Remission Rate (MADRS ≤10), % GH001 Day 8 Prior Treatment Failure Remission Rate
(MADRS ≤10), % GH001 EOT/Month 6 Prior Treatment Failure Remission Rate (MADRS ≤10), % STAR*D Reference Progressive Attenuation Results Table 1. Demographics and Baseline Characteristics Background Treatment-resistant depression (TRD)
is associated with persistent symptoms and significant unmet need for effective treatment1 Staging models for TRD have demonstrated that the number of prior treatment failures is among the strongest negative prognostic factors for subsequent
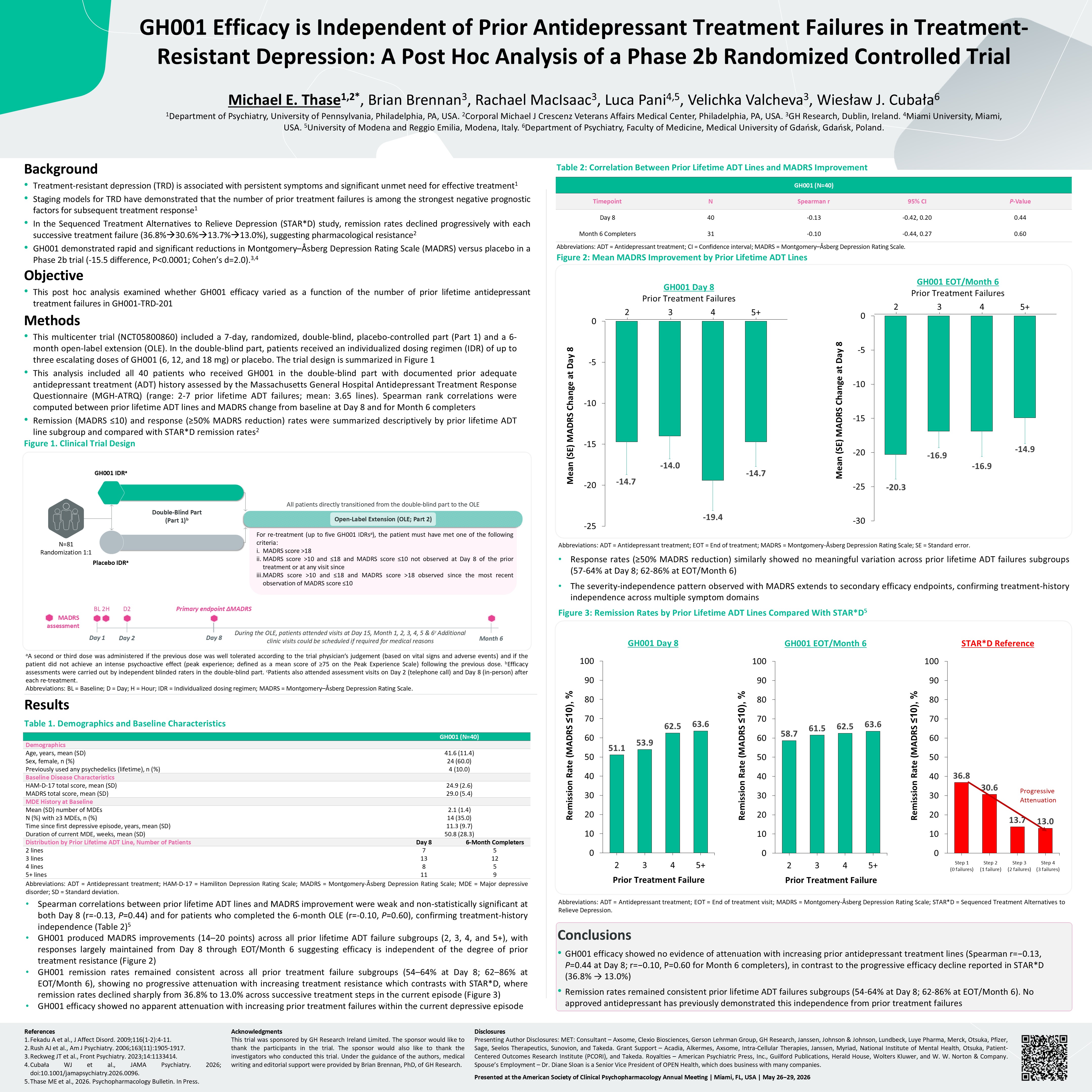
treatment response1 In the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, remission rates declined progressively with each successive treatment failure (36.8%30.6%13.7%13.0%), suggesting pharmacological
resistance2 GH001 demonstrated rapid and significant reductions in Montgomery–Åsberg Depression Rating Scale (MADRS) versus placebo in a Phase 2b trial (-15.5 difference, P<0.0001; Cohen’s d=2.0).3,4 Objective This post hoc analysis
examined whether GH001 efficacy varied as a function of the number of prior lifetime antidepressant treatment failures in GH001-TRD-201 Methods This multicenter trial (NCT05800860) included a 7-day, randomized, double-blind,
placebo-controlled part (Part 1) and a 6-month open-label extension (OLE). In the double-blind part, patients received an individualized dosing regimen (IDR) of up to three escalating doses of GH001 (6, 12, and 18 mg) or placebo. The trial
design is summarized in Figure 1 This analysis included all 40 patients who received GH001 in the double-blind part with documented prior adequate antidepressant treatment (ADT) history assessed by the Massachusetts General Hospital
Antidepressant Treatment Response Questionnaire (MGH-ATRQ) (range: 2-7 prior lifetime ADT failures; mean: 3.65 lines). Spearman rank correlations were computed between prior lifetime ADT lines and MADRS change from baseline at Day 8 and for
Month 6 completers Remission (MADRS ≤10) and response (≥50% MADRS reduction) rates were summarized descriptively by prior lifetime ADT line subgroup and compared with STAR*D remission rates2 Figure 1. Clinical Trial Design References Fekadu
A et al., J Affect Disord. 2009;116(1-2):4-11. Rush AJ et al., Am J Psychiatry. 2006;163(11):1905-1917. Reckweg JT et al., Front Psychiatry. 2023;14:1133414. Cubała WJ et al., JAMA Psychiatry. 2026;
doi:10.1001/jamapsychiatry.2026.0096. Thase ME et al., 2026. Psychopharmacology Bulletin. In Press. Acknowledgments This trial was sponsored by GH Research Ireland Limited. The sponsor would like to thank the participants in the trial. The
sponsor would also like to thank the investigators who conducted this trial. Under the guidance of the authors, medical writing and editorial support were provided by Brian Brennan, PhD, of GH Research. Disclosures Presenting Author
Disclosures: MET: Consultant – Axsome, Clexio Biosciences, Gerson Lehrman Group, GH Research, Janssen, Johnson & Johnson, Lundbeck, Luye Pharma, Merck, Otsuka, Pfizer, Sage, Seelos Therapeutics, Sunovion, and Takeda. Grant Support – Acadia,
Alkermes, Axsome, Intra-Cellular Therapies, Janssen, Myriad, National Institute of Mental Health, Otsuka, Patient-Centered Outcomes Research Institute (PCORI), and Takeda. Royalties – American Psychiatric Press, Inc., Guilford Publications,
Herald House, Wolters Kluwer, and W. W. Norton & Company. Spouse’s Employment – Dr. Diane Sloan is a Senior Vice President of OPEN Health, which does business with many companies. Presented at the American Society of Clinical
Psychopharmacology Annual Meeting | Miami, FL, USA | May 26−29, 2026 Conclusions GH001 efficacy showed no evidence of attenuation with increasing prior antidepressant treatment lines (Spearman r=−0.13, P=0.44 at Day 8; r=−0.10, P=0.60 for
Month 6 completers), in contrast to the progressive efficacy decline reported in STAR*D (36.8% → 13.0%) Remission rates remained consistent prior lifetime ADT failures subgroups (54-64% at Day 8; 62-86% at EOT/Month 6). No approved
antidepressant has previously demonstrated this independence from prior treatment failures Michael E. Thase1,2*, Brian Brennan3, Rachael MacIsaac3, Luca Pani4,5, Velichka Valcheva3, Wiesław J. Cubała6 1Department of Psychiatry, University of
Pennsylvania, Philadelphia, PA, USA. 2Corporal Michael J Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA. 3GH Research, Dublin, Ireland. 4Miami University, Miami, USA. 5University of Modena and Reggio Emilia, Modena, Italy.
6Department of Psychiatry, Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland. GH001 Efficacy is Independent of Prior Antidepressant Treatment Failures in Treatment-Resistant Depression: A Post Hoc Analysis of a Phase 2b
Randomized Controlled Trial aA second or third dose was administered if the previous dose was well tolerated according to the trial physician’s judgement (based on vital signs and adverse events) and if the patient did not achieve an intense
psychoactive effect (peak experience; defined as a mean score of ≥75 on the Peak Experience Scale) following the previous dose. bEfficacy assessments were carried out by independent blinded raters in the double-blind part. cPatients also
attended assessment visits on Day 2 (telephone call) and Day 8 (in-person) after each re-treatment. Abbreviations: BL = Baseline; D = Day; H = Hour; IDR = Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale.
Abbreviations: ADT = Antidepressant treatment; HAM-D-17 = Hamiliton Depression Rating Scale; MADRS = Montgomery-Åsberg Depression Rating Scale; MDE = Major depressive disorder; SD = Standard deviation. Spearman correlations between prior
lifetime ADT lines and MADRS improvement were weak and non-statistically significant at both Day 8 (r=-0.13, P=0.44) and for patients who completed the 6-month OLE (r=-0.10, P=0.60), confirming treatment-history independence (Table 2)5 GH001
produced MADRS improvements (14–20 points) across all prior lifetime ADT failure subgroups (2, 3, 4, and 5+), with responses largely maintained from Day 8 through EOT/Month 6 suggesting efficacy is independent of the degree of prior treatment
resistance (Figure 2) GH001 remission rates remained consistent across all prior treatment failure subgroups (54–64% at Day 8; 62–86% at EOT/Month 6), showing no progressive attenuation with increasing treatment resistance which contrasts with
STAR*D, where remission rates declined sharply from 36.8% to 13.0% across successive treatment steps in the current episode (Figure 3) GH001 efficacy showed no apparent attenuation with increasing prior treatment failures within the current
depressive episode Table 2: Correlation Between Prior Lifetime ADT Lines and MADRS Improvement Abbreviations: ADT = Antidepressant treatment; EOT = End of treatment; MADRS = Montgomery-Åsberg Depression Rating Scale; SE = Standard
error. Response rates (≥50% MADRS reduction) similarly showed no meaningful variation across prior lifetime ADT failures subgroups (57-64% at Day 8; 62-86% at EOT/Month 6) The severity-independence pattern observed with MADRS extends to
secondary efficacy endpoints, confirming treatment-history independence across multiple symptom domains Figure 3: Remission Rates by Prior Lifetime ADT Lines Compared With STAR*D5 Abbreviations: ADT = Antidepressant treatment; EOT = End of
treatment visit; MADRS = Montgomery-Åsberg Depression Rating Scale; STAR*D = Sequenced Treatment Alternatives to Relieve Depression. During the OLE, patients attended visits at Day 15, Month 1, 2, 3, 4, 5 & 6c Additional clinic visits
could be scheduled if required for medical reasons For re-treatment (up to five GH001 IDRsa), the patient must have met one of the following criteria: MADRS score >18 MADRS score >10 and ≤18 and MADRS score ≤10 not observed at Day 8
of the prior treatment or at any visit since MADRS score >10 and ≤18 and MADRS score >18 observed since the most recent observation of MADRS score ≤10 Open-Label Extension (OLE; Part 2) N=81 Randomization 1:1 Double-Blind Part (Part
1)b All patients directly transitioned from the double-blind part to the OLE Placebo IDRa GH001 IDRa BL 2H Day 1 Primary endpoint ΔMADRS Day 8 MADRS assessment Month 6 D2 Day 2 GH001 (N=40) Demographics Age, years, mean
(SD) 41.6 (11.4) Sex, female, n (%) 24 (60.0) Previously used any psychedelics (lifetime), n (%) 4 (10.0) Baseline Disease Characteristics HAM-D-17 total score, mean (SD) 24.9 (2.6) MADRS total score, mean (SD) 29.0 (5.4) MDE History
at Baseline Mean (SD) number of MDEs 2.1 (1.4) N (%) with ≥3 MDEs, n (%) 14 (35.0) Time since first depressive episode, years, mean (SD) 11.3 (9.7) Duration of current MDE, weeks, mean (SD) 50.8 (28.3) Distribution by Prior Lifetime
ADT Line, Number of Patients Day 8 6-Month Completers 2 lines 7 5 3 lines 13 12 4 lines 8 5 5+ lines 11 9 Mean (SE) MADRS Change at Day 8 GH001 Day 8 Prior Treatment Failures 2 3 4 5+ Mean (SE) MADRS Change at Day 8 GH001
EOT/Month 6 Prior Treatment Failures 2 3 4 5+ GH001 (N=40) Timepoint N Spearman r 95% CI P-Value Day 8 40 -0.13 -0.42, 0.20 0.44 Month 6 Completers 31 -0.10 -0.44, 0.27 0.60 Step 1 (0 failures) Step 2 (1 failure) Step
3 (2 failures) Step 4 (3 failures) Abbreviations: ADT = Antidepressant treatment; CI = Confidence interval; MADRS = Montgomery–Åsberg Depression Rating Scale. Figure 2: Mean MADRS Improvement by Prior Lifetime ADT Lines