Apparent sadness Reported sadness Concentration difficulty Lassitude Inability to feel Mean (SD) Change
from Baseline in MADRS Anhedonia Factor Items at Day 8 Results Disposition and Baseline Characteristics Disposition and baseline characteristics are presented in Table 1 Mean (SD) total MADRS scores at baseline were 29.0 (5.4) for GH001 and
28.2 (4.6) for placebo. Baseline MADRS anhedonia factor scores were 17.6 (3.2) for GH001 and 17.4 (2.6) for placebo Table 1. Patient Disposition and Baseline Characteristics Background Anhedonia is a transdiagnostic feature of depressive
disorders, characterized by a lack of enjoyment from and engagement in life’s experiences, and a deficit in the ability to feel pleasure. It is recognized as a core symptom of major depressive disorder (MDD)1 Improvement in anhedonia symptoms
in patients with MDD has been correlated with improvements in physical, psychological, and social functioning and quality of life2,3 GH001, a synthetic formulation of mebufotenin (5-MeO-DMT) administered via pulmonary inhalation, was evaluated
for efficacy and safety in a Phase 2b clinical trial (NCT05800860) in patients with treatment-resistant depression (TRD)4 GH001 showed rapid reductions in Montgomery-Åsberg Depression Rating Scale (MADRS) total scores, with a least squares
mean difference of -15.5 points vs placebo at Day 8 (P<0.0001)4 Objective This post-hoc analysis examined the effect of treatment with GH001 on MADRS anhedonia factor in patients with TRD Methods The trial design has been previously
reported and is summarized in Figure 1 Rater-based MADRS assessments were performed at Day 1 (baseline and 2 hours post-dose), Day 2 and Day 8 after each treatment, and all scheduled open-label extension (OLE) visits (Day 15 and monthly up to
Month 6/end of treatment) Anhedonia was assessed using the rater-based MADRS 5-item anhedonia factor (items 1: apparent sadness; 2: reported sadness; 6: concentration difficulties; 7: lassitude; 8: inability to feel; score range: 0-30, with
lower scores indicating less severe MADRS anhedonia factor) This MADRS anhedonia factor includes items that overlap with general depressive severity Clinically meaningful improvement was defined using a published minimal clinically important
change (MCIC) threshold of -4.6 to -5.5 points for patients with MDD3 This post hoc analysis summarizes MADRS anhedonia factor scores descriptively (mean [SD] changes from baseline); all P-values shown are nominal (unadjusted for multiple
comparisons) Figure 1. Clinical Trial Design References American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013. Cao B, et al. Front Psychiatry. 2019;10:17.
McIntyre RS, et al. J Affect Disord. 2024;363:430-435. Cubała WJ, et al. JAMA Psychiatry. Published online March 25, 2026. doi:10.1001/jamapsychiatry.2026.0096. Acknowledgments This trial was sponsored by GH Research Ireland Limited. The
sponsor would like to thank the participants in the trial. The sponsor would also like to thank the investigators who conducted this trial. Under the guidance of the authors, medical writing and editorial support were provided by Brian Brennan,
PhD, of GH Research. Disclosures Presenting Author : RSMcI: Research Grants: CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute; Speaker/Consultation Fees: Lundbeck, Janssen, Alkermes, Neumora
Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Neurawell, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris,
Abbvie, Bristol Myers Squibb and Atai Life Sciences. Presented at the American Society of Clinical Psychopharmacology Annual Meeting | Miami, FL, USA | May 26−29, 2026 Conclusions Patients with TRD receiving GH001 achieved rapid and large
reductions in MADRS anhedonia factor scores (Cohen’s d=-2.00 vs placebo at Day 8) that exceeded the MCIC at all assessed time points in the double-blind part, with sustained improvements by patients who completed the 6-month OLE after
infrequent treatment These findings suggests GH001 enhance patients' ability to experience pleasure, with potential implications for the physical, psychological, and social functioning deficits associated with anhedonia Roger S. McIntyre1,
Nathan P. Burns2, Wiesław J. Cubała3, Kelly Doolin2, Lisa Harding4,5, Velichka Valcheva2, Michael E. Thase6,7 1Department of Psychiatry, University of Toronto, Toronto, ON, Canada. 2GH Research, Dublin, Ireland. 3Department of Psychiatry,
Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland. 4Mood Institute, Milton, CT, USA. 5Department of Psychiatry, Yale School of Medicine, New Haven, CT, USA. 6Department of Psychiatry, University of Pennsylvania, Philadelphia,
PA, USA. 7Corporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA. Rapid and Sustained Improvement in Anhedonia Following Inhaled Mebufotenin (GH001) Treatment in Patients With Treatment-Resistant Depression aA
second or third dose was administered if the previous dose was well tolerated according to the trial physician’s judgement (based on vital signs and adverse events) and if the patient did not achieve an intense psychoactive effect (peak
experience; defined as a mean score of ≥75 on the Peak Experience Scale) following the previous dose. bEfficacy assessments were carried out by independent blinded raters in the double-blind part. cPatients also attended assessment visits on
Day 2 (telephone call) and Day 8 (in-person) after each re-treatment. Abbreviations: BL = Baseline; D = Day; H = Hour; IDR = Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale. aAll patients completed the
double-blind part of the trial and transitioned directly to the OLE. Patients could receive up to five GH001 IDR treatments in the OLE. Abbreviations: BMI = Body mass index; HAM-D-17 = 17-item Hamilton Depression Rating Scale; IDR =
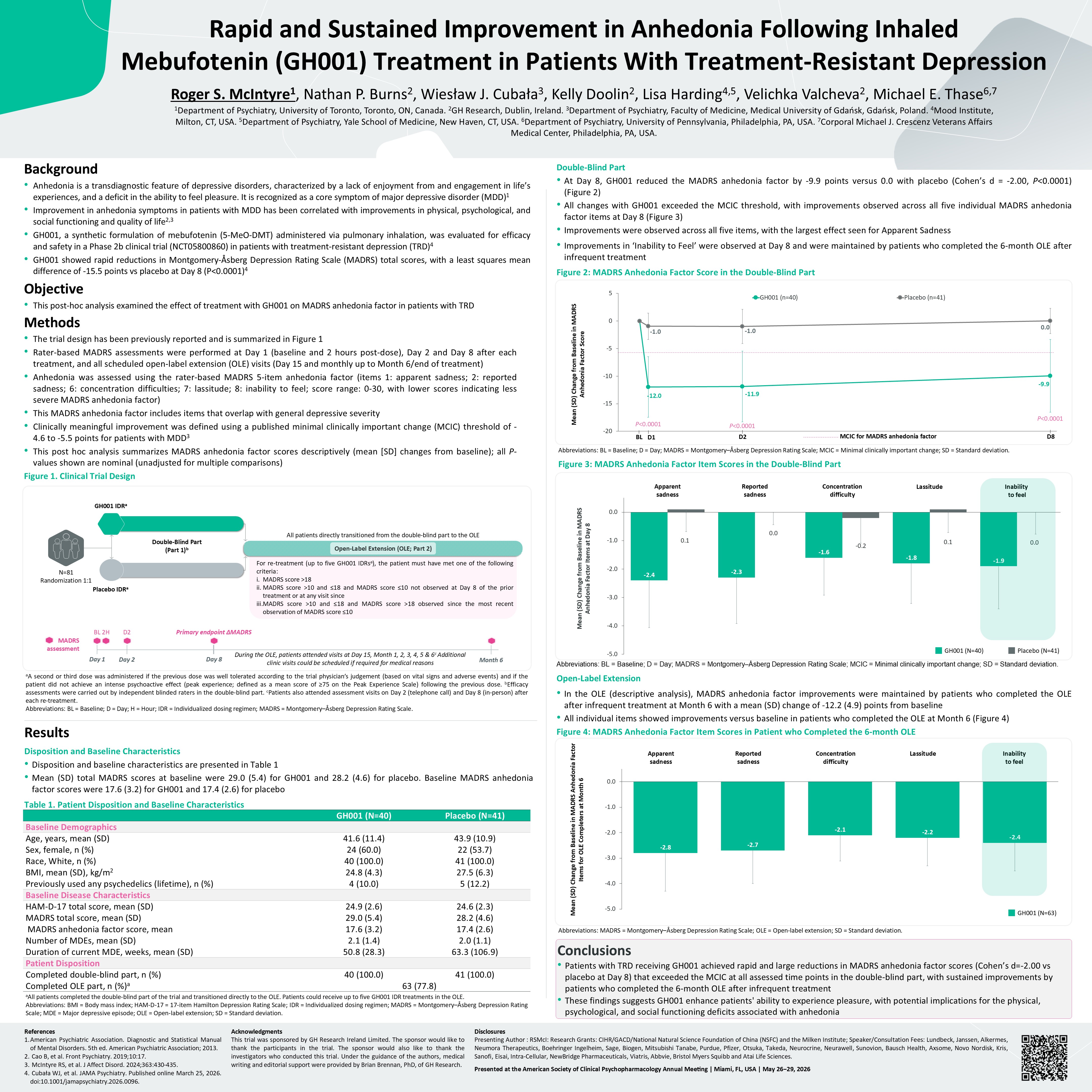
Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale; MDE = Major depressive episode; OLE = Open-label extension; SD = Standard deviation. Double-Blind Part At Day 8, GH001 reduced the MADRS anhedonia factor by
-9.9 points versus 0.0 with placebo (Cohen’s d = -2.00, P<0.0001) (Figure 2) All changes with GH001 exceeded the MCIC threshold, with improvements observed across all five individual MADRS anhedonia factor items at Day 8 (Figure
3) Improvements were observed across all five items, with the largest effect seen for Apparent Sadness Improvements in ‘Inability to Feel’ were observed at Day 8 and were maintained by patients who completed the 6-month OLE after infrequent
treatment Figure 2: MADRS Anhedonia Factor Score in the Double-Blind Part Abbreviations: BL = Baseline; D = Day; MADRS = Montgomery–Åsberg Depression Rating Scale; MCIC = Minimal clinically important change; SD = Standard deviation. Figure
3: MADRS Anhedonia Factor Item Scores in the Double-Blind Part Abbreviations: BL = Baseline; D = Day; MADRS = Montgomery–Åsberg Depression Rating Scale; MCIC = Minimal clinically important change; SD = Standard deviation. Open-Label
Extension In the OLE (descriptive analysis), MADRS anhedonia factor improvements were maintained by patients who completed the OLE after infrequent treatment at Month 6 with a mean (SD) change of -12.2 (4.9) points from baseline All
individual items showed improvements versus baseline in patients who completed the OLE at Month 6 (Figure 4) Figure 4: MADRS Anhedonia Factor Item Scores in Patient who Completed the 6-month OLE Abbreviations: MADRS = Montgomery–Åsberg
Depression Rating Scale; OLE = Open-label extension; SD = Standard deviation. During the OLE, patients attended visits at Day 15, Month 1, 2, 3, 4, 5 & 6c Additional clinic visits could be scheduled if required for medical reasons For
re-treatment (up to five GH001 IDRsa), the patient must have met one of the following criteria: MADRS score >18 MADRS score >10 and ≤18 and MADRS score ≤10 not observed at Day 8 of the prior treatment or at any visit since MADRS
score >10 and ≤18 and MADRS score >18 observed since the most recent observation of MADRS score ≤10 Open-Label Extension (OLE; Part 2) N=81 Randomization 1:1 Double-Blind Part (Part 1)b All patients directly transitioned from the
double-blind part to the OLE Placebo IDRa GH001 IDRa BL 2H Day 1 Primary endpoint ΔMADRS Day 8 MADRS assessment Month 6 D2 Day 2 GH001 (N=40) Placebo (N=41) Baseline Demographics Age, years, mean (SD) 41.6 (11.4) 43.9
(10.9) Sex, female, n (%) 24 (60.0) 22 (53.7) Race, White, n (%) 40 (100.0) 41 (100.0) BMI, mean (SD), kg/m2 24.8 (4.3) 27.5 (6.3) Previously used any psychedelics (lifetime), n (%) 4 (10.0) 5 (12.2) Baseline Disease
Characteristics HAM-D-17 total score, mean (SD) 24.9 (2.6) 24.6 (2.3) MADRS total score, mean (SD) 29.0 (5.4) 28.2 (4.6) MADRS anhedonia factor score, mean 17.6 (3.2) 17.4 (2.6) Number of MDEs, mean (SD) 2.1 (1.4) 2.0
(1.1) Duration of current MDE, weeks, mean (SD) 50.8 (28.3) 63.3 (106.9) Patient Disposition Completed double-blind part, n (%) 40 (100.0) 41 (100.0) Completed OLE part, n (%)a 63 (77.8) Mean (SD) Change from Baseline in MADRS
Anhedonia Factor Score BL D1 D2 D8 MCIC for MADRS anhedonia factor P<0.0001 P<0.0001 P<0.0001 Apparent sadness Reported sadness Concentration difficulty Lassitude Inability to feel Mean (SD) Change from Baseline in
MADRS Anhedonia Factor Items for OLE Completers at Month 6 GH001 (N=40) Placebo (N=41) GH001 (N=63)