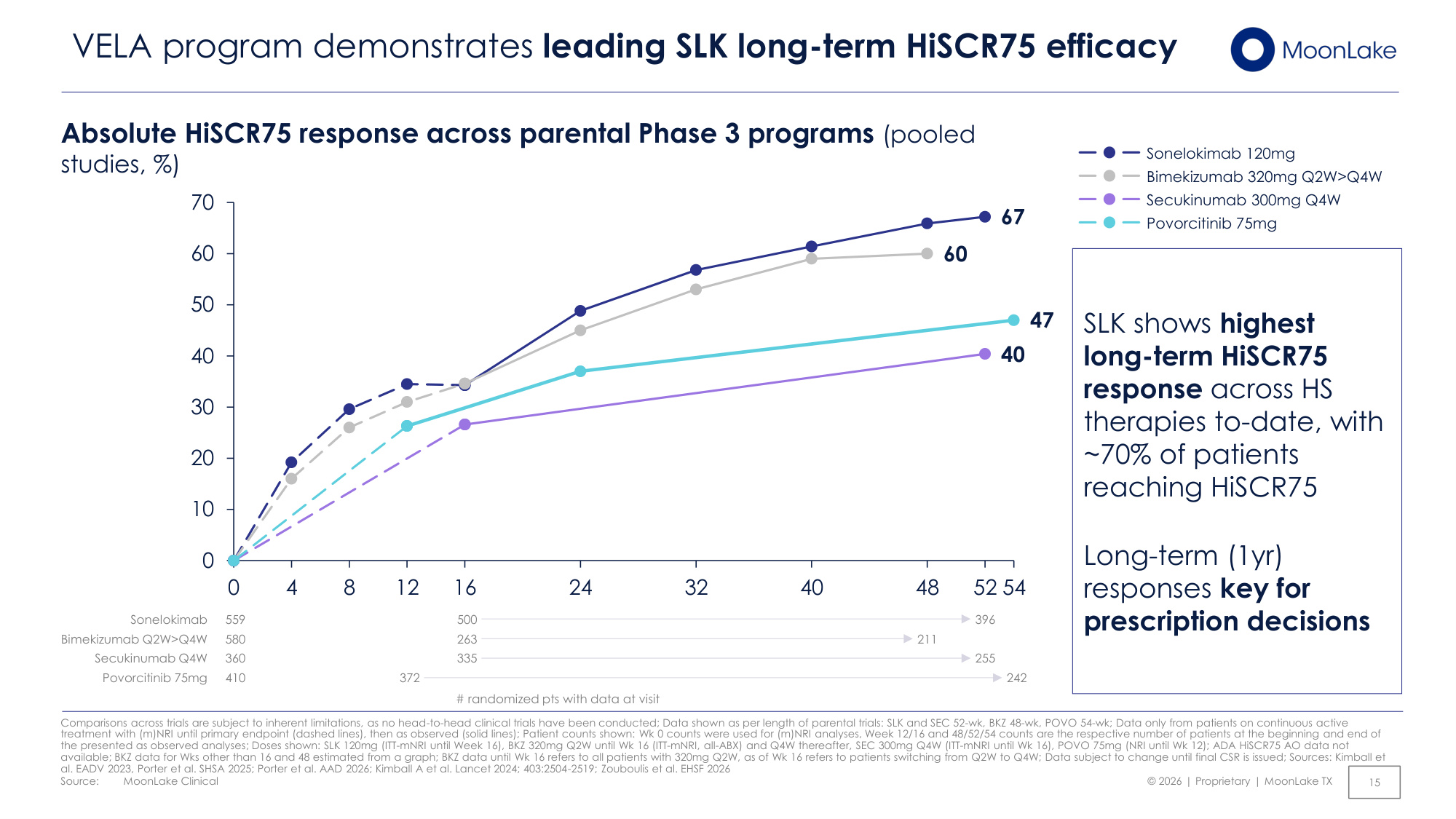
Source: © 2026 | Proprietary | MoonLake TX 67 60 40 47 0 10 20 30 40 50 60 70 0 4 8 12 16 24 32 40 48 52 54 MoonLake Clinical 15 VELA program demonstrates leading SLK long-term HiSCR75 efficacy Absolute HiSCR75 response across parental Phase 3 programs (pooled studies, %) # randomized pts with data at visit Sonelokimab 120mg Bimekizumab 320mg Q2W>Q4W Secukinumab 300mg Q4W Povorcitinib 75mg 211 Bimekizumab Q2W>Q4W 263 580 410 Povorcitinib 75mg 242 Sonelokimab 559 396 500 Secukinumab Q4W 255 360 335 SLK shows highest long-term HiSCR75 response across HS therapies to-date, with ~70% of patients reaching HiSCR75 Long-term (1yr) responses key for prescription decisions Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; Data shown as per length of parental trials: SLK and SEC 52-wk, BKZ 48-wk, POVO 54-wk; Data only from patients on continuous active treatment with (m)NRI until primary endpoint (dashed lines), then as observed (solid lines); Patient counts shown: Wk 0 counts were used for (m)NRI analyses, Week 12/16 and 48/52/54 counts are the respective number of patients at the beginning and end of the presented as observed analyses; Doses shown: SLK 120mg (ITT-mNRI until Week 16), BKZ 320mg Q2W until Wk 16 (ITT-mNRI, all-ABX) and Q4W thereafter, SEC 300mg Q4W (ITT-mNRI until Wk 16), POVO 75mg (NRI until Wk 12); ADA HiSCR75 AO data not available; BKZ data for Wks other than 16 and 48 estimated from a graph; BKZ data until Wk 16 refers to all patients with 320mg Q2W, as of Wk 16 refers to patients switching from Q2W to Q4W; Data subject to change until final CSR is issued; Sources: Kimball et al. EADV 2023, Porter et al. SHSA 2025; Porter et al. AAD 2026; Kimball A et al. Lancet 2024; 403:2504-2519; Zouboulis et al. EHSF 2026 372
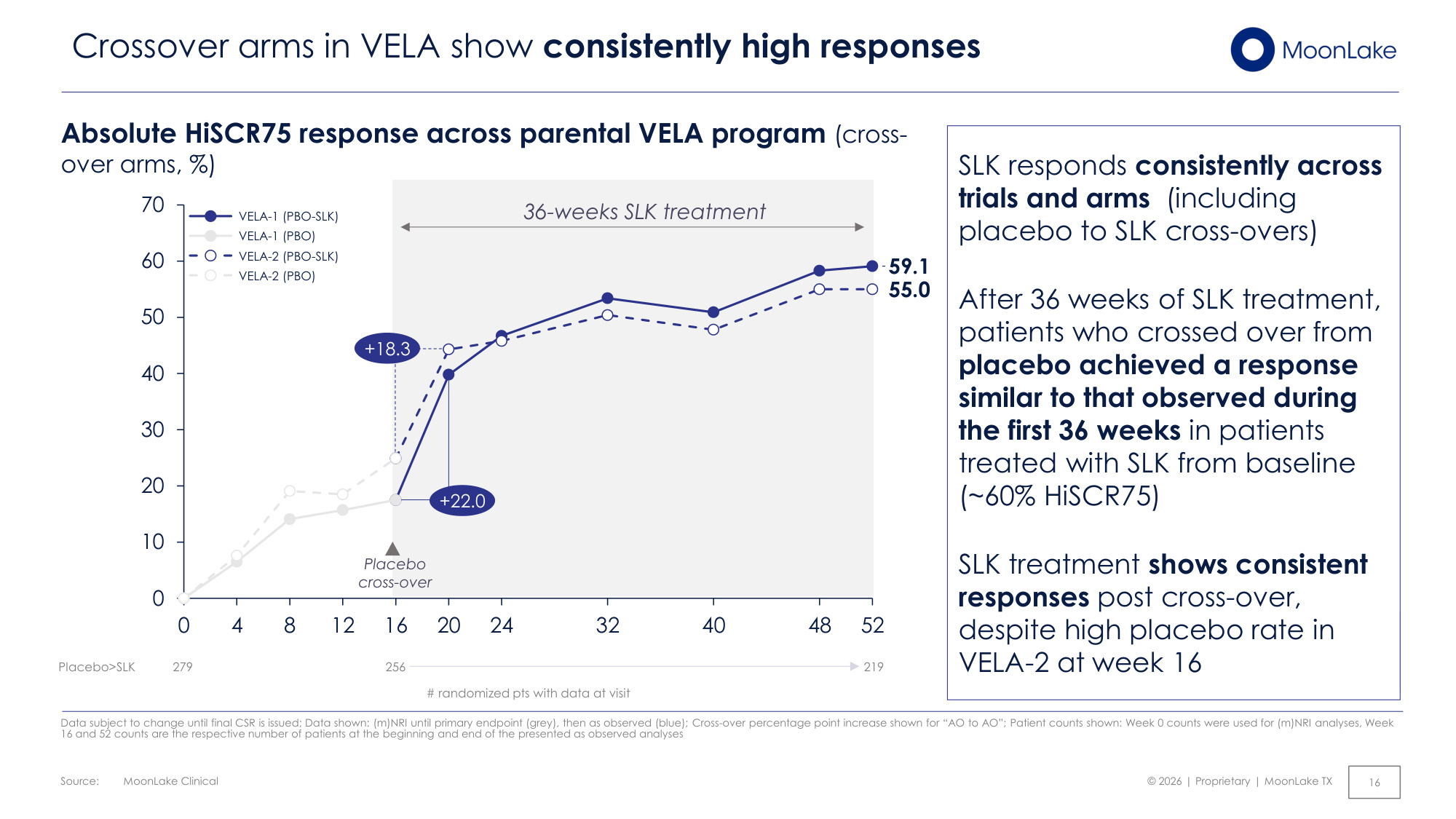
Source: © 2026 | Proprietary | MoonLake TX MoonLake Clinical 16 Crossover arms in VELA show consistently high responses Data subject to change until final CSR is issued; Data shown: (m)NRI until primary endpoint (grey), then as observed (blue); Cross-over percentage point increase shown for "AO to AO"; Patient counts shown: Week 0 counts were used for (m)NRI analyses, Week 16 and 52 counts are the respective number of patients at the beginning and end of the presented as observed analyses 59.1 55.0 0 10 20 30 40 50 60 70 0 4 8 12 16 20 24 32 40 48 52 VELA-1 (PBO-SLK) VELA-1 (PBO) VELA-2 (PBO-SLK) VELA-2 (PBO) Placebo cross-over Placebo>SLK 279 219 256 # randomized pts with data at visit Absolute HiSCR75 response across parental VELA program (cross- over arms, %) SLK responds consistently across trials and arms (including placebo to SLK cross-overs) After 36 weeks of SLK treatment, patients who crossed over from placebo achieved a response similar to that observed during the first 36 weeks in patients treated with SLK from baseline (~60% HiSCR75) SLK treatment shows consistent responses post cross-over, despite high placebo rate in VELA-2 at week 16 36-weeks SLK treatment +22.0 +18.3
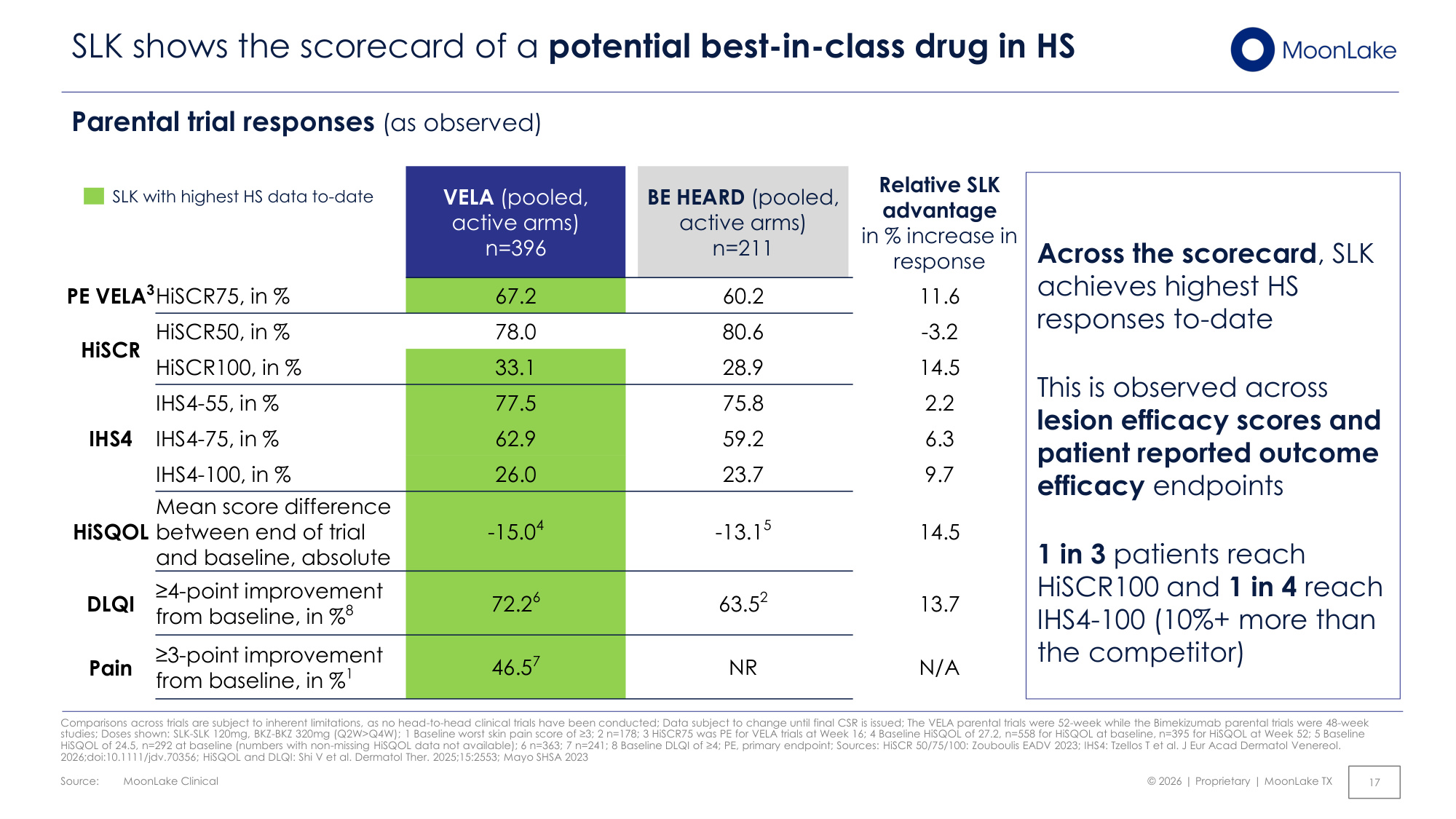
Source: © 2026 | Proprietary | MoonLake TX MoonLake Clinical 17 SLK shows the scorecard of a potential best-in-class drug in HS Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; Data subject to change until final CSR is issued; The VELA parental trials were 52-week while the Bimekizumab parental trials were 48-week studies; Doses shown: SLK-SLK 120mg, BKZ-BKZ 320mg (Q2W>Q4W); 1 Baseline worst skin pain score of ≥3; 2 n=178; 3 HiSCR75 was PE for VELA trials at Week 16; 4 Baseline HiSQOL of 27.2, n=558 for HiSQOL at baseline, n=395 for HiSQOL at Week 52; 5 Baseline HiSQOL of 24.5, n=292 at baseline (numbers with non-missing HiSQOL data not available); 6 n=363; 7 n=241; 8 Baseline DLQI of ≥4; PE, primary endpoint; Sources: HiSCR 50/75/100: Zouboulis EADV 2023; IHS4: Tzellos T et al. J Eur Acad Dermatol Venereol. 2026;doi:10.1111/jdv.70356; HiSQOL and DLQI: Shi V et al. Dermatol Ther. 2025;15:2553; Mayo SHSA 2023 VELA (pooled, active arms) n=396 BE HEARD (pooled, active arms) n=211 Relative SLK advantage in % increase in response PE VELA3HiSCR75, in % 67.2 60.2 11.6 HiSCR HiSCR50, in % 78.0 80.6 -3.2 HiSCR100, in % 33.1 28.9 14.5 IHS4 IHS4-55, in % 77.5 75.8 2.2 IHS4-75, in % 62.9 59.2 6.3 IHS4-100, in % 26.0 23.7 9.7 HiSQOL Mean score difference between end of trial and baseline, absolute -15.04 -13.15 14.5 DLQI ≥4-point improvement from baseline, in %8 72.26 63.52 13.7 Pain ≥3-point improvement from baseline, in %1 46.57 NR N/A Across the scorecard, SLK achieves highest HS responses to-date This is observed across lesion efficacy scores and patient reported outcome efficacy endpoints 1 in 3 patients reach HiSCR100 and 1 in 4 reach IHS4-100 (10%+ more than the competitor) SLK with highest HS data to-date Parental trial responses (as observed)
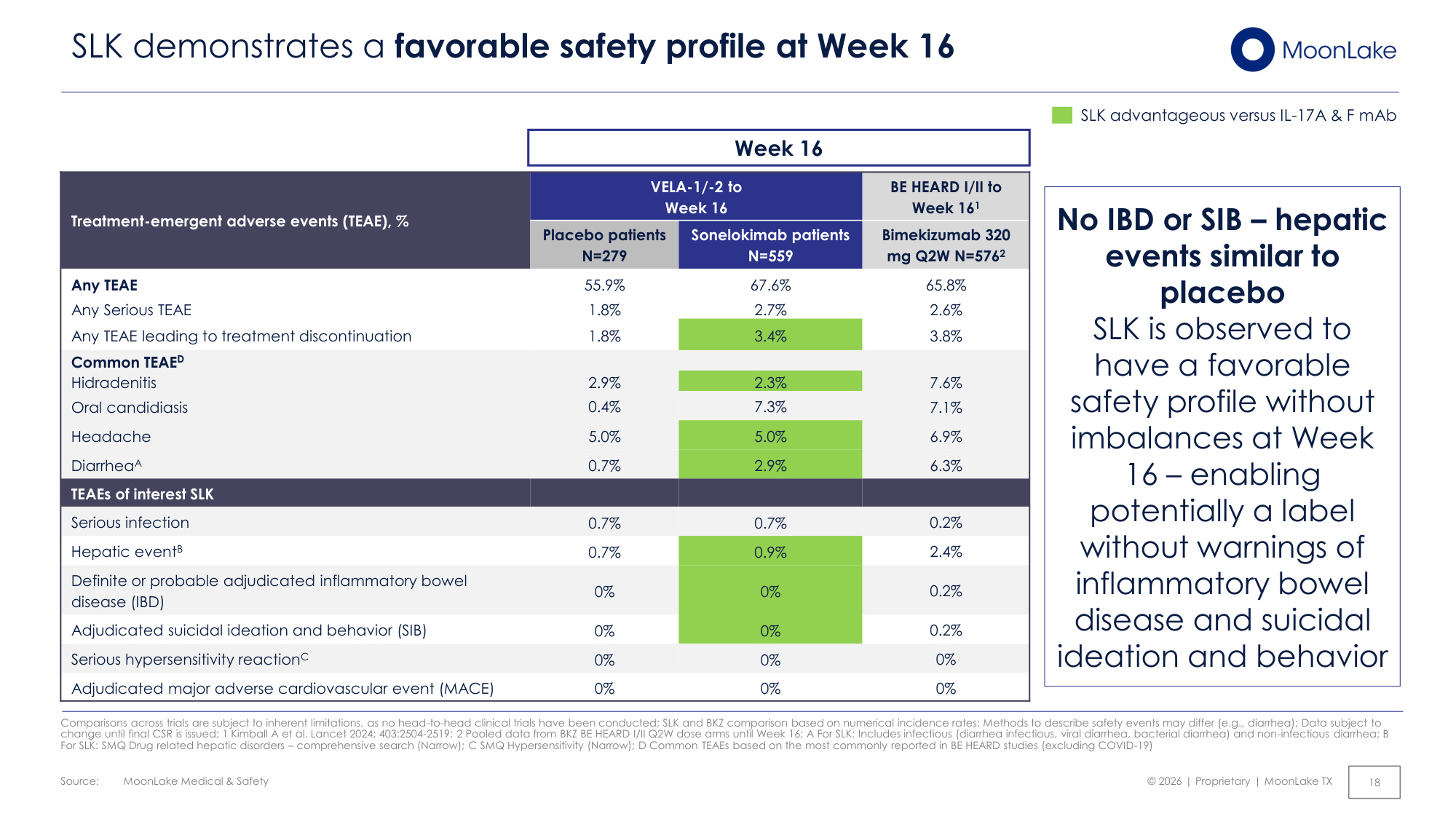
Source: © 2026 | Proprietary | MoonLake TX MoonLake Medical & Safety SLK demonstrates a favorable safety profile at Week 16 Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; SLK and BKZ comparison based on numerical incidence rates; Methods to describe safety events may differ (e.g., diarrhea); Data subject to change until final CSR is issued; 1 Kimball A et al. Lancet 2024; 403:2504-2519; 2 Pooled data from BKZ BE HEARD I/II Q2W dose arms until Week 16; A For SLK: Includes infectious (diarrhea infectious, viral diarrhea, bacterial diarrhea) and non-infectious diarrhea; B For SLK: SMQ Drug related hepatic disorders – comprehensive search (Narrow); C SMQ Hypersensitivity (Narrow); D Common TEAEs based on the most commonly reported in BE HEARD studies (excluding COVID-19) Treatment-emergent adverse events (TEAE), % VELA-1/-2 to Week 16 BE HEARD I/II to Week 161 Placebo patients N=279 Sonelokimab patients N=559 Bimekizumab 320 mg Q2W N=5762 Any TEAE 55.9% 67.6% 65.8% Any Serious TEAE 1.8% 2.7% 2.6% Any TEAE leading to treatment discontinuation 1.8% 3.4% 3.8% Common TEAED Hidradenitis 2.9% 2.3% 7.6% Oral candidiasis 0.4% 7.3% 7.1% Headache 5.0% 5.0% 6.9% DiarrheaA 0.7% 2.9% 6.3% TEAEs of interest SLK Serious infection 0.7% 0.7% 0.2% Hepatic eventB 0.7% 0.9% 2.4% Definite or probable adjudicated inflammatory bowel disease (IBD) 0% 0% 0.2% Adjudicated suicidal ideation and behavior (SIB) 0% 0% 0.2% Serious hypersensitivity reactionC 0% 0% 0% Adjudicated major adverse cardiovascular event (MACE) 0% 0% 0% 18 No IBD or SIB – hepatic events similar to placebo SLK is observed to have a favorable safety profile without imbalances at Week 16 – enabling potentially a label without warnings of inflammatory bowel disease and suicidal ideation and behavior Week 16 SLK advantageous versus IL-17A & F mAb
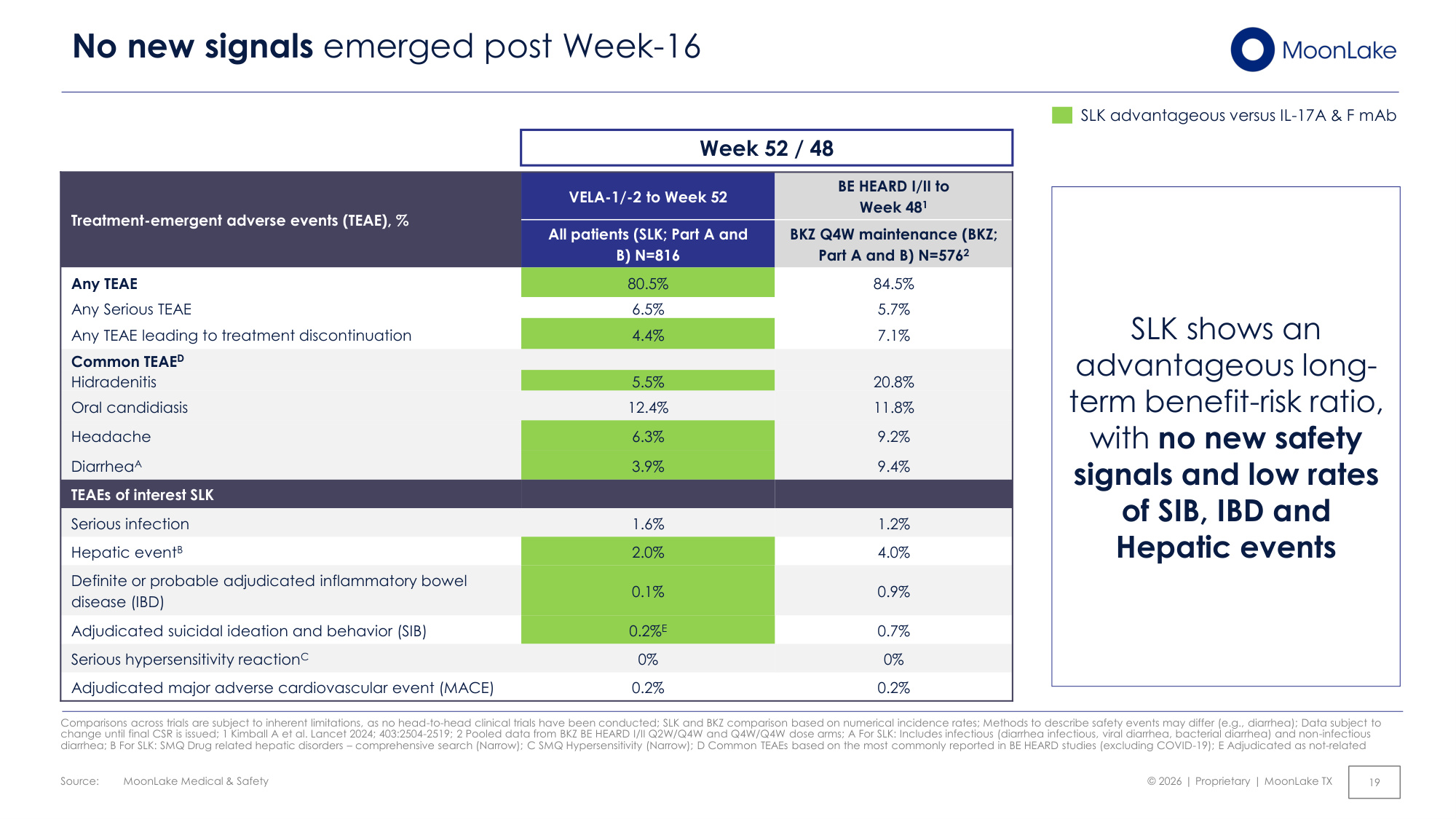
Source: © 2026 | Proprietary | MoonLake TX MoonLake Medical & Safety No new signals emerged post Week-16 Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; SLK and BKZ comparison based on numerical incidence rates; Methods to describe safety events may differ (e.g., diarrhea); Data subject to change until final CSR is issued; 1 Kimball A et al. Lancet 2024; 403:2504-2519; 2 Pooled data from BKZ BE HEARD I/II Q2W/Q4W and Q4W/Q4W dose arms; A For SLK: Includes infectious (diarrhea infectious, viral diarrhea, bacterial diarrhea) and non-infectious diarrhea; B For SLK: SMQ Drug related hepatic disorders – comprehensive search (Narrow); C SMQ Hypersensitivity (Narrow); D Common TEAEs based on the most commonly reported in BE HEARD studies (excluding COVID-19); E Adjudicated as not-related Treatment-emergent adverse events (TEAE), % VELA-1/-2 to Week 52 BE HEARD I/II to Week 481 All patients (SLK; Part A and B) N=816 BKZ Q4W maintenance (BKZ; Part A and B) N=5762 Any TEAE 80.5% 84.5% Any Serious TEAE 6.5% 5.7% Any TEAE leading to treatment discontinuation 4.4% 7.1% Common TEAED Hidradenitis 5.5% 20.8% Oral candidiasis 12.4% 11.8% Headache 6.3% 9.2% DiarrheaA 3.9% 9.4% TEAEs of interest SLK Serious infection 1.6% 1.2% Hepatic eventB 2.0% 4.0% Definite or probable adjudicated inflammatory bowel disease (IBD) 0.1% 0.9% Adjudicated suicidal ideation and behavior (SIB) 0.2%E 0.7% Serious hypersensitivity reactionC 0% 0% Adjudicated major adverse cardiovascular event (MACE) 0.2% 0.2% Week 52 / 48 19 SLK shows an advantageous long- term benefit-risk ratio, with no new safety signals and low rates of SIB, IBD and Hepatic events SLK advantageous versus IL-17A & F mAb
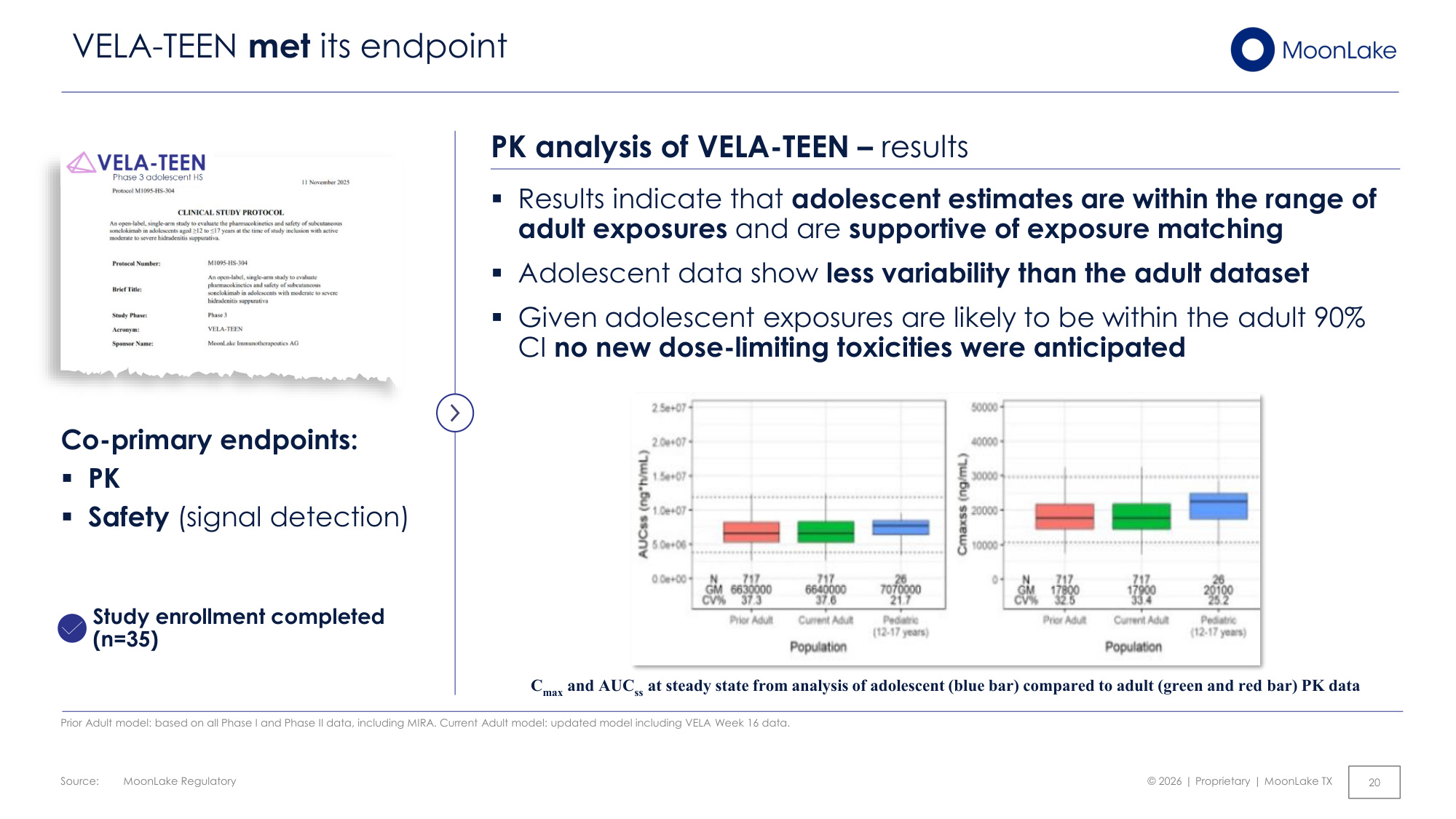
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 20 VELA-TEEN met its endpoint PK analysis of VELA-TEEN – results ▪Results indicate that adolescent estimates are within the range of adult exposures and are supportive of exposure matching ▪Adolescent data show less variability than the adult dataset ▪Given adolescent exposures are likely to be within the adult 90% CI no new dose-limiting toxicities were anticipated Co-primary endpoints: ▪PK ▪Safety (signal detection) Study enrollment completed (n=35) Cmax and AUCss at steady state from analysis of adolescent (blue bar) compared to adult (green and red bar) PK data Prior Adult model: based on all Phase I and Phase II data, including MIRA. Current Adult model: updated model including VELA Week 16 data.
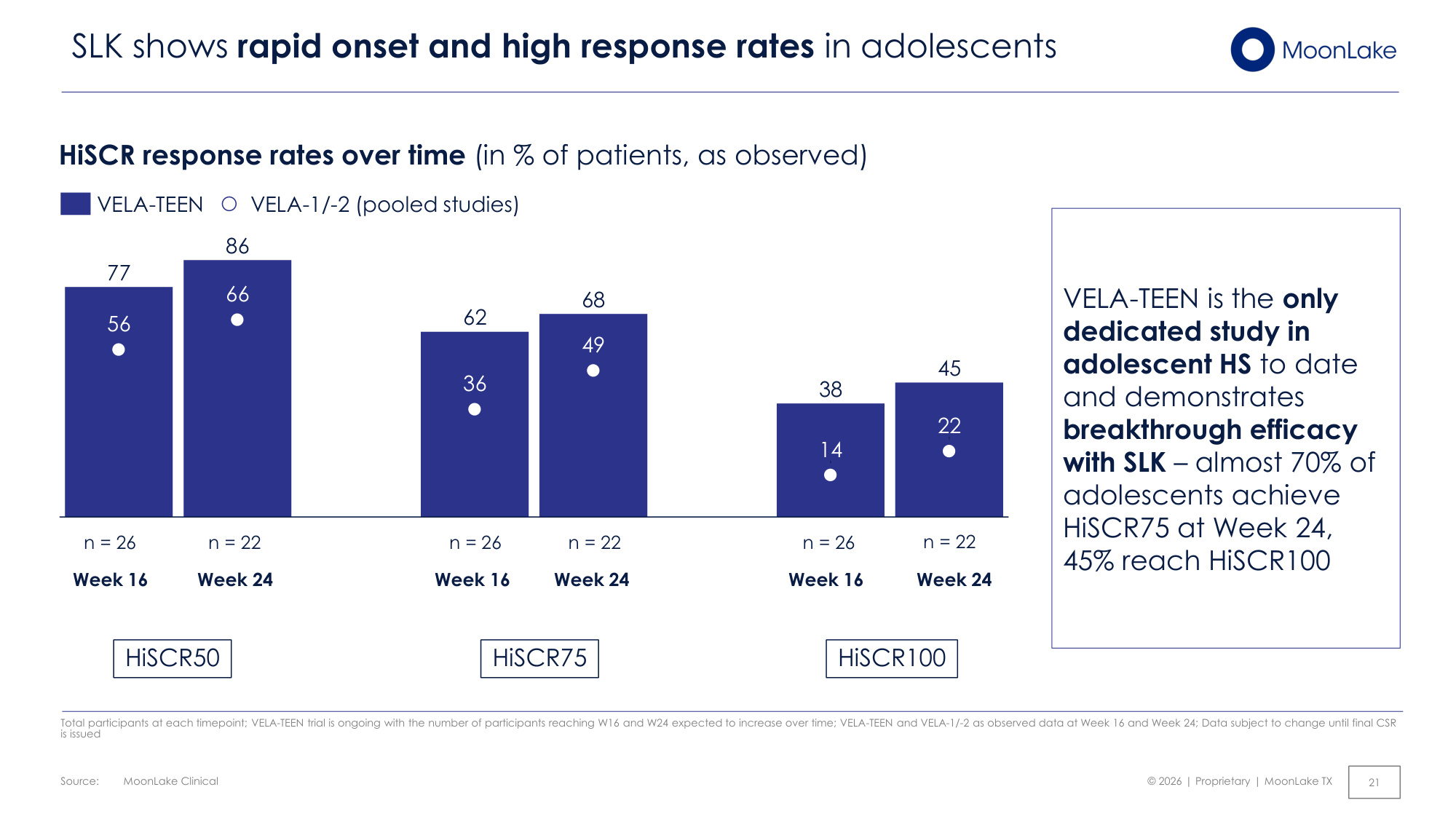
Source: © 2026 | Proprietary | MoonLake TX MoonLake Clinical 21 SLK shows rapid onset and high response rates in adolescents Total participants at each timepoint; VELA-TEEN trial is ongoing with the number of participants reaching W16 and W24 expected to increase over time; VELA-TEEN and VELA-1/-2 as observed data at Week 16 and Week 24; Data subject to change until final CSR is issued HiSCR response rates over time (in % of patients, as observed) HiSCR50 HiSCR75 HiSCR100 VELA-TEEN is the only dedicated study in adolescent HS to date and demonstrates breakthrough efficacy with SLK – almost 70% of adolescents achieve HiSCR75 at Week 24, 45% reach HiSCR100 77 86 62 68 38 45 56 66 36 49 14 22 VELA-TEEN VELA-1/-2 (pooled studies) Week 24 Week 16 Week 24 Week 16 n = 22 n = 26 n = 22 n = 26 Week 24 Week 16 n = 22 n = 26
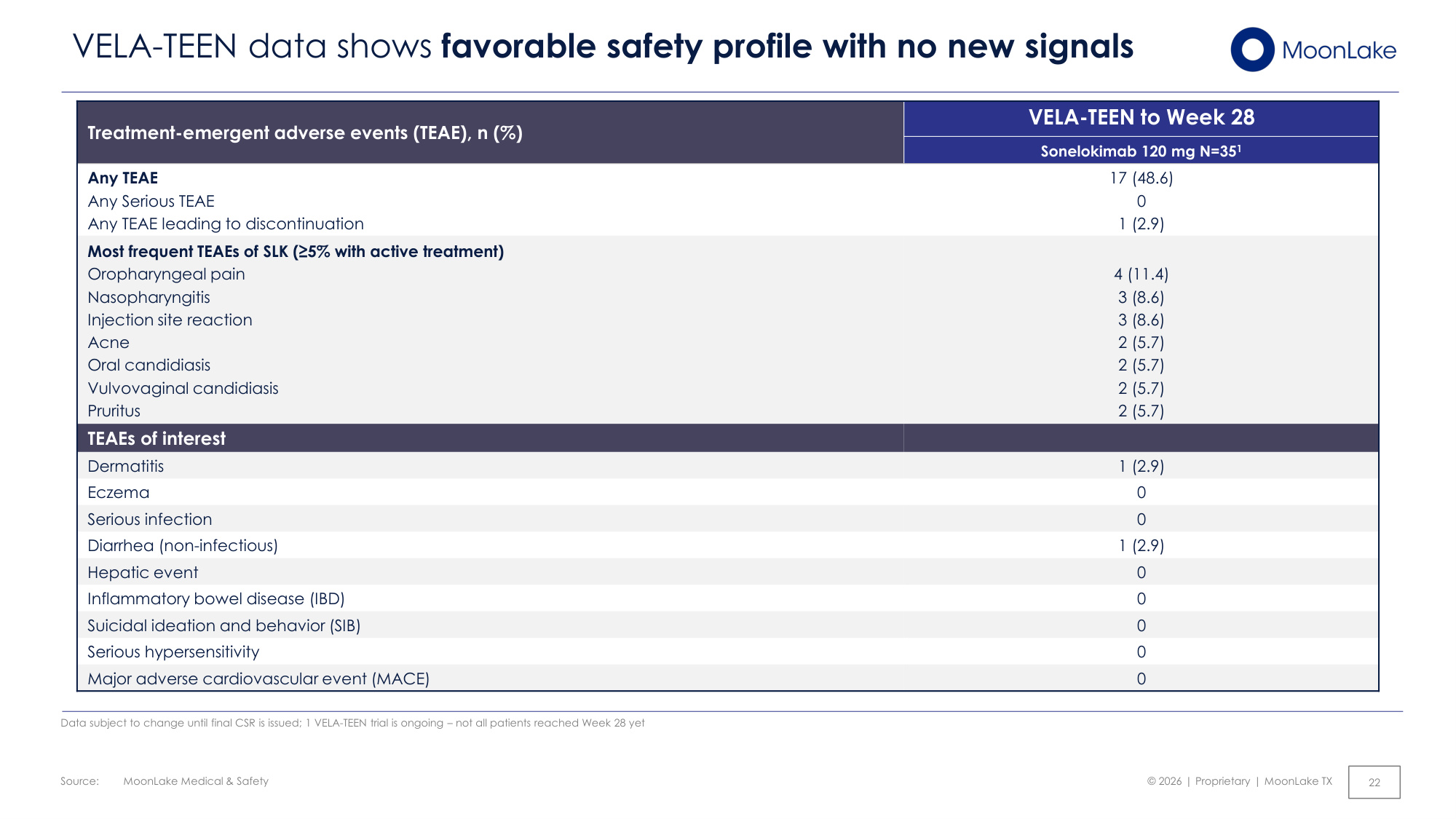
Source: © 2026 | Proprietary | MoonLake TX MoonLake Medical & Safety 22 VELA-TEEN data shows favorable safety profile with no new signals Data subject to change until final CSR is issued; 1 VELA-TEEN trial is ongoing – not all patients reached Week 28 yet Treatment-emergent adverse events (TEAE), n (%) VELA-TEEN to Week 28 Sonelokimab 120 mg N=351 Any TEAE Any Serious TEAE Any TEAE leading to discontinuation 17 (48.6) 0 1 (2.9) Most frequent TEAEs of SLK (≥5% with active treatment) Oropharyngeal pain Nasopharyngitis Injection site reaction Acne Oral candidiasis Vulvovaginal candidiasis Pruritus 4 (11.4) 3 (8.6) 3 (8.6) 2 (5.7) 2 (5.7) 2 (5.7) 2 (5.7) TEAEs of interest Dermatitis 1 (2.9) Eczema 0 Serious infection 0 Diarrhea (non-infectious) 1 (2.9) Hepatic event 0 Inflammatory bowel disease (IBD) 0 Suicidal ideation and behavior (SIB) 0 Serious hypersensitivity 0 Major adverse cardiovascular event (MACE) 0
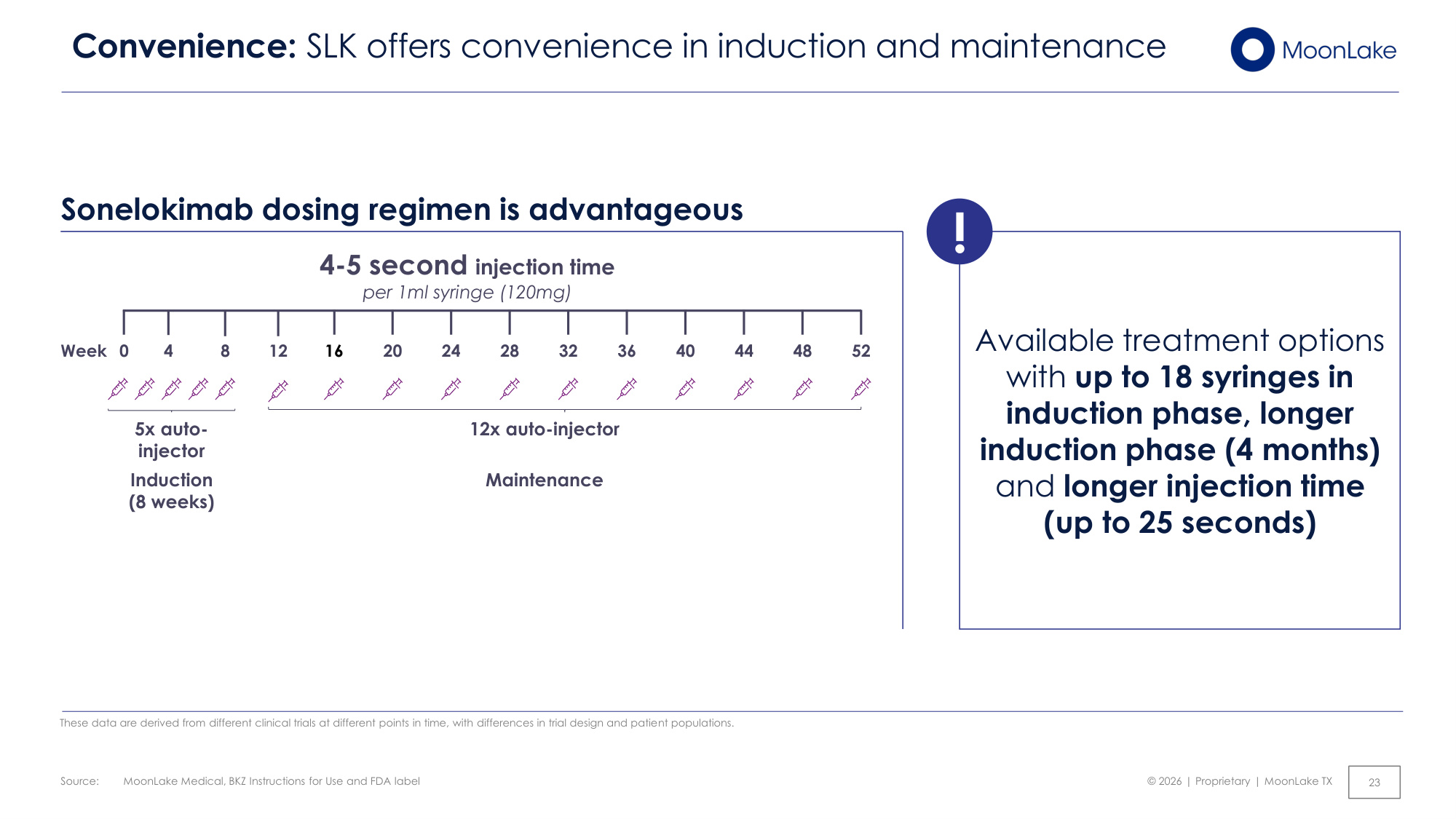
Source: © 2026 | Proprietary | MoonLake TX MoonLake Medical, BKZ Instructions for Use and FDA label 23 Convenience: SLK offers convenience in induction and maintenance These data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. Available treatment options with up to 18 syringes in induction phase, longer induction phase (4 months) and longer injection time (up to 25 seconds) Sonelokimab dosing regimen is advantageous Induction (8 weeks) 4-5 second injection time per 1ml syringe (120mg) Maintenance 4 Week 24 28 32 36 40 44 48 8 12 52 16 20 5x auto- injector 12x auto-injector 0 !

© 2026 | Proprietary | MoonLake TX BLA strategy 24
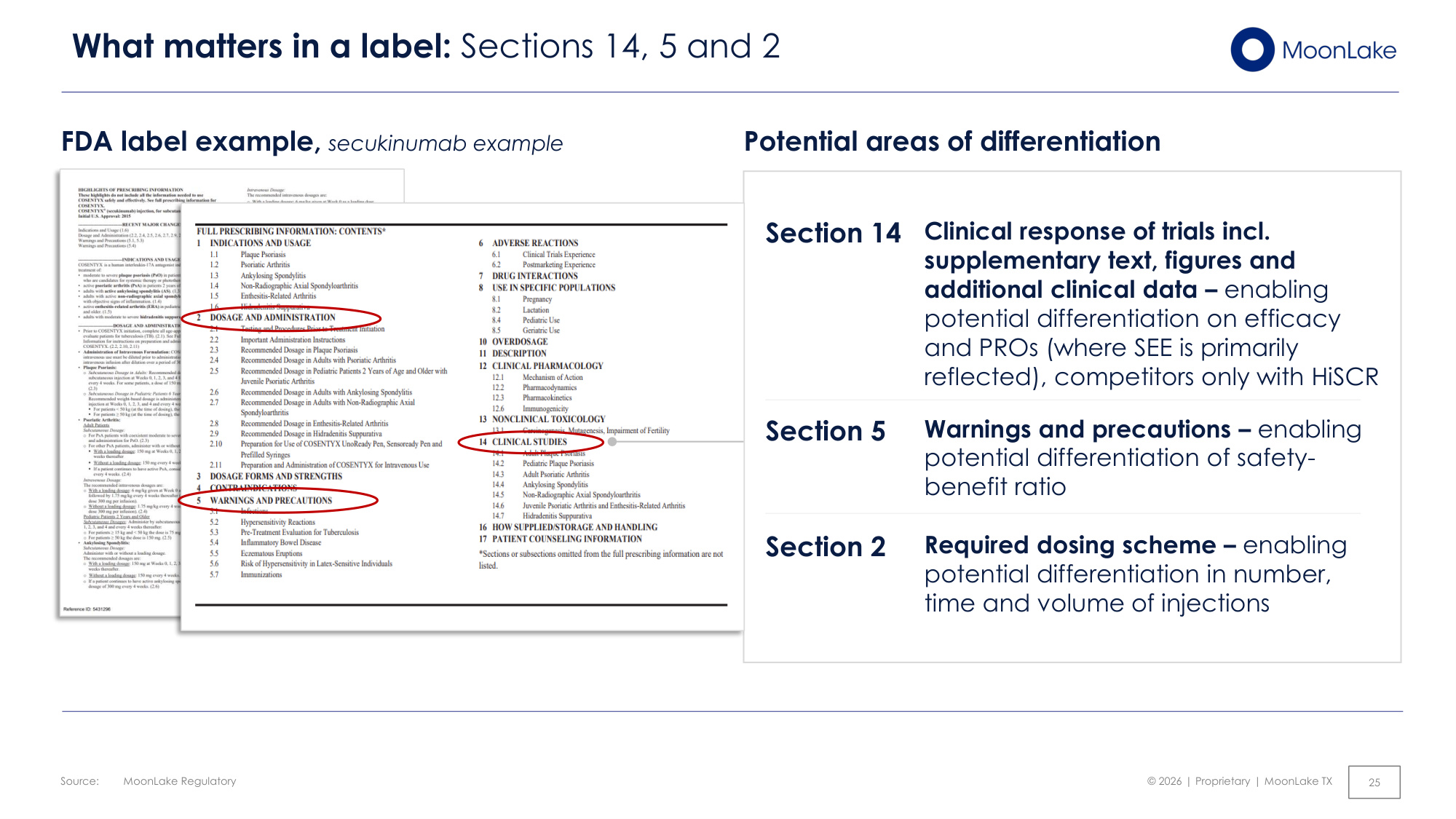
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 25 What matters in a label: Sections 14, 5 and 2 FDA label example, secukinumab example Potential areas of differentiation Clinical response of trials incl. supplementary text, figures and additional clinical data – enabling potential differentiation on efficacy and PROs (where SEE is primarily reflected), competitors only with HiSCR Section 14 Warnings and precautions – enabling potential differentiation of safety- benefit ratio Section 5 Required dosing scheme – enabling potential differentiation in number, time and volume of injections Section 2
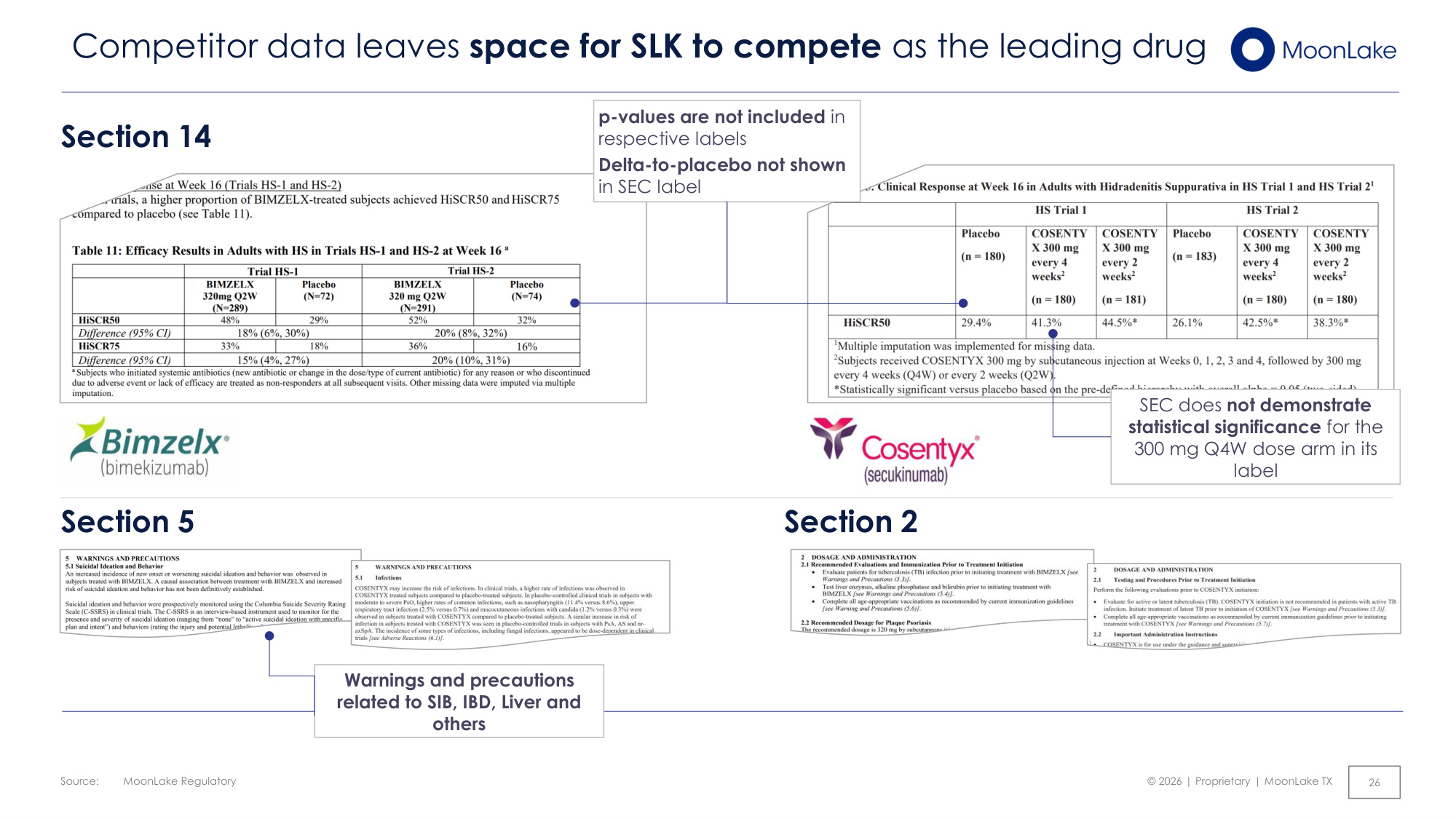
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 26 Competitor data leaves space for SLK to compete as the leading drug Section 5 Section 2 Section 14 p-values are not included in respective labels Delta-to-placebo not shown in SEC label SEC does not demonstrate statistical significance for the 300 mg Q4W dose arm in its label Warnings and precautions related to SIB, IBD, Liver and others
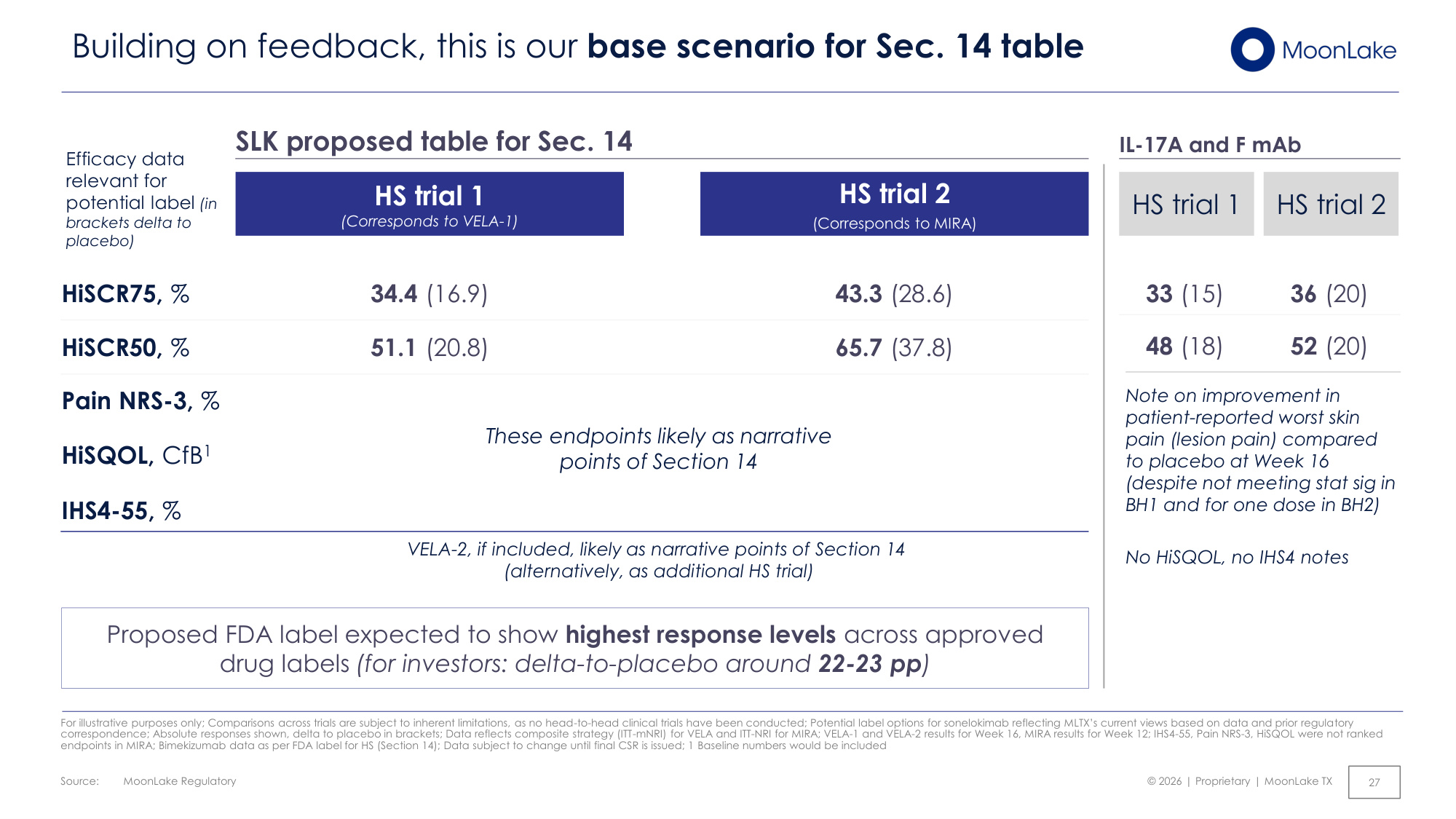
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 27 Building on feedback, this is our base scenario for Sec. 14 table For illustrative purposes only; Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; Potential label options for sonelokimab reflecting MLTX's current views based on data and prior regulatory correspondence; Absolute responses shown, delta to placebo in brackets; Data reflects composite strategy (ITT-mNRI) for VELA and ITT-NRI for MIRA; VELA-1 and VELA-2 results for Week 16, MIRA results for Week 12; IHS4-55, Pain NRS-3, HiSQOL were not ranked endpoints in MIRA; Bimekizumab data as per FDA label for HS (Section 14); Data subject to change until final CSR is issued; 1 Baseline numbers would be included SLK proposed table for Sec. 14 HS trial 1 (Corresponds to VELA-1) HS trial 2 (Corresponds to MIRA) HiSCR50, % 65.7 (37.8) 51.1 (20.8) HiSCR75, % 43.3 (28.6) 34.4 (16.9) Efficacy data relevant for potential label (in brackets delta to placebo) Pain NRS-3, % These endpoints likely as narrative points of Section 14 IHS4-55, % VELA-2, if included, likely as narrative points of Section 14 (alternatively, as additional HS trial) Note on improvement in patient-reported worst skin pain (lesion pain) compared to placebo at Week 16 (despite not meeting stat sig in BH1 and for one dose in BH2) No HiSQOL, no IHS4 notes 33 (15) 48 (18) 36 (20) 52 (20) IL-17A and F mAb HS trial 2 HS trial 1 Proposed FDA label expected to show highest response levels across approved drug labels (for investors: delta-to-placebo around 22-23 pp) HiSQOL, CfB1
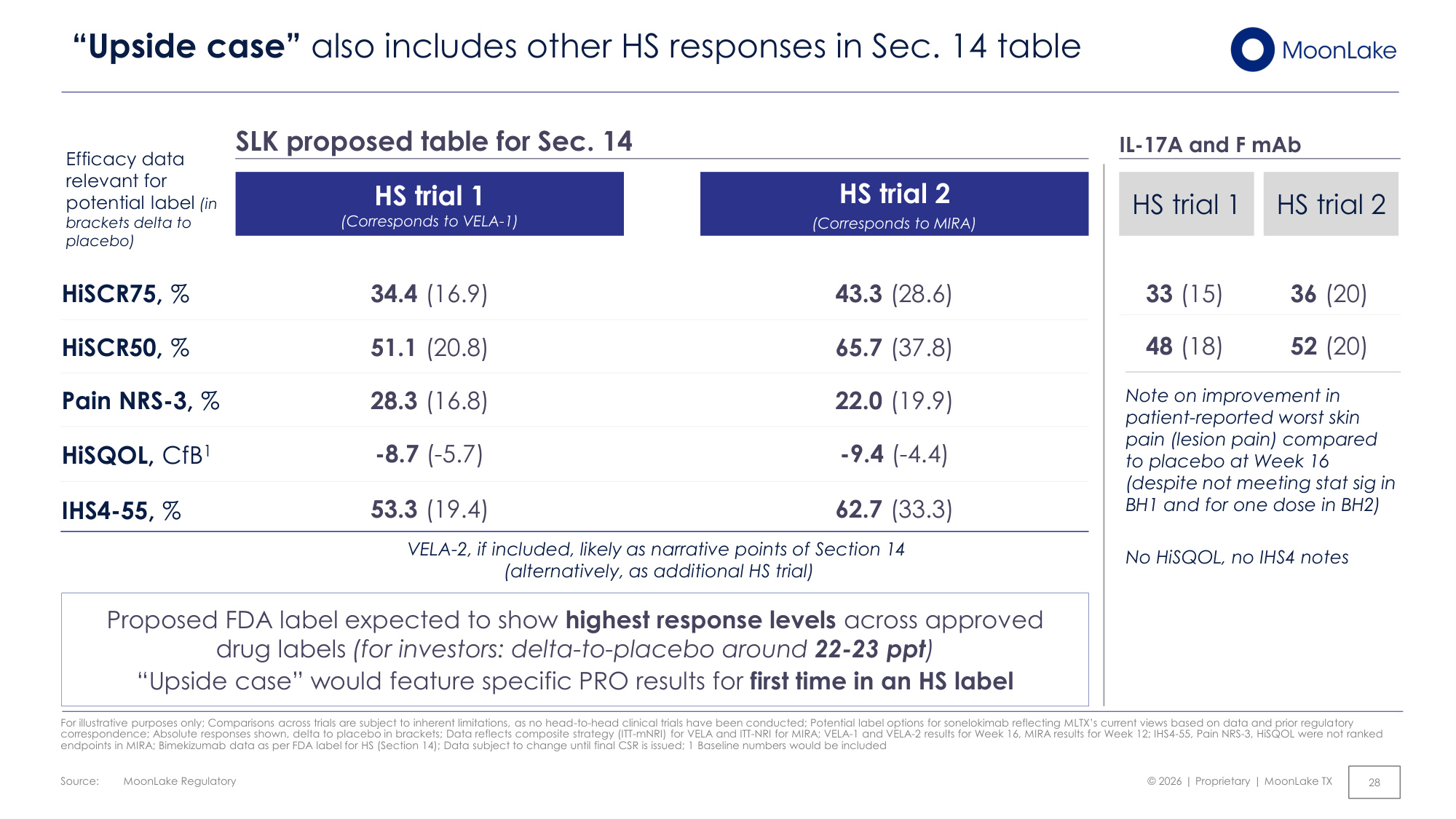
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 28 "Upside case" also includes other HS responses in Sec. 14 table Efficacy data relevant for potential label (in brackets delta to placebo) IHS4-55, % 53.3 (19.4) 62.7 (33.3) Pain NRS-3, % 28.3 (16.8) 22.0 (19.9) HiSQOL, CfB1 -8.7 (-5.7) -9.4 (-4.4) HS trial 1 (Corresponds to VELA-1) HS trial 2 (Corresponds to MIRA) HiSCR75, % 43.3 (28.6) 34.4 (16.9) HiSCR50, % 65.7 (37.8) 51.1 (20.8) For illustrative purposes only; Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; Potential label options for sonelokimab reflecting MLTX's current views based on data and prior regulatory correspondence; Absolute responses shown, delta to placebo in brackets; Data reflects composite strategy (ITT-mNRI) for VELA and ITT-NRI for MIRA; VELA-1 and VELA-2 results for Week 16, MIRA results for Week 12; IHS4-55, Pain NRS-3, HiSQOL were not ranked endpoints in MIRA; Bimekizumab data as per FDA label for HS (Section 14); Data subject to change until final CSR is issued; 1 Baseline numbers would be included Note on improvement in patient-reported worst skin pain (lesion pain) compared to placebo at Week 16 (despite not meeting stat sig in BH1 and for one dose in BH2) No HiSQOL, no IHS4 notes 33 (15) 48 (18) 36 (20) 52 (20) IL-17A and F mAb HS trial 2 HS trial 1 SLK proposed table for Sec. 14 VELA-2, if included, likely as narrative points of Section 14 (alternatively, as additional HS trial) Proposed FDA label expected to show highest response levels across approved drug labels (for investors: delta-to-placebo around 22-23 ppt) "Upside case" would feature specific PRO results for first time in an HS label
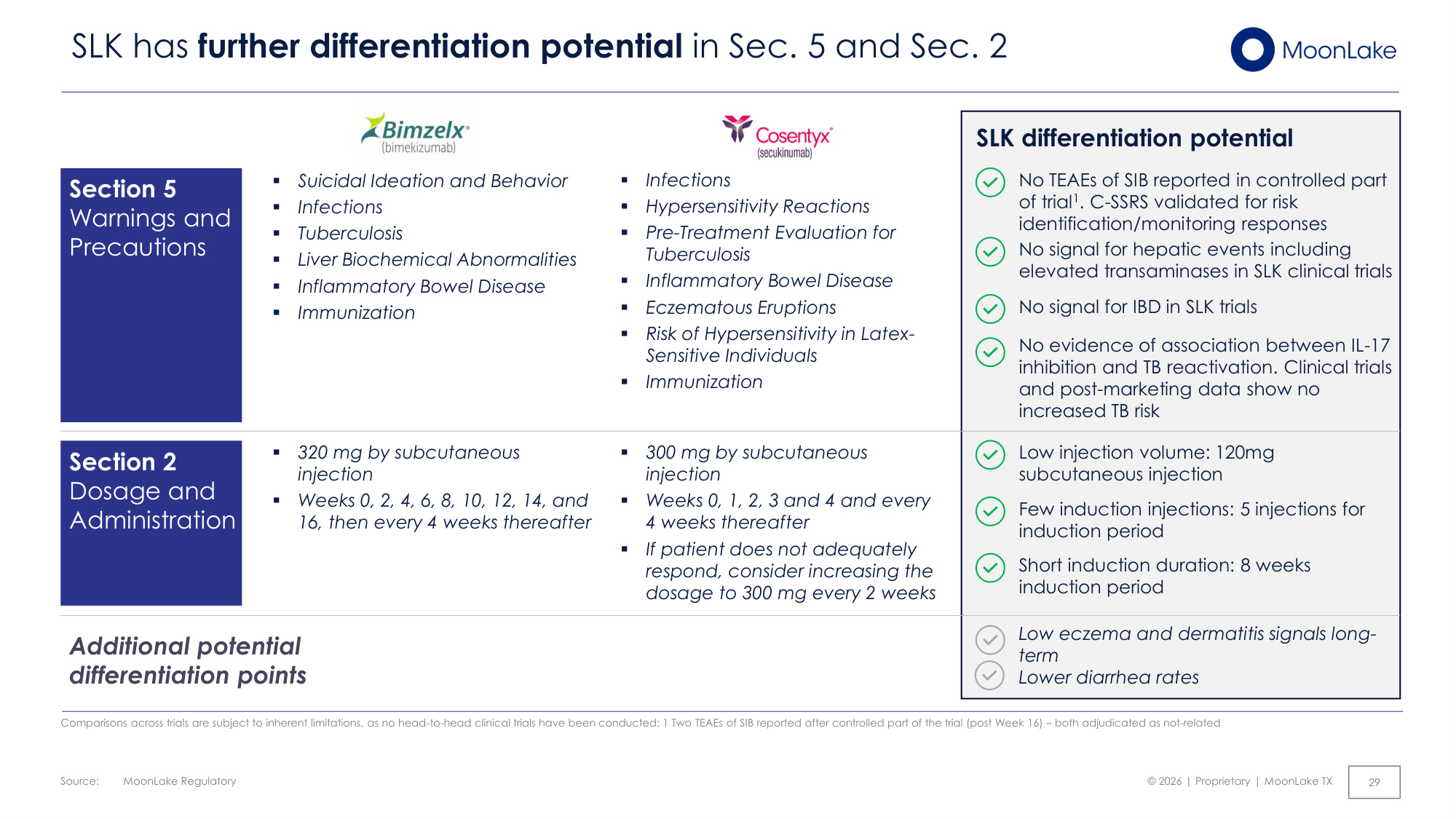
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 29 SLK has further differentiation potential in Sec. 5 and Sec. 2 SLK differentiation potential Section 5 Warnings and Precautions ▪ Suicidal Ideation and Behavior ▪ Infections ▪ Tuberculosis ▪ Liver Biochemical Abnormalities ▪ Inflammatory Bowel Disease ▪ Immunization ▪ Infections ▪ Hypersensitivity Reactions ▪ Pre-Treatment Evaluation for Tuberculosis ▪ Inflammatory Bowel Disease ▪ Eczematous Eruptions ▪ Risk of Hypersensitivity in Latex- Sensitive Individuals ▪ Immunization No evidence of association between IL-17 inhibition and TB reactivation. Clinical trials and post-marketing data show no increased TB risk No TEAEs of SIB reported in controlled part of trial1. C-SSRS validated for risk identification/monitoring responses No signal for hepatic events including elevated transaminases in SLK clinical trials Section 2 Dosage and Administration ▪ 320 mg by subcutaneous injection ▪ Weeks 0, 2, 4, 6, 8, 10, 12, 14, and 16, then every 4 weeks thereafter ▪ 300 mg by subcutaneous injection ▪ Weeks 0, 1, 2, 3 and 4 and every 4 weeks thereafter ▪ If patient does not adequately respond, consider increasing the dosage to 300 mg every 2 weeks Short induction duration: 8 weeks induction period Low injection volume: 120mg subcutaneous injection Few induction injections: 5 injections for induction period Low eczema and dermatitis signals long- term Lower diarrhea rates Additional potential differentiation points Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; 1 Two TEAEs of SIB reported after controlled part of the trial (post Week 16) – both adjudicated as not-related No signal for IBD in SLK trials
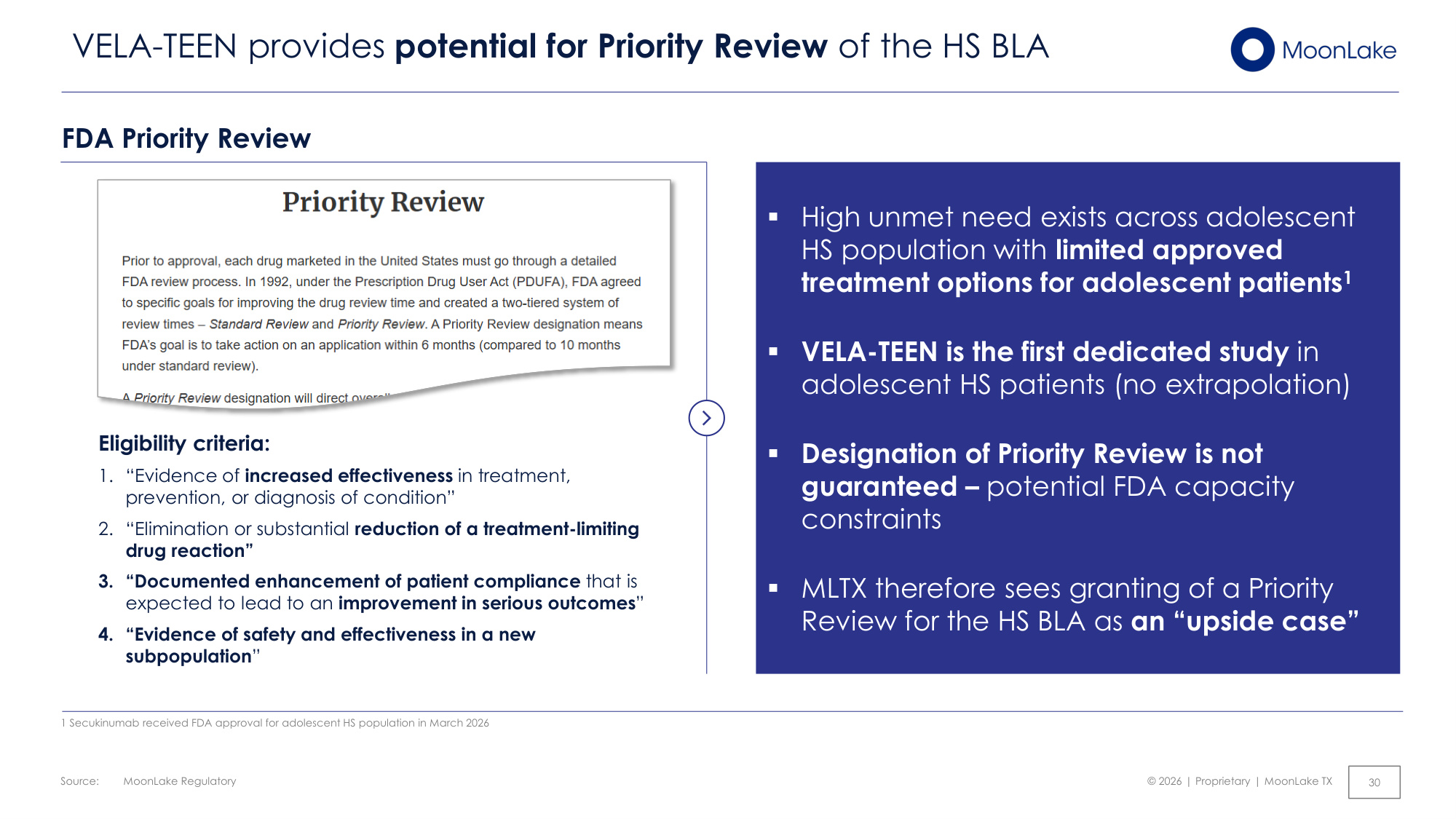
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 30 VELA-TEEN provides potential for Priority Review of the HS BLA 1 Secukinumab received FDA approval for adolescent HS population in March 2026 FDA Priority Review Eligibility criteria: 1. "Evidence of increased effectiveness in treatment, prevention, or diagnosis of condition" 2. "Elimination or substantial reduction of a treatment-limiting drug reaction" 3. "Documented enhancement of patient compliance that is expected to lead to an improvement in serious outcomes" 4. "Evidence of safety and effectiveness in a new subpopulation" ▪High unmet need exists across adolescent HS population with limited approved treatment options for adolescent patients1 ▪VELA-TEEN is the first dedicated study in adolescent HS patients (no extrapolation) ▪Designation of Priority Review is not guaranteed – potential FDA capacity constraints ▪MLTX therefore sees granting of a Priority Review for the HS BLA as an "upside case"
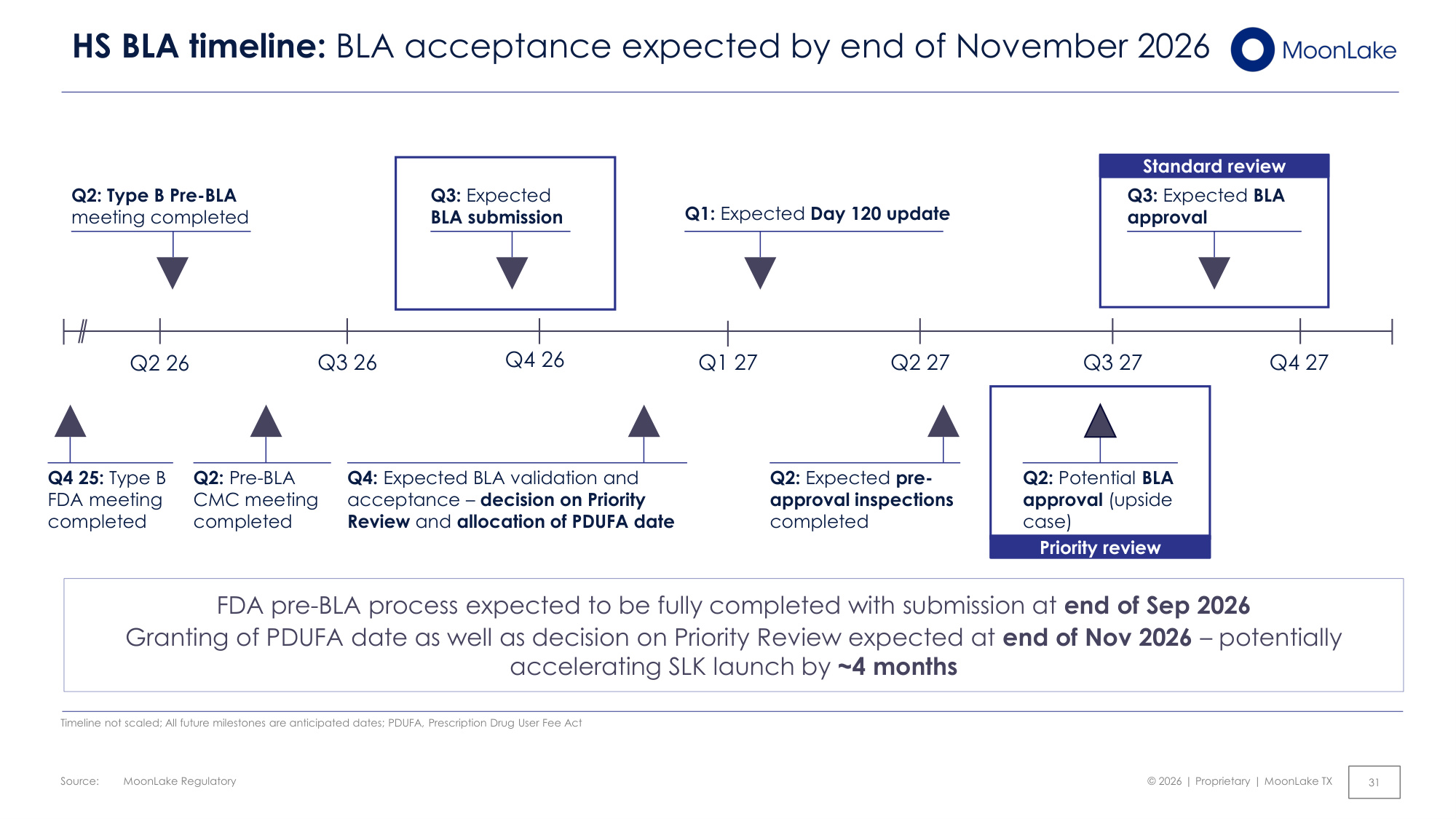
Source: © 2026 | Proprietary | MoonLake TX MoonLake Regulatory 31 HS BLA timeline: BLA acceptance expected by end of November 2026 FDA pre-BLA process expected to be fully completed with submission at end of Sep 2026 Granting of PDUFA date as well as decision on Priority Review expected at end of Nov 2026 – potentially accelerating SLK launch by ~4 months Q3 26 Q4 26 Q2 27 Q3 27 Q2 26 Q1 27 Q4 27 Q1: Expected Day 120 update Standard review Q3: Expected BLA approval Q2: Type B Pre-BLA meeting completed Q3: Expected BLA submission Q2: Expected pre- approval inspections completed Priority review Q2: Potential BLA approval (upside case) Q4: Expected BLA validation and acceptance – decision on Priority Review and allocation of PDUFA date Timeline not scaled; All future milestones are anticipated dates; PDUFA, Prescription Drug User Fee Act Q2: Pre-BLA CMC meeting completed Q4 25: Type B FDA meeting completed
© 2026 | Proprietary | MoonLake TX Commercializing SLK in HS 32
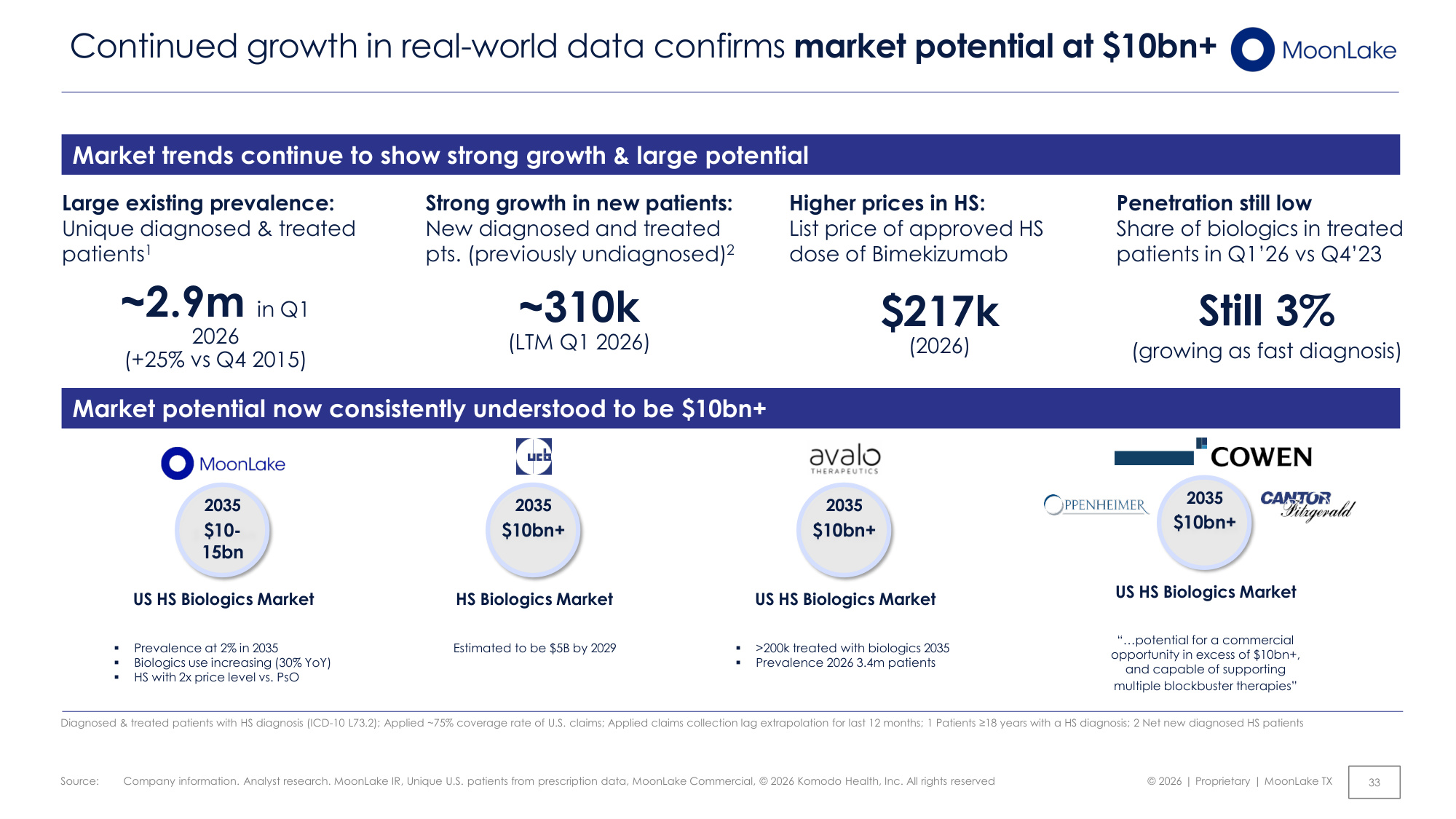
Source: © 2026 | Proprietary | MoonLake TX Company information. Analyst research. MoonLake IR, Unique U.S. patients from prescription data, MoonLake Commercial, © 2026 Komodo Health, Inc. All rights reserved 33 Continued growth in real-world data confirms market potential at $10bn+ Market trends continue to show strong growth & large potential Strong growth in new patients: New diagnosed and treated pts. (previously undiagnosed)2 Large existing prevalence: Unique diagnosed & treated patients1 ~2.9m in Q1 2026 (+25% vs Q4 2015) ~310k (LTM Q1 2026) Higher prices in HS: List price of approved HS dose of Bimekizumab $217k (2026) Market potential now consistently understood to be $10bn+ US HS Biologics Market ▪ Prevalence at 2% in 2035 ▪ Biologics use increasing (30% YoY) ▪ HS with 2x price level vs. PsO $10- 15bn 2035 HS Biologics Market Estimated to be $5B by 2029 $10bn+ 2035 US HS Biologics Market ▪ >200k treated with biologics 2035 ▪ Prevalence 2026 3.4m patients $10bn+ 2035 US HS Biologics Market "...potential for a commercial opportunity in excess of $10bn+, and capable of supporting multiple blockbuster therapies" $10bn+ 2035 Diagnosed & treated patients with HS diagnosis (ICD-10 L73.2); Applied ~75% coverage rate of U.S. claims; Applied claims collection lag extrapolation for last 12 months; 1 Patients ≥18 years with a HS diagnosis; 2 Net new diagnosed HS patients Penetration still low Share of biologics in treated patients in Q1'26 vs Q4'23 Still 3% (growing as fast diagnosis)
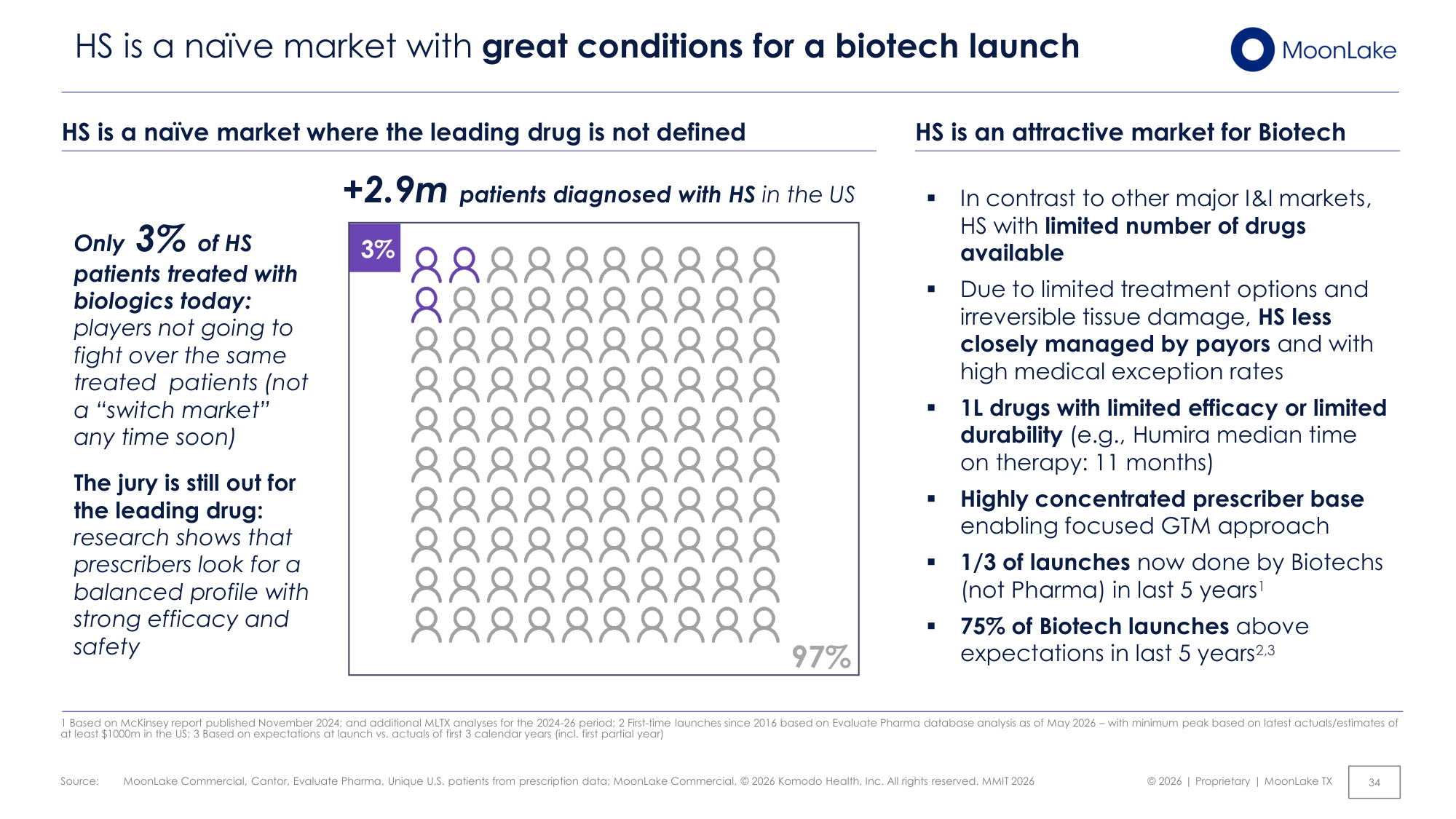
Source: © 2026 | Proprietary | MoonLake TX MoonLake Commercial, Cantor, Evaluate Pharma, Unique U.S. patients from prescription data; MoonLake Commercial, © 2026 Komodo Health, Inc. All rights reserved. MMIT 2026 34 +2.9m patients diagnosed with HS in the US Only 3% of HS patients treated with biologics today: players not going to fight over the same treated patients (not a "switch market" any time soon) The jury is still out for the leading drug: research shows that prescribers look for a balanced profile with strong efficacy and safety 3% HS is a naïve market with great conditions for a biotech launch 97% ▪ In contrast to other major I&I markets, HS with limited number of drugs available ▪ Due to limited treatment options and irreversible tissue damage, HS less closely managed by payors and with high medical exception rates ▪ 1L drugs with limited efficacy or limited durability (e.g., Humira median time on therapy: 11 months) ▪ Highly concentrated prescriber base enabling focused GTM approach ▪ 1/3 of launches now done by Biotechs (not Pharma) in last 5 years1 ▪ 75% of Biotech launches above expectations in last 5 years2,3 HS is a naïve market where the leading drug is not defined HS is an attractive market for Biotech 1 Based on McKinsey report published November 2024; and additional MLTX analyses for the 2024-26 period; 2 First-time launches since 2016 based on Evaluate Pharma database analysis as of May 2026 – with minimum peak based on latest actuals/estimates of at least $1000m in the US; 3 Based on expectations at launch vs. actuals of first 3 calendar years (incl. first partial year)
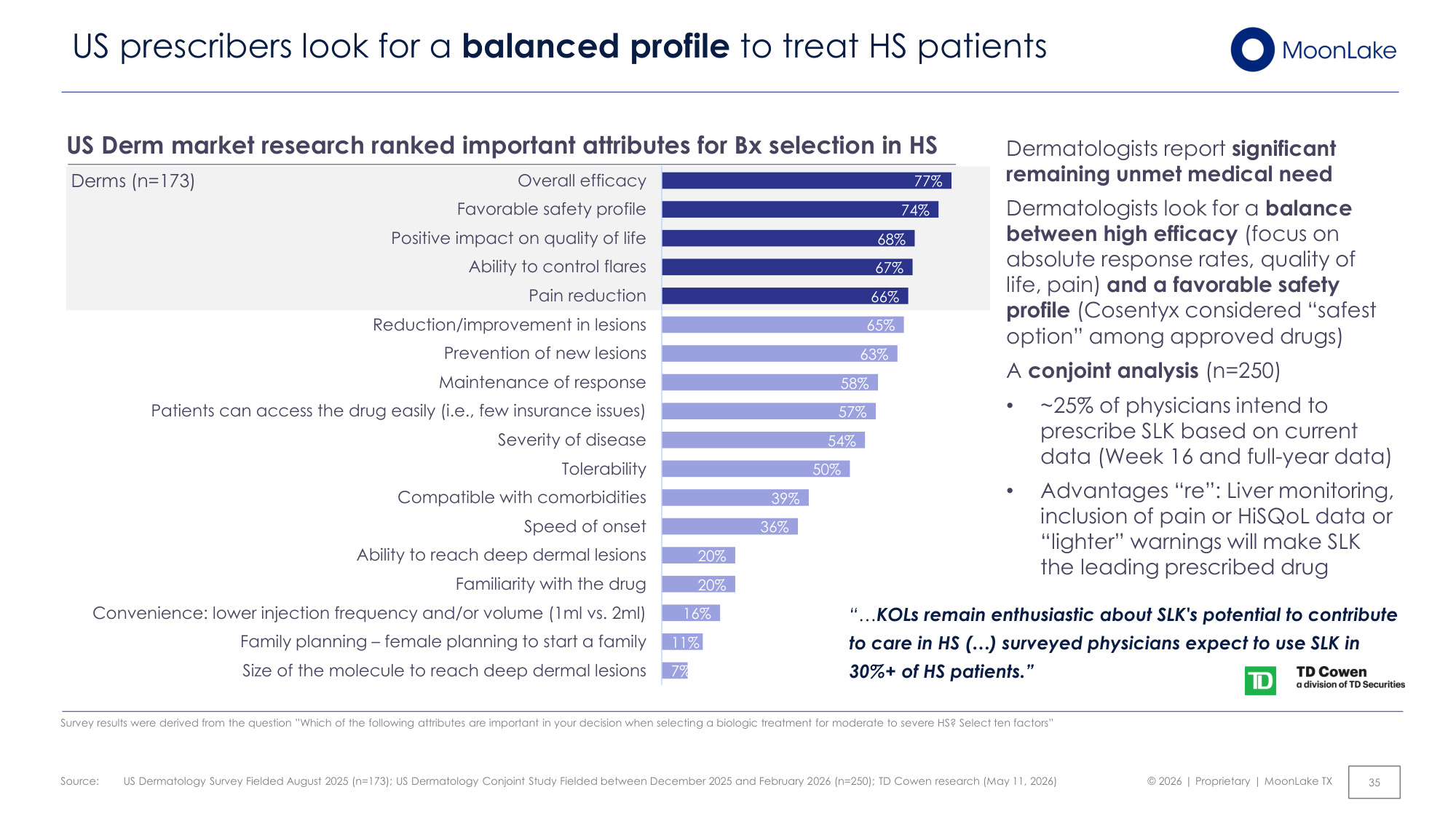
Source: © 2026 | Proprietary | MoonLake TX 77% 74% 68% 67% 66% 65% 63% 58% 57% 54% 50% 39% 36% 20% 20% 16% 11% 7% Overall efficacy Favorable safety profile Positive impact on quality of life Ability to control flares Pain reduction Reduction/improvement in lesions Prevention of new lesions Maintenance of response Patients can access the drug easily (i.e., few insurance issues) Severity of disease Tolerability Compatible with comorbidities Speed of onset Ability to reach deep dermal lesions Familiarity with the drug Convenience: lower injection frequency and/or volume (1ml vs. 2ml) Family planning – female planning to start a family Size of the molecule to reach deep dermal lesions US Dermatology Survey Fielded August 2025 (n=173); US Dermatology Conjoint Study Fielded between December 2025 and February 2026 (n=250); TD Cowen research (May 11, 2026) US Derm market research ranked important attributes for Bx selection in HS Dermatologists report significant remaining unmet medical need Dermatologists look for a balance between high efficacy (focus on absolute response rates, quality of life, pain) and a favorable safety profile (Cosentyx considered "safest option" among approved drugs) A conjoint analysis (n=250) • ~25% of physicians intend to prescribe SLK based on current data (Week 16 and full-year data) • Advantages "re": Liver monitoring, inclusion of pain or HiSQoL data or "lighter" warnings will make SLK the leading prescribed drug Derms (n=173) US prescribers look for a balanced profile to treat HS patients 35 Survey results were derived from the question "Which of the following attributes are important in your decision when selecting a biologic treatment for moderate to severe HS? Select ten factors" "...KOLs remain enthusiastic about SLK's potential to contribute to care in HS (...) surveyed physicians expect to use SLK in 30%+ of HS patients."
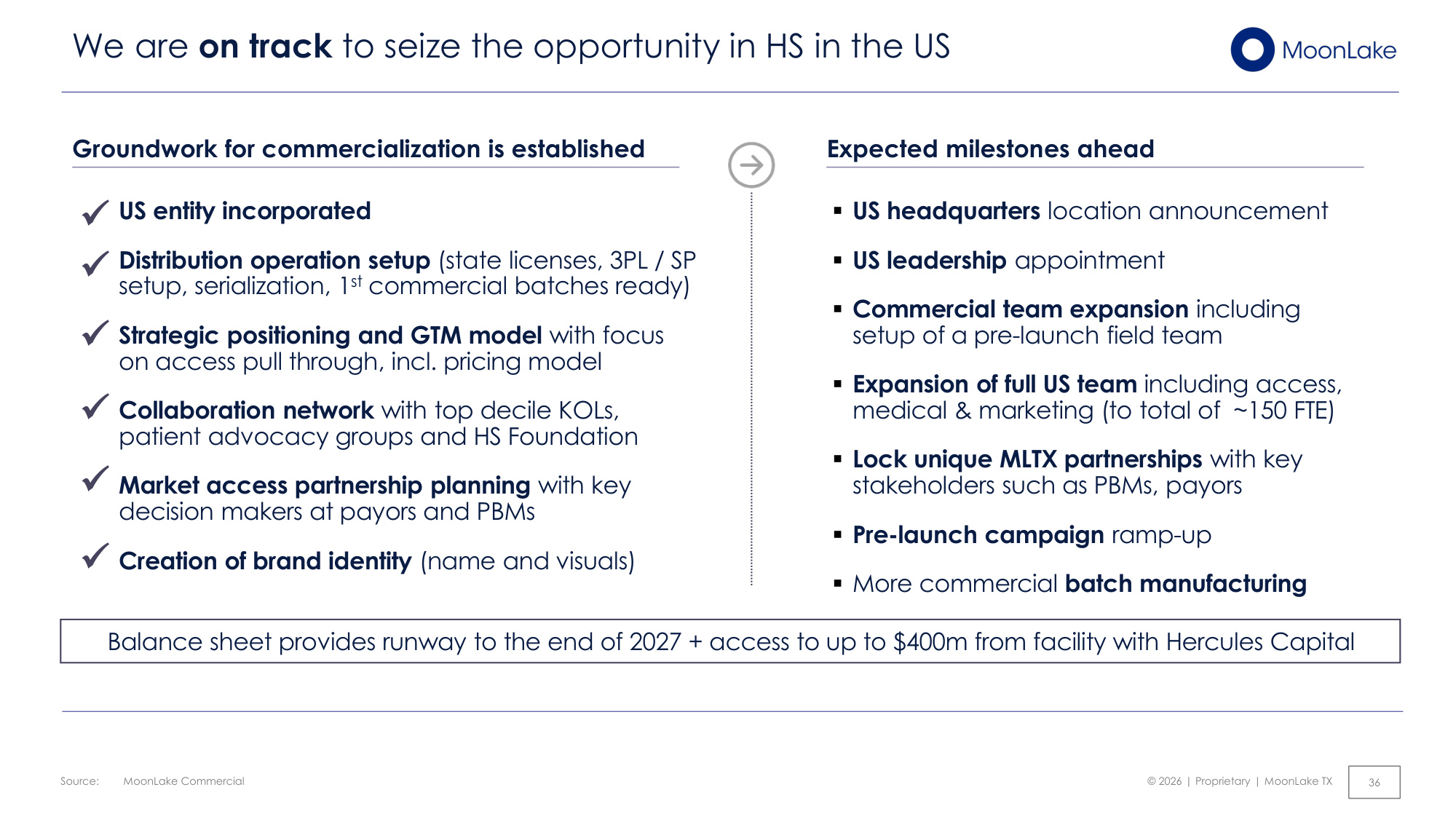
Source: © 2026 | Proprietary | MoonLake TX MoonLake Commercial 36 We are on track to seize the opportunity in HS in the US ▪US entity incorporated ▪Distribution operation setup (state licenses, 3PL / SP setup, serialization, 1st commercial batches ready) ▪Strategic positioning and GTM model with focus on access pull through, incl. pricing model ▪Collaboration network with top decile KOLs, patient advocacy groups and HS Foundation ▪Market access partnership planning with key decision makers at payors and PBMs ▪Creation of brand identity (name and visuals) Groundwork for commercialization is established ▪US headquarters location announcement ▪US leadership appointment ▪Commercial team expansion including setup of a pre-launch field team ▪Expansion of full US team including access, medical & marketing (to total of ~150 FTE) ▪Lock unique MLTX partnerships with key stakeholders such as PBMs, payors ▪Pre-launch campaign ramp-up ▪More commercial batch manufacturing Expected milestones ahead ✓ ✓ ✓ ✓ ✓ Balance sheet provides runway to the end of 2027 + access to up to $400m from facility with Hercules Capital ✓

© 2026 | Proprietary | MoonLake TX Closing remarks 37
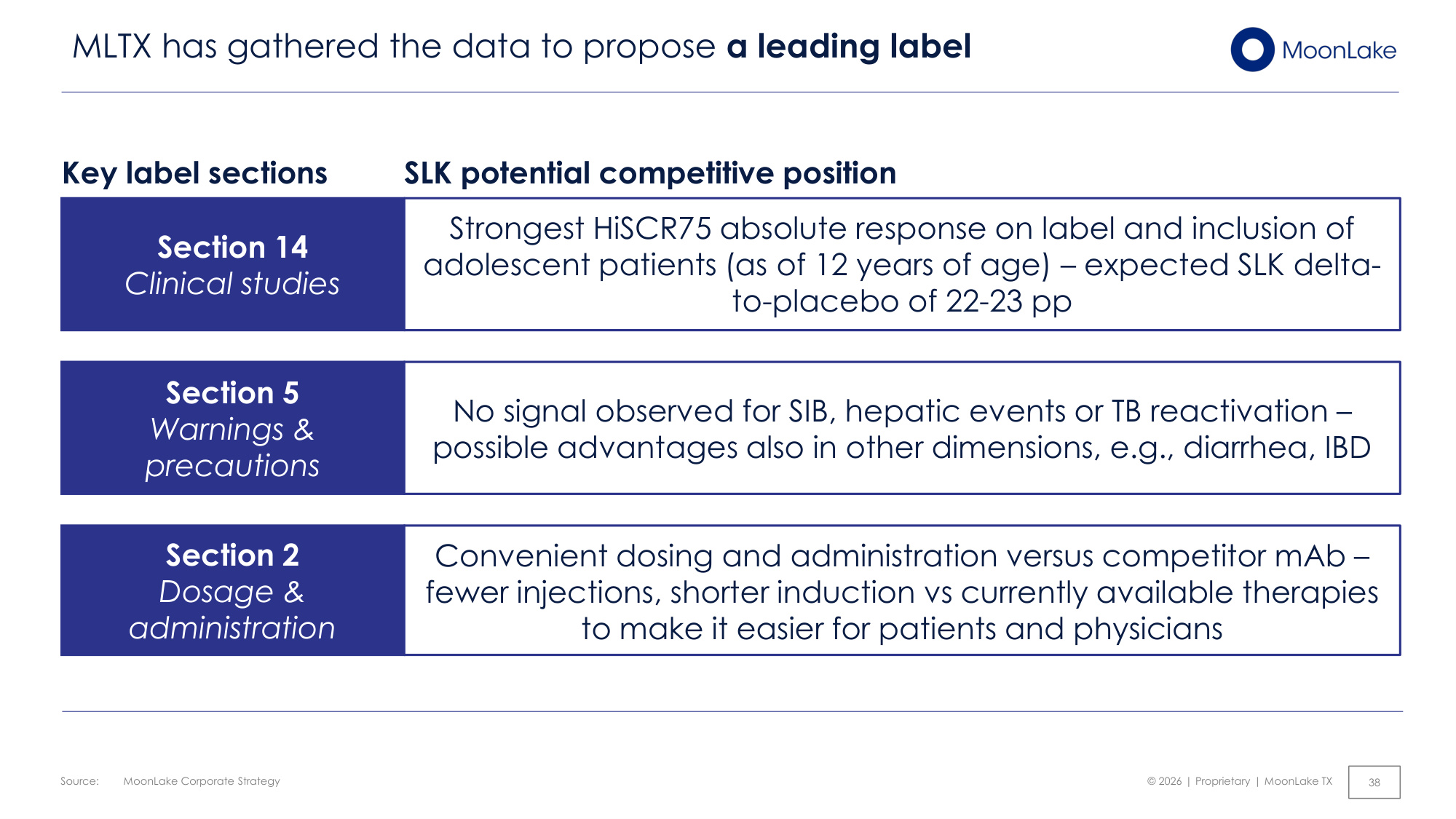
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 38 MLTX has gathered the data to propose a leading label Section 5 Warnings & precautions No signal observed for SIB, hepatic events or TB reactivation – possible advantages also in other dimensions, e.g., diarrhea, IBD Section 2 Dosage & administration Convenient dosing and administration versus competitor mAb – fewer injections, shorter induction vs currently available therapies to make it easier for patients and physicians Section 14 Clinical studies Strongest HiSCR75 absolute response on label and inclusion of adolescent patients (as of 12 years of age) – expected SLK delta- to-placebo of 22-23 pp Key label sections SLK potential competitive position
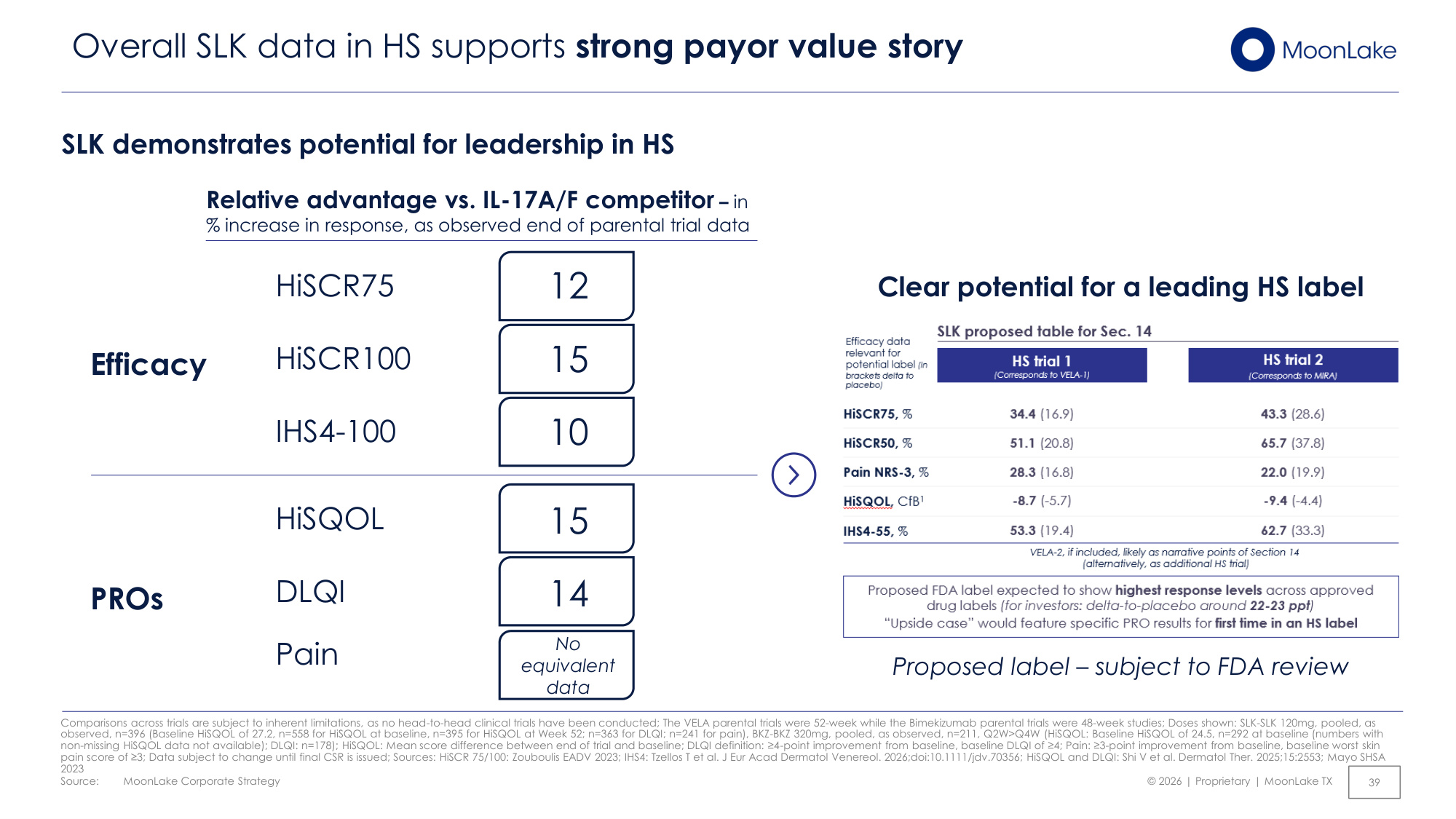
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 39 Overall SLK data in HS supports strong payor value story Comparisons across trials are subject to inherent limitations, as no head-to-head clinical trials have been conducted; The VELA parental trials were 52-week while the Bimekizumab parental trials were 48-week studies; Doses shown: SLK-SLK 120mg, pooled, as observed, n=396 (Baseline HiSQOL of 27.2, n=558 for HiSQOL at baseline, n=395 for HiSQOL at Week 52; n=363 for DLQI; n=241 for pain), BKZ-BKZ 320mg, pooled, as observed, n=211, Q2W>Q4W (HiSQOL: Baseline HiSQOL of 24.5, n=292 at baseline (numbers with non-missing HiSQOL data not available); DLQI: n=178); HiSQOL: Mean score difference between end of trial and baseline; DLQI definition: ≥4-point improvement from baseline, baseline DLQI of ≥4; Pain: ≥3-point improvement from baseline, baseline worst skin pain score of ≥3; Data subject to change until final CSR is issued; Sources: HiSCR 75/100: Zouboulis EADV 2023; IHS4: Tzellos T et al. J Eur Acad Dermatol Venereol. 2026;doi:10.1111/jdv.70356; HiSQOL and DLQI: Shi V et al. Dermatol Ther. 2025;15:2553; Mayo SHSA 2023 SLK demonstrates potential for leadership in HS Efficacy PROs Relative advantage vs. IL-17A/F competitor – in % increase in response, as observed end of parental trial data HiSCR100 DLQI IHS4-100 HiSQOL Pain 15 10 15 14 HiSCR75 12 No equivalent data Clear potential for a leading HS label Proposed label – subject to FDA review
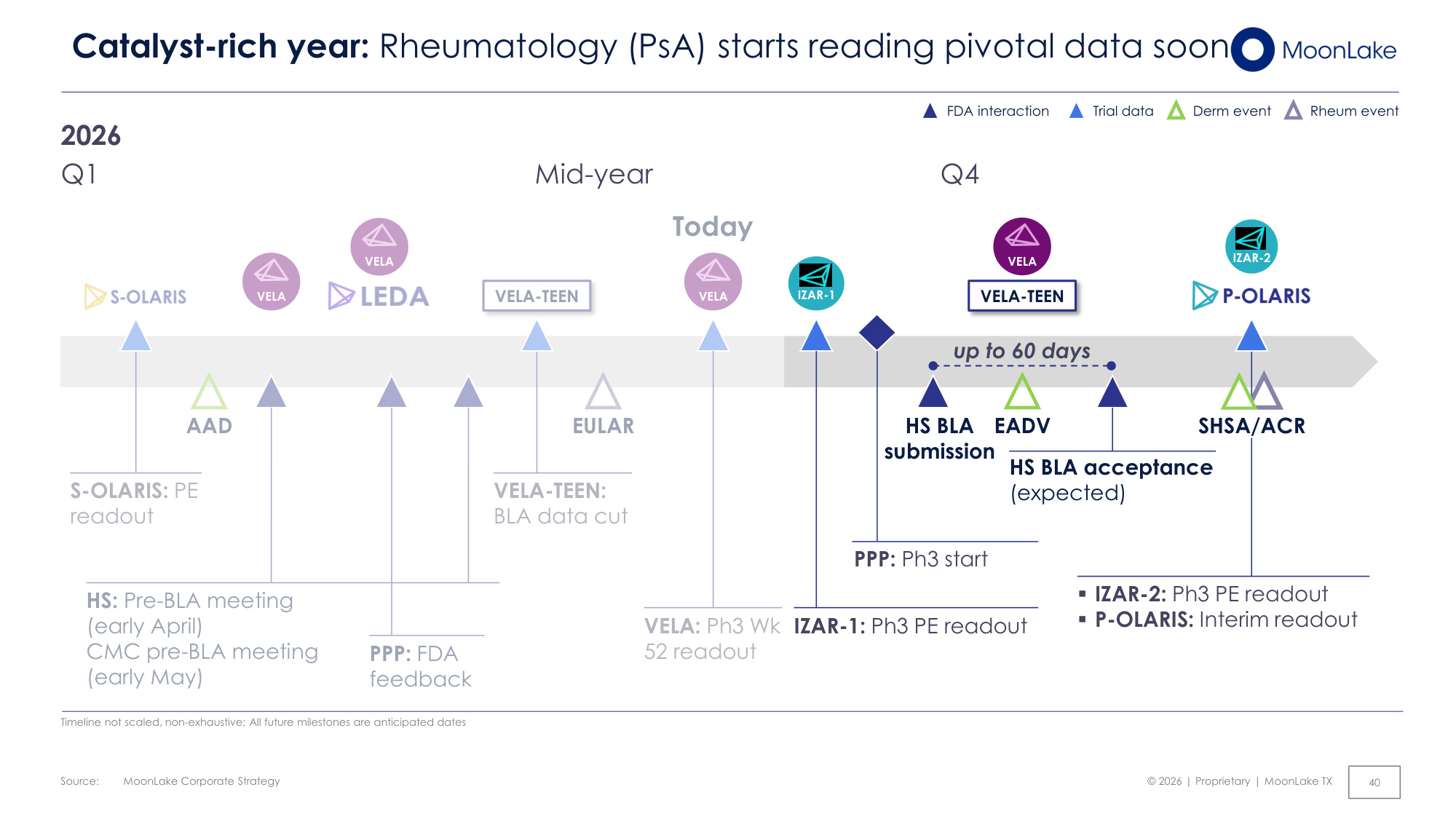
Source: © 2026 | Proprietary | MoonLake TX Today MoonLake Corporate Strategy 40 Catalyst-rich year: Rheumatology (PsA) starts reading pivotal data soon FDA interaction Trial data Timeline not scaled, non-exhaustive; All future milestones are anticipated dates 2026 up to 60 days ▪IZAR-2: Ph3 PE readout ▪P-OLARIS: Interim readout IZAR-1: Ph3 PE readout Q1 Q4 IZAR-2 Derm event Rheum event AAD VELA HS: Pre-BLA meeting (early April) CMC pre-BLA meeting (early May) PPP: FDA feedback EADV HS BLA submission VELA-TEEN VELA SHSA/ACR VELA-TEEN VELA-TEEN: BLA data cut S-OLARIS: PE readout IZAR-1 EULAR VELA VELA: Ph3 Wk 52 readout VELA Mid-year HS BLA acceptance (expected) PPP: Ph3 start
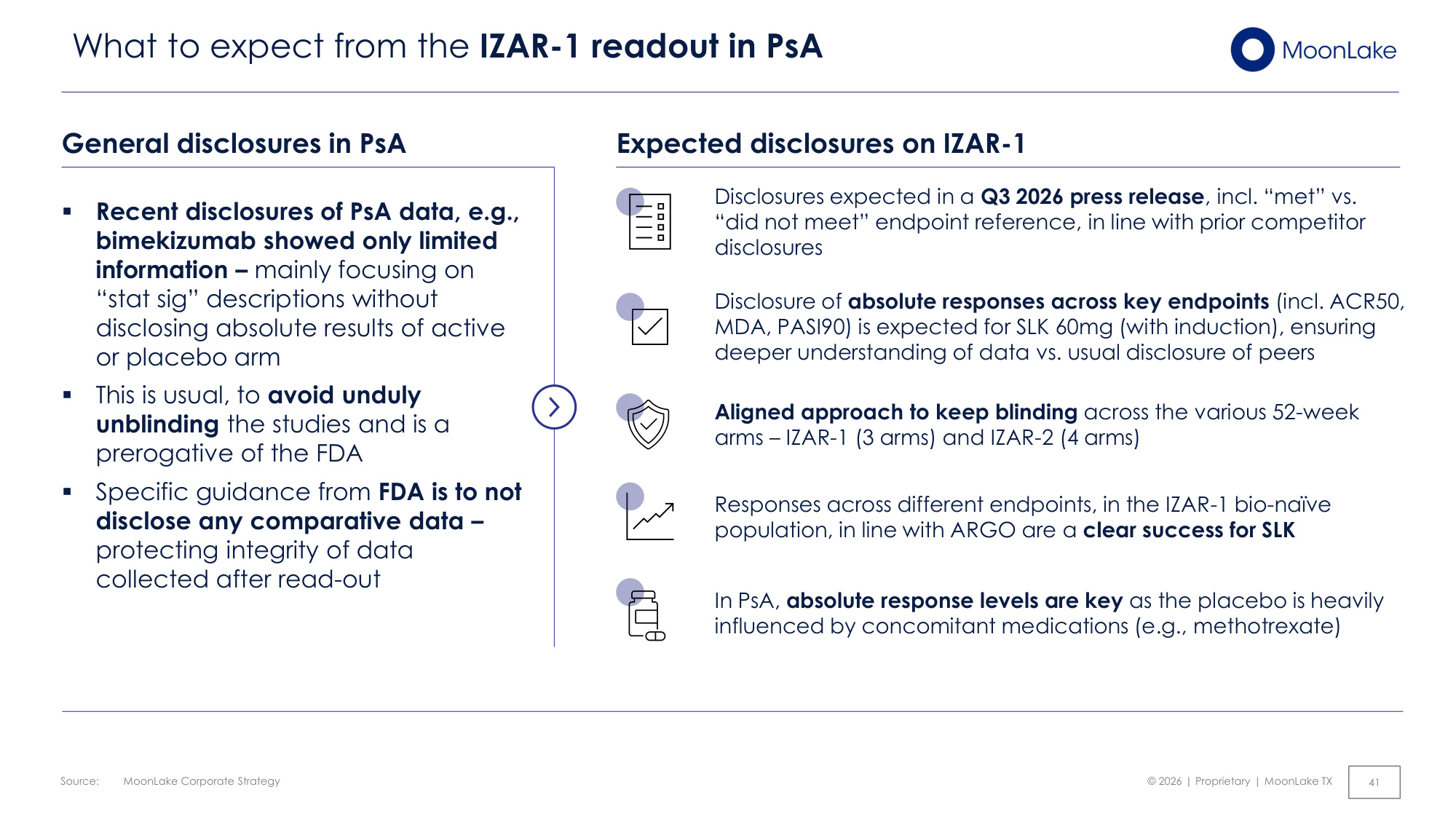
Source: © 2026 | Proprietary | MoonLake TX MoonLake Corporate Strategy 41 What to expect from the IZAR-1 readout in PsA General disclosures in PsA ▪ Recent disclosures of PsA data, e.g., bimekizumab showed only limited information – mainly focusing on "stat sig" descriptions without disclosing absolute results of active or placebo arm ▪ This is usual, to avoid unduly unblinding the studies and is a prerogative of the FDA ▪ Specific guidance from FDA is to not disclose any comparative data – protecting integrity of data collected after read-out Expected disclosures on IZAR-1 Disclosures expected in a Q3 2026 press release, incl. "met" vs. "did not meet" endpoint reference, in line with prior competitor disclosures In PsA, absolute response levels are key as the placebo is heavily influenced by concomitant medications (e.g., methotrexate) Aligned approach to keep blinding across the various 52-week arms – IZAR-1 (3 arms) and IZAR-2 (4 arms) Disclosure of absolute responses across key endpoints (incl. ACR50, MDA, PASI90) is expected for SLK 60mg (with induction), ensuring deeper understanding of data vs. usual disclosure of peers Responses across different endpoints, in the IZAR-1 bio-naïve population, in line with ARGO are a clear success for SLK
© 2026 | Proprietary | MoonLake TX Q & A Please submit your questions via the dedicated Q&A function in the portal
