| May 27, 2026 APEX Part B 16-week data |
| 2 © Apogee Therapeutics, Inc. Other than statements of historical facts, all statements included in this presentation are forward-looking statements, including statements about our plans for our current and future product candidates, programs, and clinical trials, including expansion of zumilokibart into additional indications, and announcement plans for APG273 and an additional pipeline program; the anticipated timing of initiation of our clinical trials, including the Phase 2b trial of zumilokibart in asthma, the Phase 2a trial of zumilokibart in eosinophilic esophagitis (EoE), and the Phase 3 ADventure program for zumilokibart in AD; the expected timing of results from our clinical trials, including the 52-week readout from Part B and the 2-year follow-up from Part A of our Phase 2 trial of zumilokibart in AD, 16-week readouts from the Phase 3 ADventure program, the data readouts for the Phase 2a ELEVATE program, and the Phase 1b readout for APG279 vs. DUPIXENT; the timing of other program catalysts; the expectation that the APEX Phase 2 Part B 16-week results will support commencement of a Phase 3 trial in zumilokibart; the potential for dose ranging trials in AD, asthma and EoE to enable a straight to Phase 3 approach; our planned clinical trial designs, including anticipated enrollment and dosing regimens; the potential clinical benefit, dosing regimen, safety and efficacy profiles and treatment outcomes of zumilokibart, including its potential to be a best-in-class therapy, new standard of care and biologic of choice in AD; the planned 2029 launch timeline for zumilokibart in AD; the pipeline-in-a-product potential for zumilokibart; our planned business strategies; expected timing for future pipeline updates, regulatory decisions, the BLA filing for zumilokibart in AD, and potential commercialization; our expectations regarding the time period over which our capital resources will be sufficient to fund our anticipated operations; our future funding needs, which do not include the need for equity financing; and estimates of market size. In some cases, you can identify forward-looking statements by terms such as “anticipate,” “believe,” “can,” “could,” “design,” “estimate,” “expect,” “intend,” “likely,” “may,” “might,” “plan,” “potential,” “predict,” “suggest,” “target,” “will,” “would,” or the negative of these terms, and similar expressions intended to identify forward-looking statements. The forward-looking statements are based on our beliefs, assumptions and expectations of future performance, taking into account the information currently available to us. These statements are only predictions based upon our current expectations and projections about future events. The data included in this presentation may be subject to change following the availability of additional data or following a more comprehensive review of the data. Forward-looking statements are subject to known and unknown risks, uncertainties and other factors that may cause our actual results, level of activity, performance or achievements to be materially different from those expressed or implied by such forward-looking statements, including those risks described in “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in our Annual Report on Form 10-K for the year ended December 31, 2025, filed with the U.S. Securities and Exchange Commission (the SEC) on March 2, 2026 and subsequent disclosure documents we have filed and may file with the SEC. Although we have attempted to identify important factors that could cause actual results to differ materially from those contained in forward-looking statements, there may be other factors that cause results not to be as anticipated, estimated or intended. We claim the protection of the Safe Harbor contained in the Private Securities Litigation Reform Act of 1995 for forward-looking statements. This presentation concerns drug candidates that are under clinical investigation, and which have not yet been approved by the U.S. Food and Drug Administration. These are currently limited by federal law to investigational use, and no representation is made as to their safety or effectiveness for the purposes for which they are being investigated. The assumptions used in the preparation of this presentation, although considered reasonable by us at the time of preparation, may prove to be incorrect. You are cautioned that the information is based on assumptions as to many factors and that actual results may vary from the results projected and such variations may be material. Accordingly, you should not place undue reliance on any forward-looking statements contained herein or rely on them as predictions of future events. All forward-looking statements in this presentation apply only as of the date made and are expressly qualified by the cautionary statements included in this presentation. We do not undertake to update any forward-looking statements, except in accordance with applicable securities laws. This presentation also uses estimates and other statistical data made by independent parties and us relating to the data and analysis about our industry. The data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. The trademarks, trade names and service marks appearing in this presentation are the property of their respective owners. Certain information contained in this presentation relate to or are based on studies, publications and other data obtained from third-party sources as well as our own internal estimates and research. While we believe these third-party sources to be reliable as of the date of this presentation, we have not independently verified, and make no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. This presentation contains data based on cross-study comparisons and not based on any head-to-head clinical trials. Cross-study comparisons are inherently limited and may suggest misleading similarities and differences. The values shown in the cross-study comparisons are directional and may not be directly comparable. Disclaimers and Forward-looking statements |
| 3 © Apogee Therapeutics, Inc. Agenda Introduction Michael Henderson, MD Chief Executive Officer Carl Dambkowski, MD Chief Medical Officer Kristine Nograles, MD, SVP, Head of Clinical Development & Medical Affairs, Dermatology Amol Kamboj, MD, SVP, Head of Clinical Development, Respiratory & GI APEX Phase 2 Part B 16-Week Results Zumilokibart Development Program Building a Leading I&I Company Analyst Q&A Michael Henderson, MD Chief Executive Officer Michael Henderson, MD, CEO Carl Dambkowski, MD, CMO Jane Pritchett Henderson, CFO Jeff Hartness, CCO Invited KOL: Ruth Ann Vleugels, MD, MPH, MBA Treatment Gaps in Atopic Dermatitis Invited KOL: Ruth Ann Vleugels, MD, MPH, MBA Mass General Brigham, Harvard Medical School |

| Introduction Michael Henderson, MD Chief Executive Officer |
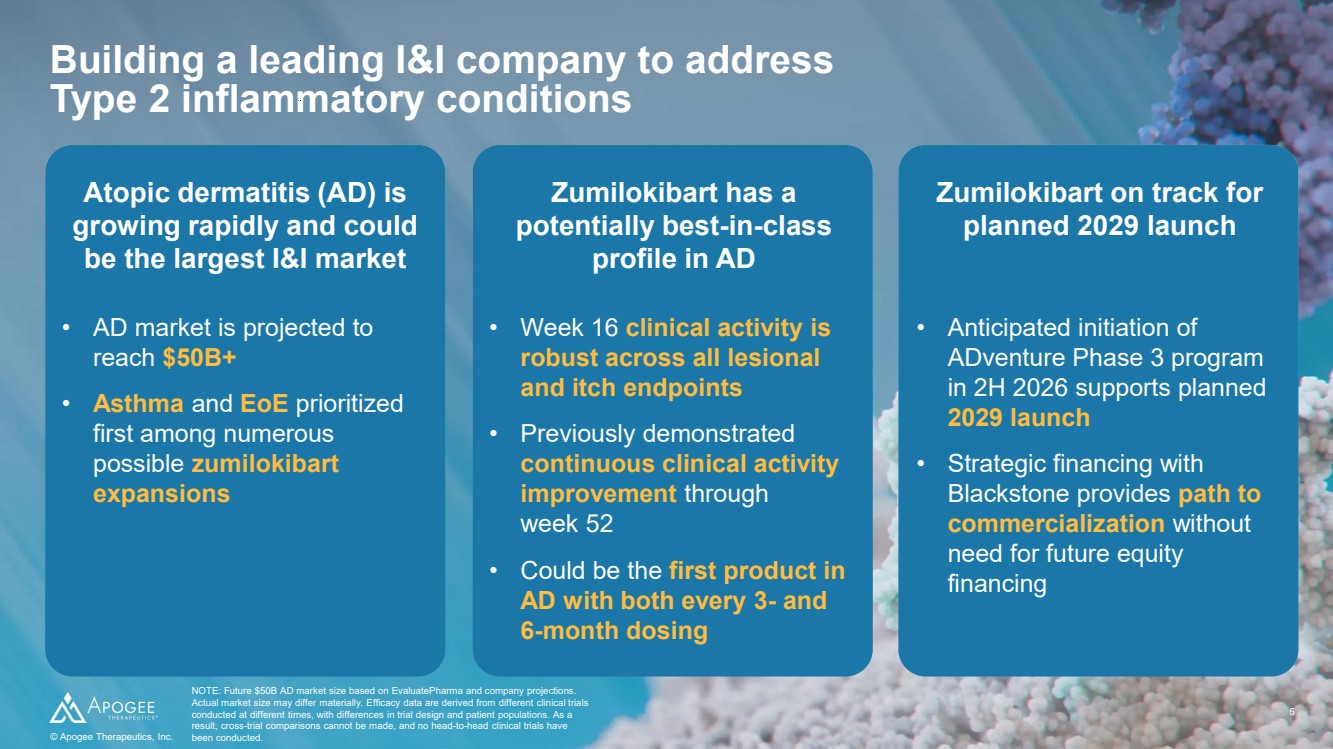
| 5 © Apogee Therapeutics, Inc. Building a leading I&I company to address Type 2 inflammatory conditions NOTE: Future $50B AD market size based on EvaluatePharma and company projections. Actual market size may differ materially. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Zumilokibart has a potentially best-in-class profile in AD Zumilokibart on track for planned 2029 launch Atopic dermatitis (AD) is growing rapidly and could be the largest I&I market • AD market is projected to reach $50B+ • Asthma and EoE prioritized first among numerous possible zumilokibart expansions © Apogee Therapeutics, Inc. • Week 16 clinical activity is robust across all lesional and itch endpoints • Previously demonstrated continuous clinical activity improvement through week 52 • Could be the first product in AD with both every 3- and 6-month dosing • Anticipated initiation of ADventure Phase 3 program in 2H 2026 supports planned 2029 launch • Strategic financing with Blackstone provides path to commercialization without need for future equity financing |
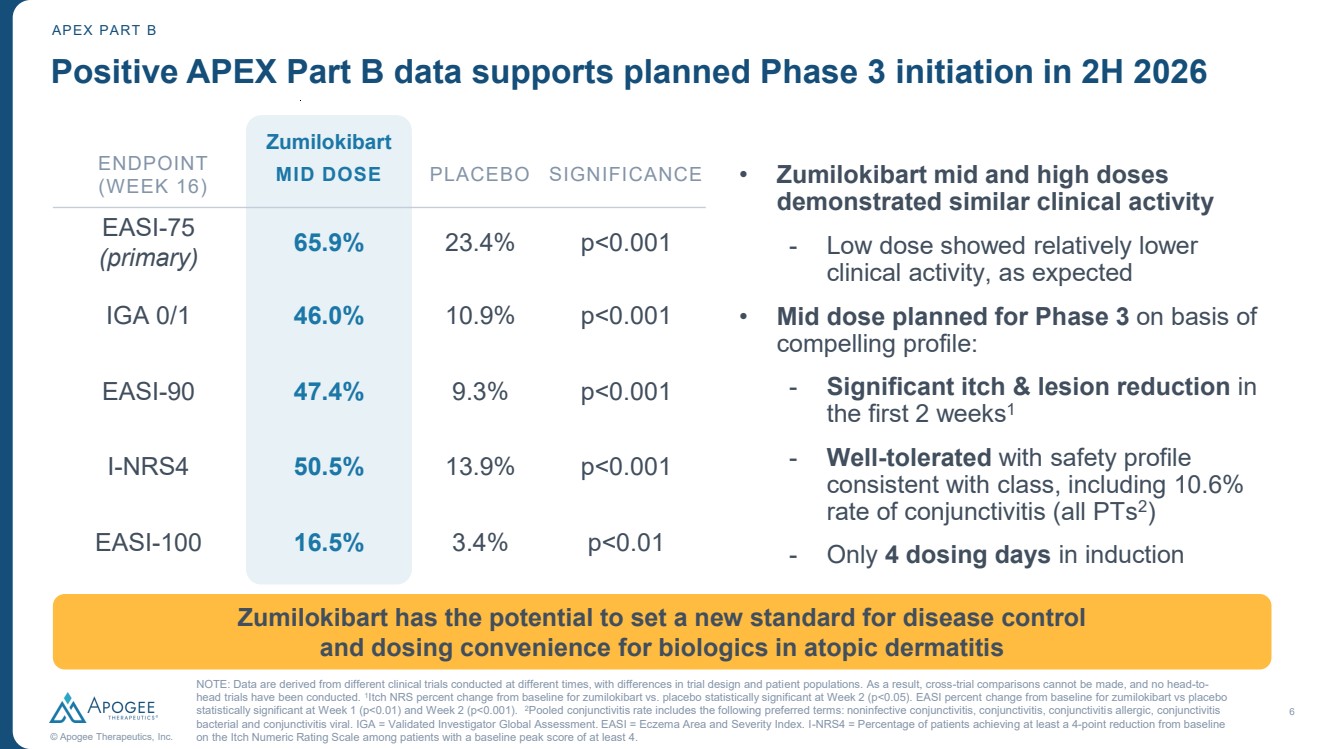
| 6 © Apogee Therapeutics, Inc. APEX PART B ENDPOINT (WEEK 16) MID DOSE PLACEBO SIGNIFICANCE EASI-75 (primary) 65.9% 23.4% p<0.001 IGA 0/1 46.0% 10.9% p<0.001 EASI-90 47.4% 9.3% p<0.001 I-NRS4 50.5% 13.9% p<0.001 EASI-100 16.5% 3.4% p<0.01 Positive APEX Part B data supports planned Phase 3 initiation in 2H 2026 Zumilokibart • Zumilokibart mid and high doses demonstrated similar clinical activity - Low dose showed relatively lower clinical activity, as expected • Mid dose planned for Phase 3 on basis of compelling profile: - Significant itch & lesion reduction in the first 2 weeks1 - Well-tolerated with safety profile consistent with class, including 10.6% rate of conjunctivitis (all PTs2 ) - Only 4 dosing days in induction NOTE: Data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head trials have been conducted. 1 Itch NRS percent change from baseline for zumilokibart vs. placebo statistically significant at Week 2 (p<0.05). EASI percent change from baseline for zumilokibart vs placebo statistically significant at Week 1 (p<0.01) and Week 2 (p<0.001). 2Pooled conjunctivitis rate includes the following preferred terms: noninfective conjunctivitis, conjunctivitis, conjunctivitis allergic, conjunctivitis bacterial and conjunctivitis viral. IGA = Validated Investigator Global Assessment. EASI = Eczema Area and Severity Index. I-NRS4 = Percentage of patients achieving at least a 4-point reduction from baseline on the Itch Numeric Rating Scale among patients with a baseline peak score of at least 4. Zumilokibart has the potential to set a new standard for disease control and dosing convenience for biologics in atopic dermatitis |
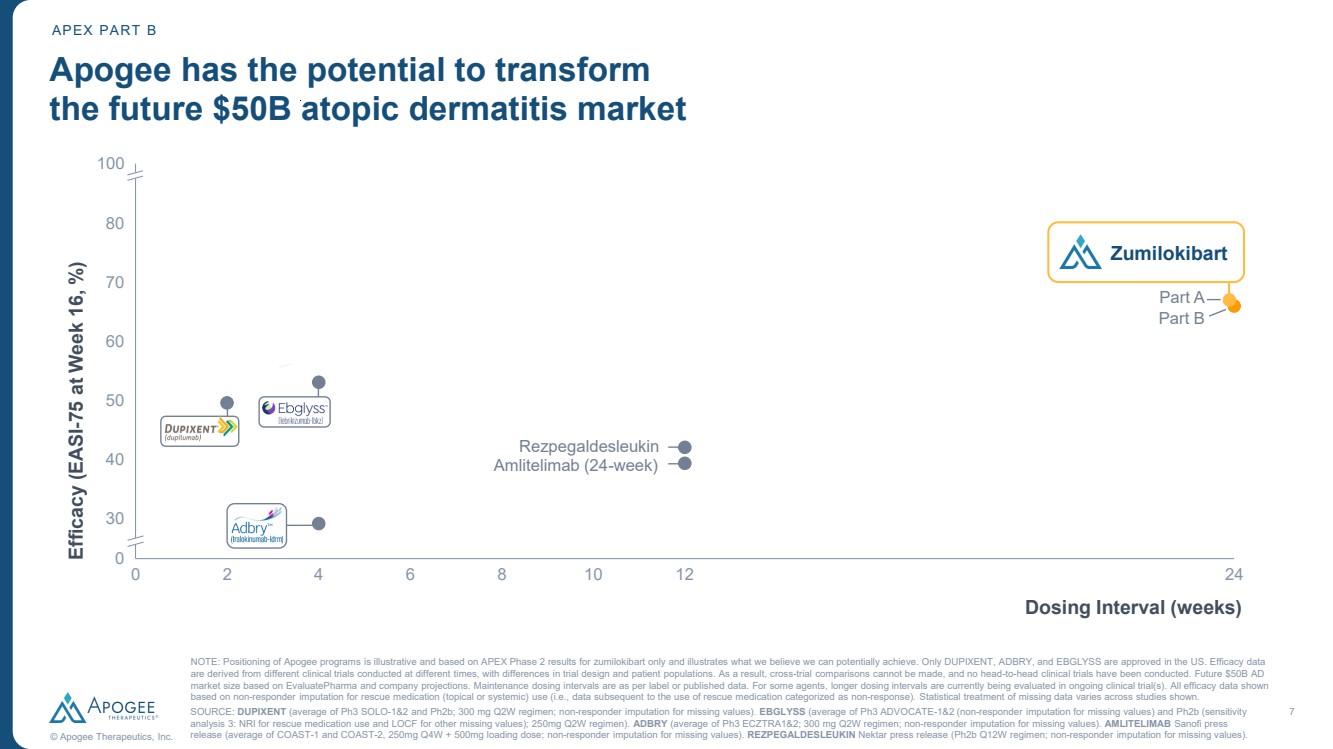
| 7 © Apogee Therapeutics, Inc. APEX PART B 0 2 4 6 8 10 12 24 0 30 40 50 60 70 80 90 Amlitelimab (24-week) Part B Part A Apogee has the potential to transform the future $50B atopic dermatitis market Efficacy (EASI-75 at Week 16, %) NOTE: Positioning of Apogee programs is illustrative and based on APEX Phase 2 results for zumilokibart only and illustrates what we believe we can potentially achieve. Only DUPIXENT, ADBRY, and EBGLYSS are approved in the US. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Future $50B AD market size based on EvaluatePharma and company projections. Maintenance dosing intervals are as per label or published data. For some agents, longer dosing intervals are currently being evaluated in ongoing clinical trial(s). All efficacy data shown based on non-responder imputation for rescue medication (topical or systemic) use (i.e., data subsequent to the use of rescue medication categorized as non-response). Statistical treatment of missing data varies across studies shown. SOURCE: DUPIXENT (average of Ph3 SOLO-1&2 and Ph2b; 300 mg Q2W regimen; non-responder imputation for missing values). EBGLYSS (average of Ph3 ADVOCATE-1&2 (non-responder imputation for missing values) and Ph2b (sensitivity analysis 3: NRI for rescue medication use and LOCF for other missing values); 250mg Q2W regimen). ADBRY (average of Ph3 ECZTRA1&2; 300 mg Q2W regimen; non-responder imputation for missing values). AMLITELIMAB Sanofi press release (average of COAST-1 and COAST-2, 250mg Q4W + 500mg loading dose; non-responder imputation for missing values). REZPEGALDESLEUKIN Nektar press release (Ph2b Q12W regimen; non-responder imputation for missing values). 100 Zumilokibart Dosing Interval (weeks) Rezpegaldesleukin |
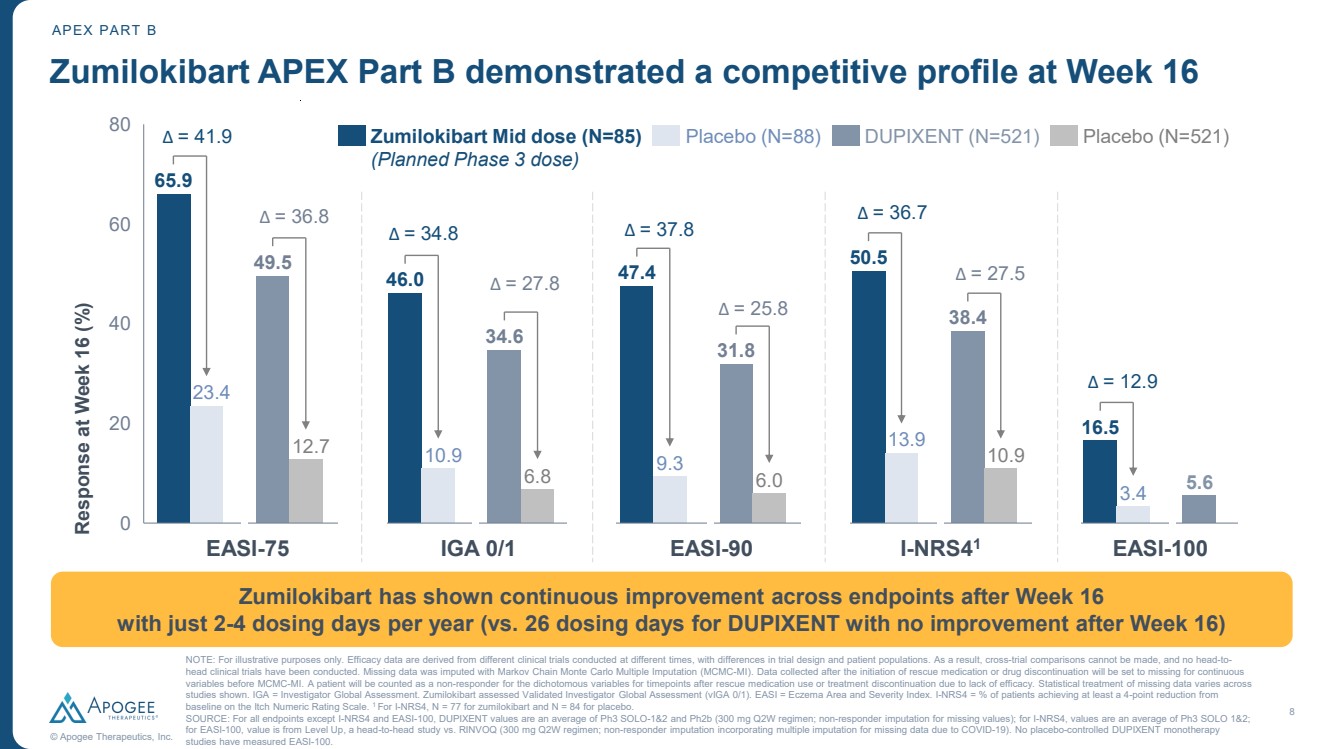
| 8 © Apogee Therapeutics, Inc. 65.9 23.4 49.5 12.7 46.0 10.9 34.6 6.8 47.4 9.3 31.8 6.0 50.5 13.9 38.4 10.9 16.5 3.4 5.6 20 40 60 80 Response at Week 16 (%) 0 Zumilokibart APEX Part B demonstrated a competitive profile at Week 16 Zumilokibart Mid dose (N=85) (Planned Phase 3 dose) Placebo (N=88) DUPIXENT (N=521) Placebo (N=521) EASI-75 IGA 0/1 EASI-90 NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Missing data was imputed with Markov Chain Monte Carlo Multiple Imputation (MCMC-MI). Data collected after the initiation of rescue medication or drug discontinuation will be set to missing for continuous variables before MCMC-MI. A patient will be counted as a non-responder for the dichotomous variables for timepoints after rescue medication use or treatment discontinuation due to lack of efficacy. Statistical treatment of missing data varies across studies shown. IGA = Investigator Global Assessment. Zumilokibart assessed Validated Investigator Global Assessment (vIGA 0/1). EASI = Eczema Area and Severity Index. I-NRS4 = % of patients achieving at least a 4-point reduction from baseline on the Itch Numeric Rating Scale. 1 For I-NRS4, N = 77 for zumilokibart and N = 84 for placebo. SOURCE: For all endpoints except I-NRS4 and EASI-100, DUPIXENT values are an average of Ph3 SOLO-1&2 and Ph2b (300 mg Q2W regimen; non-responder imputation for missing values); for I-NRS4, values are an average of Ph3 SOLO 1&2; for EASI-100, value is from Level Up, a head-to-head study vs. RINVOQ (300 mg Q2W regimen; non-responder imputation incorporating multiple imputation for missing data due to COVID-19). No placebo-controlled DUPIXENT monotherapy studies have measured EASI-100. Δ = 41.9 Δ = 34.8 Δ = 37.8 Δ = 36.8 Δ = 25.8 Δ = 27.8 Zumilokibart has shown continuous improvement across endpoints after Week 16 with just 2-4 dosing days per year (vs. 26 dosing days for DUPIXENT with no improvement after Week 16) Δ = 36.7 Δ = 27.5 I-NRS41 Δ = 12.9 EASI-100 APEX PART B |
| APEX Phase 2 Part B 16-week Results Carl Dambkowski, MD Chief Medical Officer |
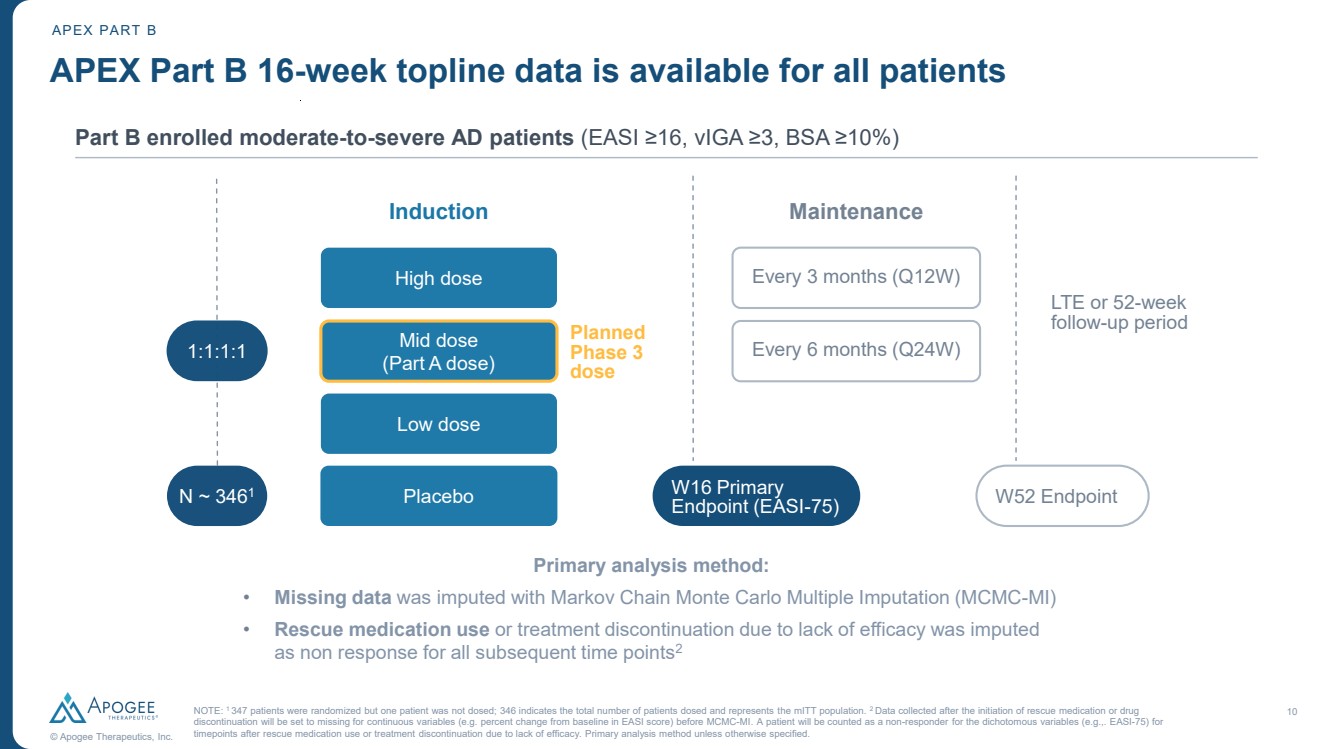
| 10 © Apogee Therapeutics, Inc. APEX Part B 16-week topline data is available for all patients Part B enrolled moderate-to-severe AD patients (EASI ≥16, vIGA ≥3, BSA ≥10%) APEX PART B Primary analysis method: • Missing data was imputed with Markov Chain Monte Carlo Multiple Imputation (MCMC-MI) • Rescue medication use or treatment discontinuation due to lack of efficacy was imputed as non response for all subsequent time points2 Every 3 months (Q12W) Every 6 months (Q24W) Maintenance LTE or 52-week follow-up period W16 Primary Endpoint (EASI-75) W52 Endpoint 1:1:1:1 Induction High dose Mid dose (Part A dose) Low dose N ~ 346 Placebo 1 Planned Phase 3 dose NOTE: 1 347 patients were randomized but one patient was not dosed; 346 indicates the total number of patients dosed and represents the mITT population. 2 Data collected after the initiation of rescue medication or drug discontinuation will be set to missing for continuous variables (e.g. percent change from baseline in EASI score) before MCMC-MI. A patient will be counted as a non-responder for the dichotomous variables (e.g.,. EASI-75) for timepoints after rescue medication use or treatment discontinuation due to lack of efficacy. Primary analysis method unless otherwise specified. |
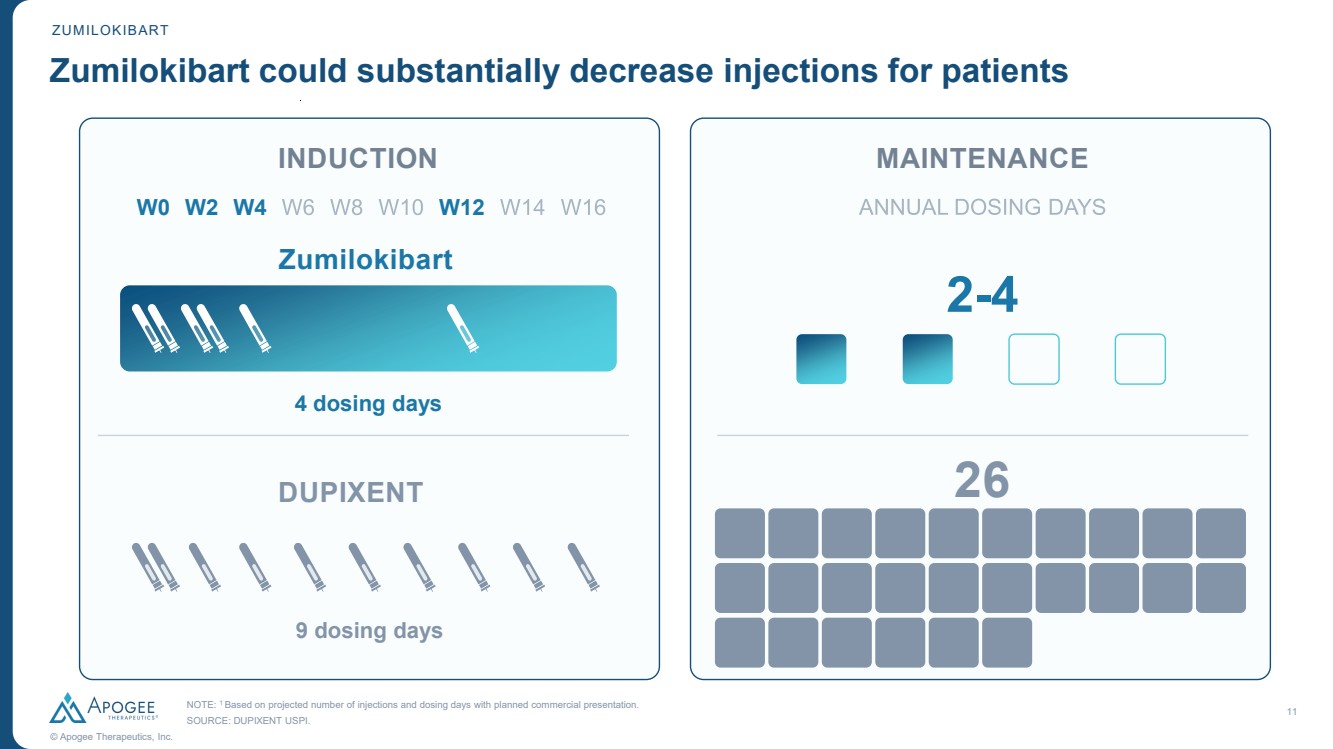
| 11 © Apogee Therapeutics, Inc. NOTE: 1 Based on projected number of injections and dosing days with planned commercial presentation. SOURCE: DUPIXENT USPI. Zumilokibart could substantially decrease injections for patients ZUMILOKIBART DUPIXENT 9 dosing days INDUCTION MAINTENANCE W0 W2 W4 W12 Zumilokibart 4 dosing days 2-4 26 |
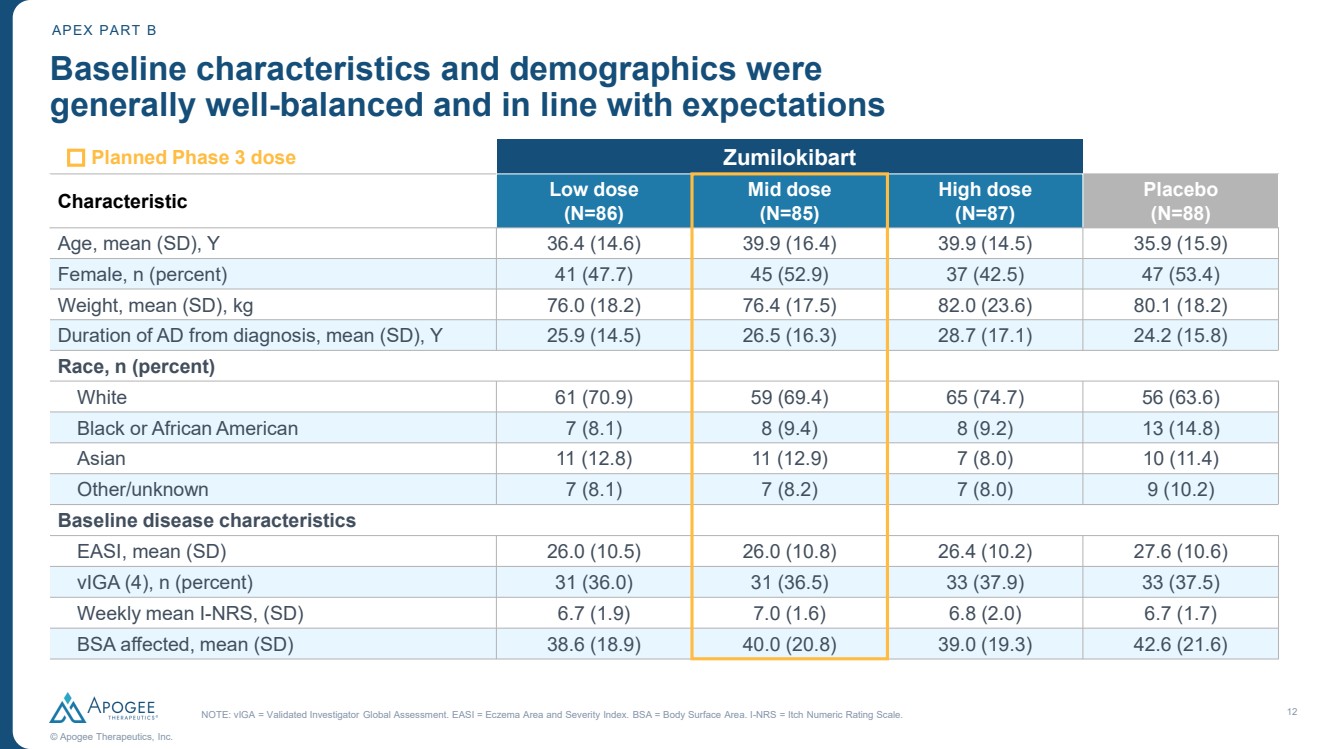
| 12 © Apogee Therapeutics, Inc. Baseline characteristics and demographics were generally well-balanced and in line with expectations APEX PART B Zumilokibart NOTE: vIGA = Validated Investigator Global Assessment. EASI = Eczema Area and Severity Index. BSA = Body Surface Area. I-NRS = Itch Numeric Rating Scale. Planned Phase 3 dose Characteristic Low dose (N=86) Mid dose (N=85) High dose (N=87) Placebo (N=88) Age, mean (SD), Y 36.4 (14.6) 39.9 (16.4) 39.9 (14.5) 35.9 (15.9) Female, n (percent) 41 (47.7) 45 (52.9) 37 (42.5) 47 (53.4) Weight, mean (SD), kg 76.0 (18.2) 76.4 (17.5) 82.0 (23.6) 80.1 (18.2) Duration of AD from diagnosis, mean (SD), Y 25.9 (14.5) 26.5 (16.3) 28.7 (17.1) 24.2 (15.8) Race, n (percent) White 61 (70.9) 59 (69.4) 65 (74.7) 56 (63.6) Black or African American 7 (8.1) 8 (9.4) 8 (9.2) 13 (14.8) Asian 11 (12.8) 11 (12.9) 7 (8.0) 10 (11.4) Other/unknown 7 (8.1) 7 (8.2) 7 (8.0) 9 (10.2) Baseline disease characteristics EASI, mean (SD) 26.0 (10.5) 26.0 (10.8) 26.4 (10.2) 27.6 (10.6) vIGA (4), n (percent) 31 (36.0) 31 (36.5) 33 (37.9) 33 (37.5) Weekly mean I-NRS, (SD) 6.7 (1.9) 7.0 (1.6) 6.8 (2.0) 6.7 (1.7) BSA affected, mean (SD) 38.6 (18.9) 40.0 (20.8) 39.0 (19.3) 42.6 (21.6) |
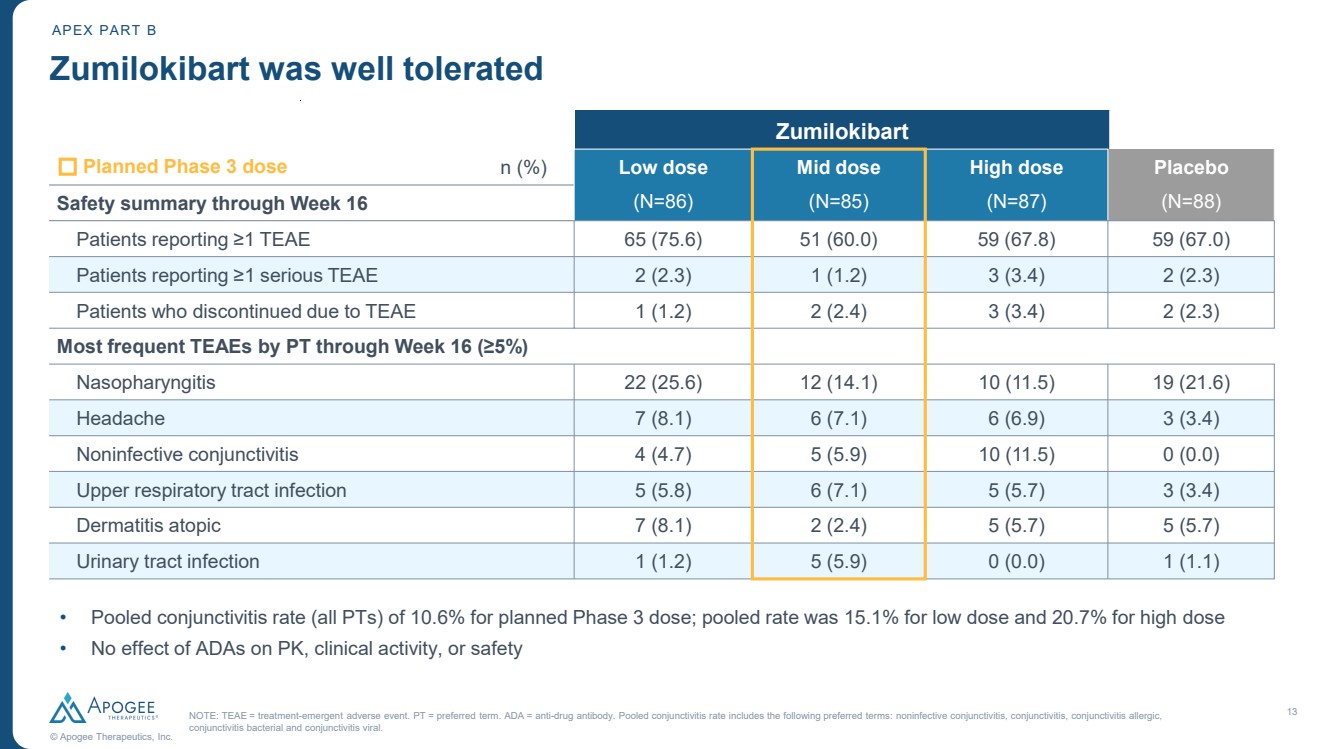
| 13 © Apogee Therapeutics, Inc. Zumilokibart was well tolerated Zumilokibart NOTE: TEAE = treatment-emergent adverse event. PT = preferred term. ADA = anti-drug antibody. Pooled conjunctivitis rate includes the following preferred terms: noninfective conjunctivitis, conjunctivitis, conjunctivitis allergic, conjunctivitis bacterial and conjunctivitis viral. APEX PART B • Pooled conjunctivitis rate (all PTs) of 10.6% for planned Phase 3 dose; pooled rate was 15.1% for low dose and 20.7% for high dose • No effect of ADAs on PK, clinical activity, or safety Planned Phase 3 dose n (%) Low dose Mid dose High dose Placebo Safety summary through Week 16 (N=86) (N=85) (N=87) (N=88) Patients reporting ≥1 TEAE 65 (75.6) 51 (60.0) 59 (67.8) 59 (67.0) Patients reporting ≥1 serious TEAE 2 (2.3) 1 (1.2) 3 (3.4) 2 (2.3) Patients who discontinued due to TEAE 1 (1.2) 2 (2.4) 3 (3.4) 2 (2.3) Most frequent TEAEs by PT through Week 16 (≥5%) Nasopharyngitis 22 (25.6) 12 (14.1) 10 (11.5) 19 (21.6) Headache 7 (8.1) 6 (7.1) 6 (6.9) 3 (3.4) Noninfective conjunctivitis 4 (4.7) 5 (5.9) 10 (11.5) 0 (0.0) Upper respiratory tract infection 5 (5.8) 6 (7.1) 5 (5.7) 3 (3.4) Dermatitis atopic 7 (8.1) 2 (2.4) 5 (5.7) 5 (5.7) Urinary tract infection 1 (1.2) 5 (5.9) 0 (0.0) 1 (1.1) |
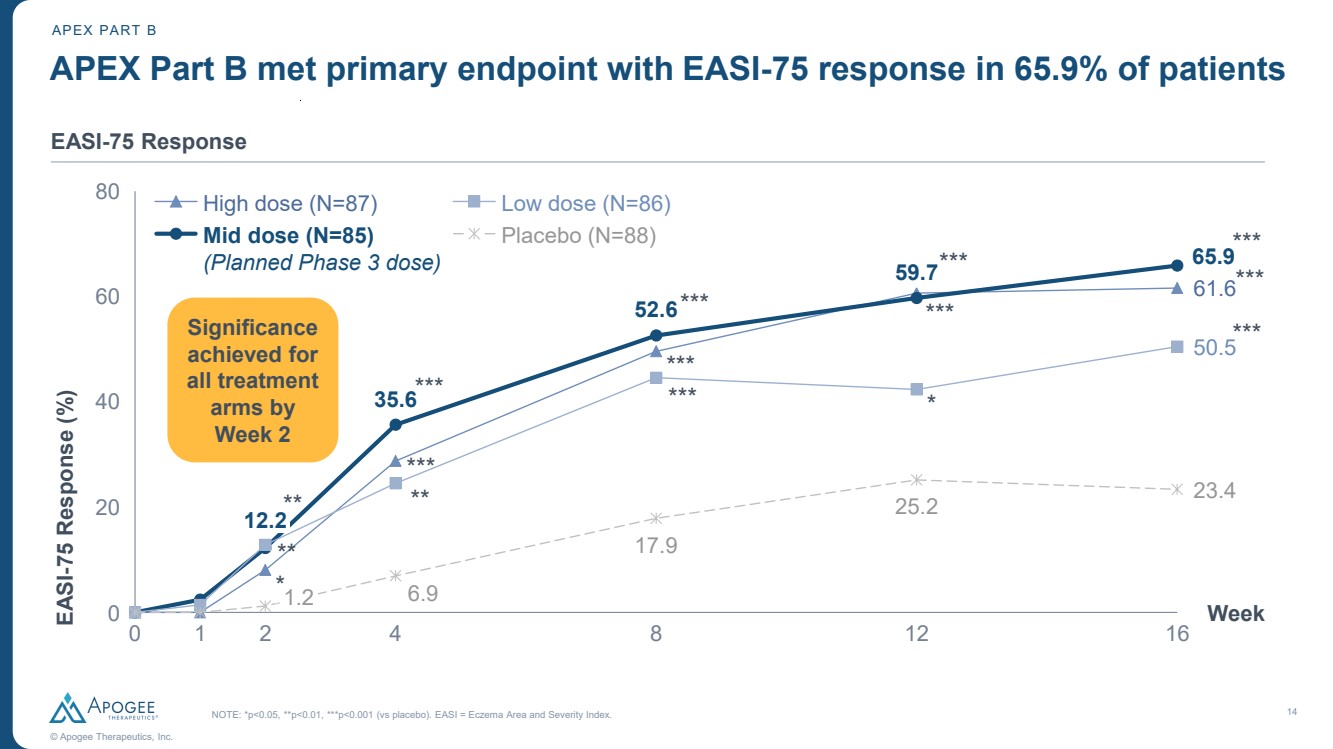
| 14 © Apogee Therapeutics, Inc. APEX PART B EASI-75 Response 61.6 35.6 52.6 59.7 65.9 50.5 6.9 17.9 25.2 23.4 0 1 2 4 8 12 16 0 20 40 60 80 EASI Week -75 Response (%) 12.2 1.2 High dose (N=87) Mid dose (N=85) (Planned Phase 3 dose) Low dose (N=86) Placebo (N=88) APEX Part B met primary endpoint with EASI-75 response in 65.9% of patients NOTE: *p<0.05, **p<0.01, ***p<0.001 (vs placebo). EASI = Eczema Area and Severity Index. Significance achieved for all treatment arms by Week 2 ** ** *** *** *** *** *** *** *** * *** *** ** * *** |
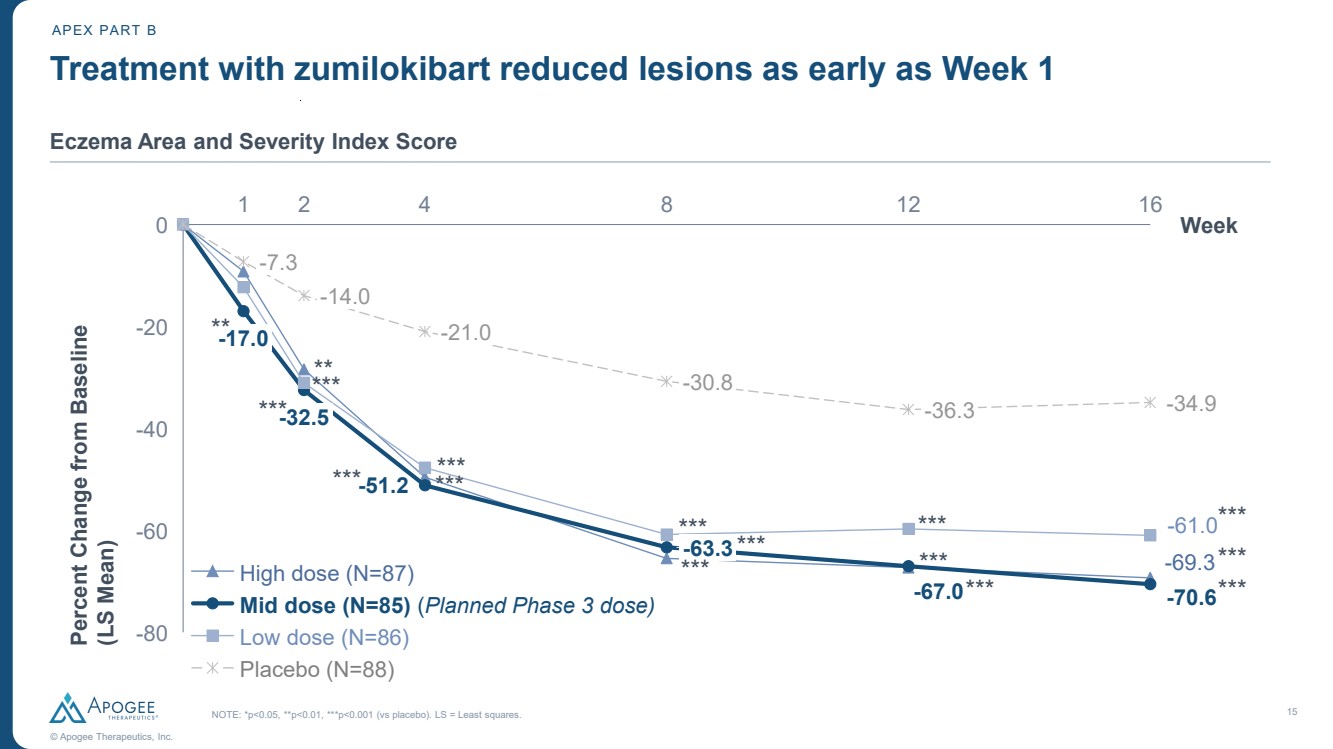
| 15 © Apogee Therapeutics, Inc. Treatment with zumilokibart reduced lesions as early as Week 1 -69.3 -51.2 -67.0 -70.6 -61.0 -34.9 1 2 4 8 12 16 -80 -60 -40 -20 0 Week Percent Change from Baseline (LS Mean) -17.0 -7.3 -32.5 -14.0 -21.0 -63.3 -30.8 -36.3 High dose (N=87) Mid dose (N=85) (Planned Phase 3 dose) Low dose (N=86) Placebo (N=88) APEX PART B Eczema Area and Severity Index Score ** *** *** ** *** *** *** *** *** *** *** *** *** *** *** *** NOTE: *p<0.05, **p<0.01, ***p<0.001 (vs placebo). LS = Least squares. |
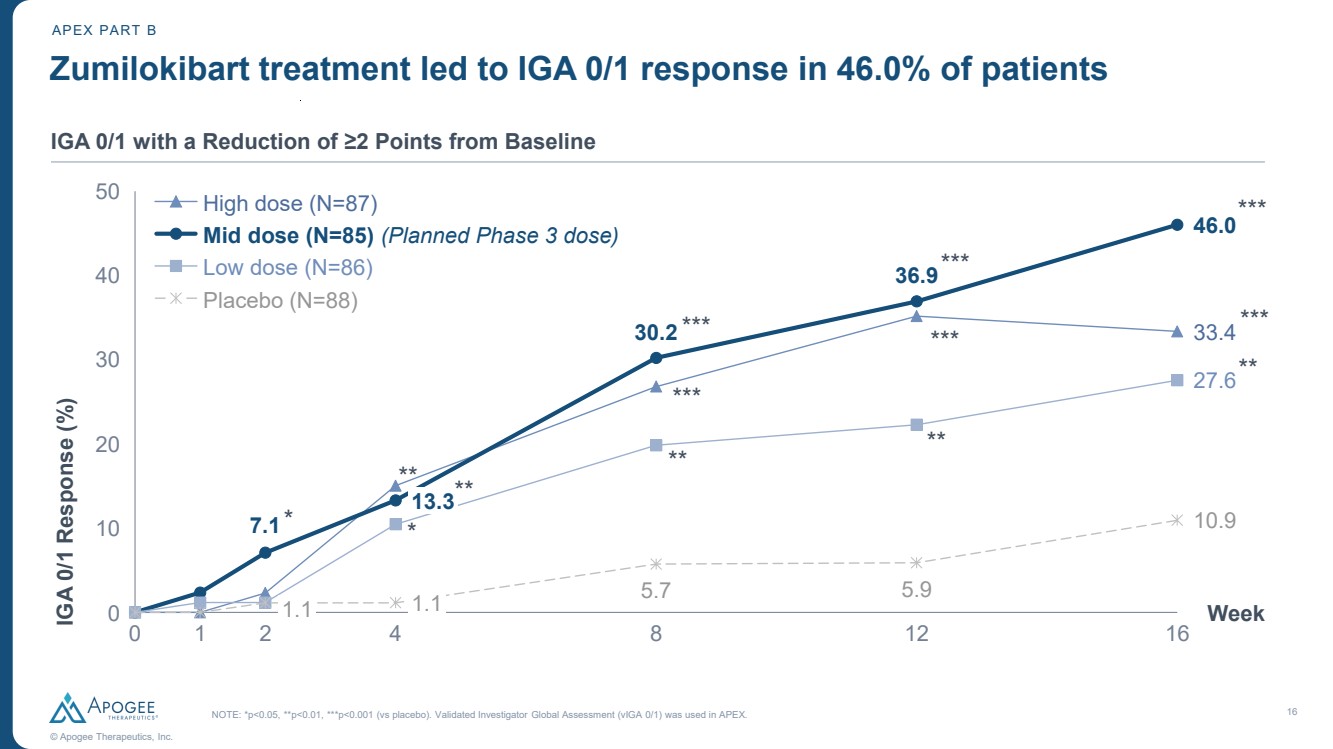
| 16 © Apogee Therapeutics, Inc. APEX PART B IGA 0/1 with a Reduction of ≥2 Points from Baseline 33.4 7.1 30.2 36.9 46.0 27.6 5.7 5.9 10.9 0 1 2 4 8 12 16 0 10 20 30 40 50 IGA 0/1 Response (%) 1.1 Week 13.3 1.1 High dose (N=87) Mid dose (N=85) (Planned Phase 3 dose) Low dose (N=86) Placebo (N=88) Zumilokibart treatment led to IGA 0/1 response in 46.0% of patients NOTE: *p<0.05, **p<0.01, ***p<0.001 (vs placebo). Validated Investigator Global Assessment (vIGA 0/1) was used in APEX. * * ** ** ** *** *** ** *** *** ** *** *** |
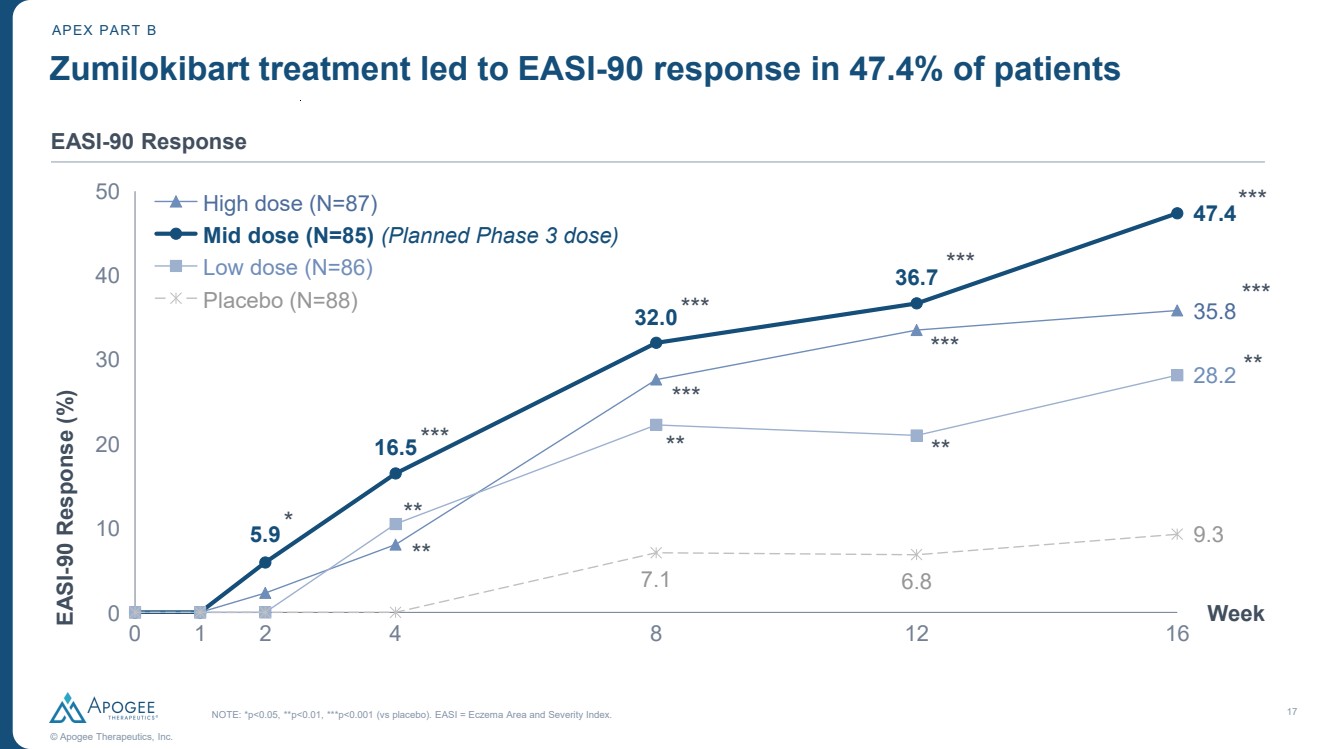
| 17 © Apogee Therapeutics, Inc. APEX PART B EASI-90 Response 35.8 5.9 16.5 32.0 36.7 47.4 28.2 7.1 6.8 9.3 0 1 2 4 8 12 16 0 10 20 30 40 50 EASI Week -90 Response (%) High dose (N=87) Mid dose (N=85) (Planned Phase 3 dose) Low dose (N=86) Placebo (N=88) Zumilokibart treatment led to EASI-90 response in 47.4% of patients NOTE: *p<0.05, **p<0.01, ***p<0.001 (vs placebo). EASI = Eczema Area and Severity Index. * ** ** *** ** *** *** ** *** *** ** *** *** |
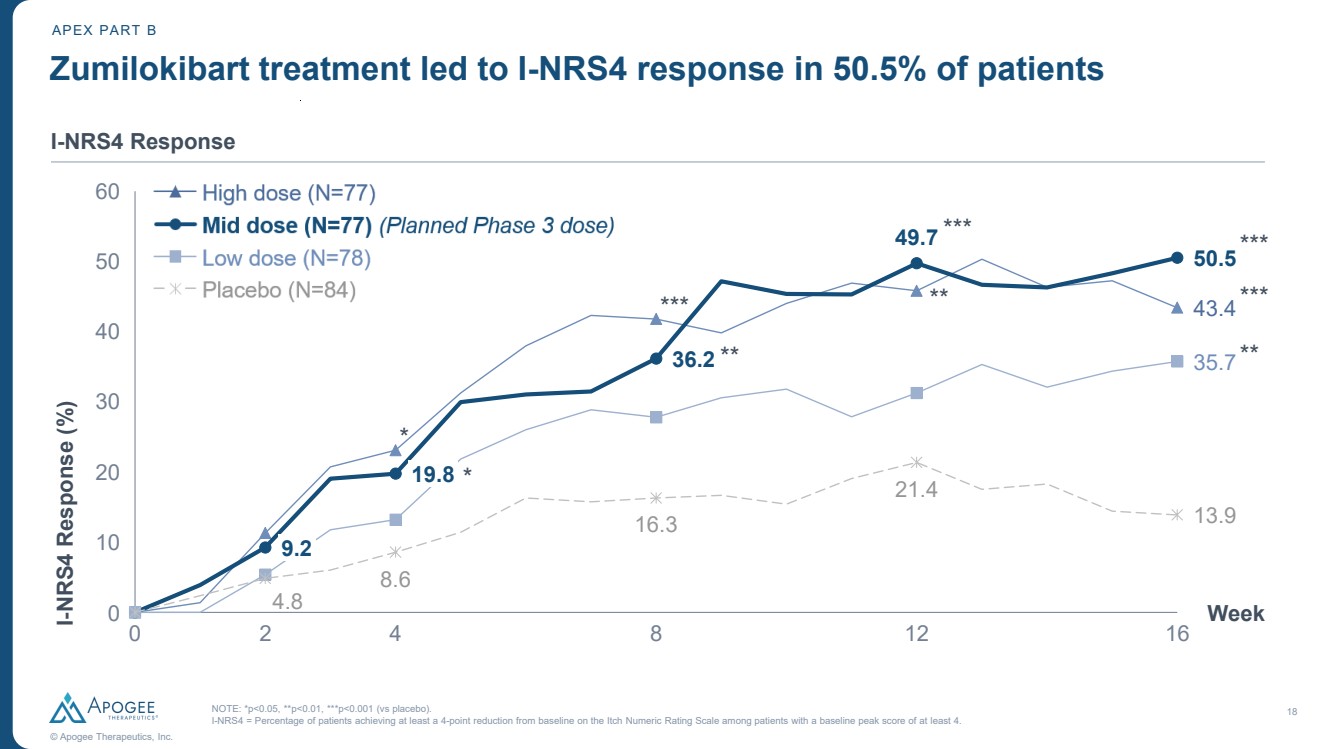
| 18 © Apogee Therapeutics, Inc. APEX PART B I-NRS4 Response 43.4 36.2 49.7 50.5 35.7 4.8 8.6 16.3 21.4 13.9 0 2 4 8 12 16 0 10 20 30 40 50 60 I-Week NRS4 Response (%) 9.2 19.8 Zumilokibart treatment led to I-NRS4 response in 50.5% of patients NOTE: *p<0.05, **p<0.01, ***p<0.001 (vs placebo). I-NRS4 = Percentage of patients achieving at least a 4-point reduction from baseline on the Itch Numeric Rating Scale among patients with a baseline peak score of at least 4. * * ** *** ** *** *** *** ** |
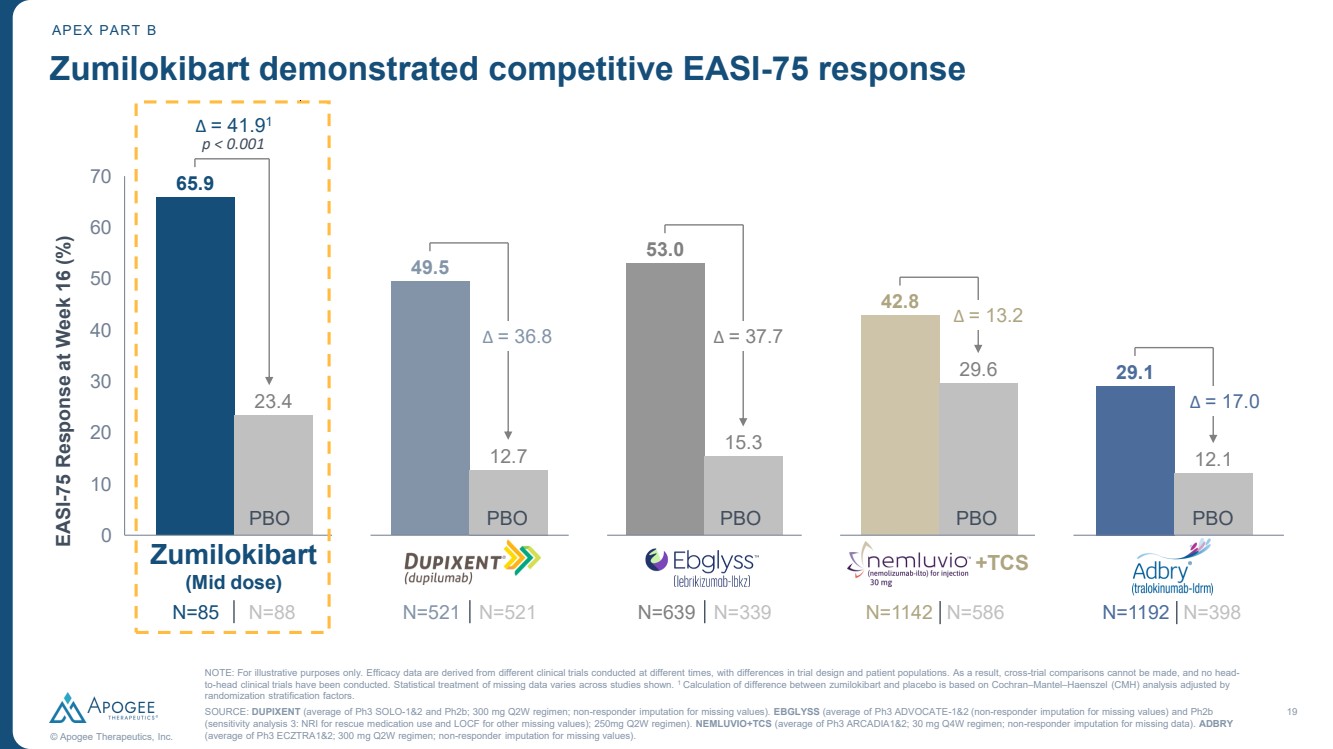
| 19 © Apogee Therapeutics, Inc. 65.9 23.4 49.5 12.7 53.0 15.3 42.8 29.6 29.1 12.1 0 20 40 60 10 30 50 70 EASI-75 Response at Week 16 (%) N=85 N=88 N=521 N=521 N=639 N=339 N=1142 N=586 Zumilokibart demonstrated competitive EASI-75 response APEX PART B Δ = 41.91 p < 0.001 Δ = 36.8 Δ = 37.7 PBO PBO PBO PBO PBO Zumilokibart (Mid dose) +TCS N=1192 N=398 Δ = 13.2 Δ = 17.0 NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Statistical treatment of missing data varies across studies shown. 1 Calculation of difference between zumilokibart and placebo is based on Cochran–Mantel–Haenszel (CMH) analysis adjusted by randomization stratification factors. SOURCE: DUPIXENT (average of Ph3 SOLO-1&2 and Ph2b; 300 mg Q2W regimen; non-responder imputation for missing values). EBGLYSS (average of Ph3 ADVOCATE-1&2 (non-responder imputation for missing values) and Ph2b (sensitivity analysis 3: NRI for rescue medication use and LOCF for other missing values); 250mg Q2W regimen). NEMLUVIO+TCS (average of Ph3 ARCADIA1&2; 30 mg Q4W regimen; non-responder imputation for missing data). ADBRY (average of Ph3 ECZTRA1&2; 300 mg Q2W regimen; non-responder imputation for missing values). |
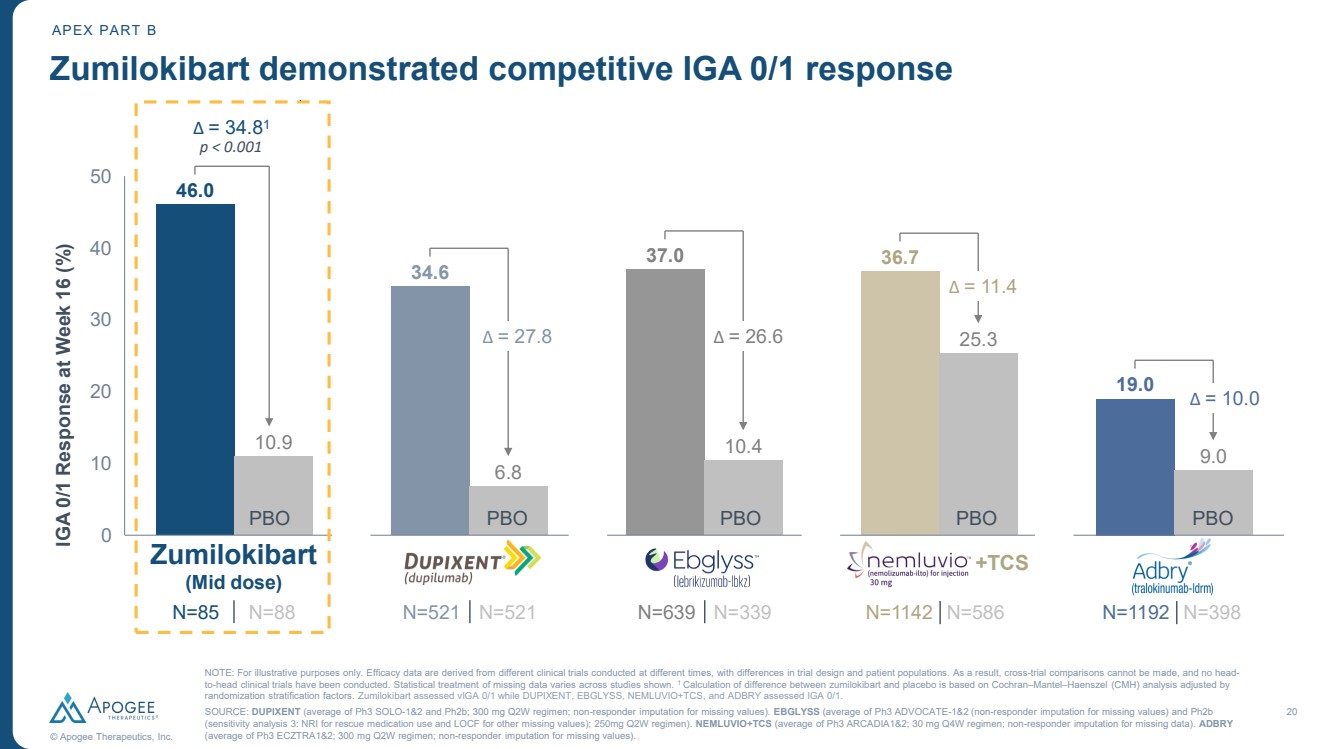
| 20 © Apogee Therapeutics, Inc. 46.0 10.9 34.6 6.8 37.0 10.4 36.7 25.3 19.0 9.0 0 10 20 30 40 50 IGA 0/1 Response at Week 16 (%) N=85 N=88 N=521 N=521 N=639 N=339 N=1142 N=586 Zumilokibart demonstrated competitive IGA 0/1 response Δ = 34.81 p < 0.001 Δ = 27.8 Δ = 26.6 Δ = 11.4 PBO PBO PBO PBO PBO Zumilokibart (Mid dose) +TCS N=1192 N=398 Δ = 10.0 APEX PART B NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Statistical treatment of missing data varies across studies shown. 1 Calculation of difference between zumilokibart and placebo is based on Cochran–Mantel–Haenszel (CMH) analysis adjusted by randomization stratification factors. Zumilokibart assessed vIGA 0/1 while DUPIXENT, EBGLYSS, NEMLUVIO+TCS, and ADBRY assessed IGA 0/1. SOURCE: DUPIXENT (average of Ph3 SOLO-1&2 and Ph2b; 300 mg Q2W regimen; non-responder imputation for missing values). EBGLYSS (average of Ph3 ADVOCATE-1&2 (non-responder imputation for missing values) and Ph2b (sensitivity analysis 3: NRI for rescue medication use and LOCF for other missing values); 250mg Q2W regimen). NEMLUVIO+TCS (average of Ph3 ARCADIA1&2; 30 mg Q4W regimen; non-responder imputation for missing data). ADBRY (average of Ph3 ECZTRA1&2; 300 mg Q2W regimen; non-responder imputation for missing values). |
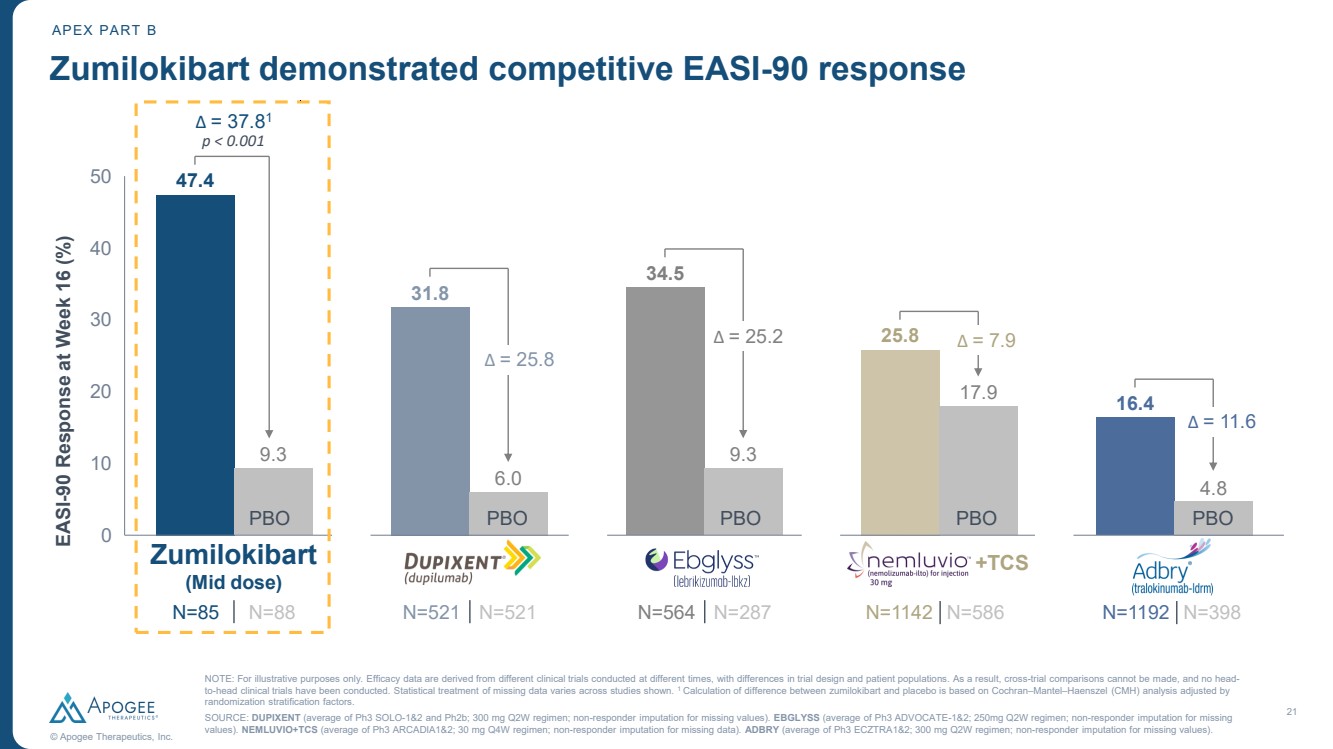
| 21 © Apogee Therapeutics, Inc. 47.4 9.3 31.8 6.0 34.5 9.3 25.8 17.9 16.4 4.8 0 10 20 30 40 50 EASI-90 Response at Week 16 (%) N=85 N=88 N=521 N=521 N=1142 N=586 Zumilokibart demonstrated competitive EASI-90 response Δ = 37.81 p < 0.001 Δ = 25.2 Δ = 25.8 Δ = 7.9 PBO PBO PBO PBO PBO Zumilokibart (Mid dose) +TCS N=1192 N=398 Δ = 11.6 APEX PART B N=564 N=287 NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Statistical treatment of missing data varies across studies shown. 1 Calculation of difference between zumilokibart and placebo is based on Cochran–Mantel–Haenszel (CMH) analysis adjusted by randomization stratification factors. SOURCE: DUPIXENT (average of Ph3 SOLO-1&2 and Ph2b; 300 mg Q2W regimen; non-responder imputation for missing values). EBGLYSS (average of Ph3 ADVOCATE-1&2; 250mg Q2W regimen; non-responder imputation for missing values). NEMLUVIO+TCS (average of Ph3 ARCADIA1&2; 30 mg Q4W regimen; non-responder imputation for missing data). ADBRY (average of Ph3 ECZTRA1&2; 300 mg Q2W regimen; non-responder imputation for missing values). |
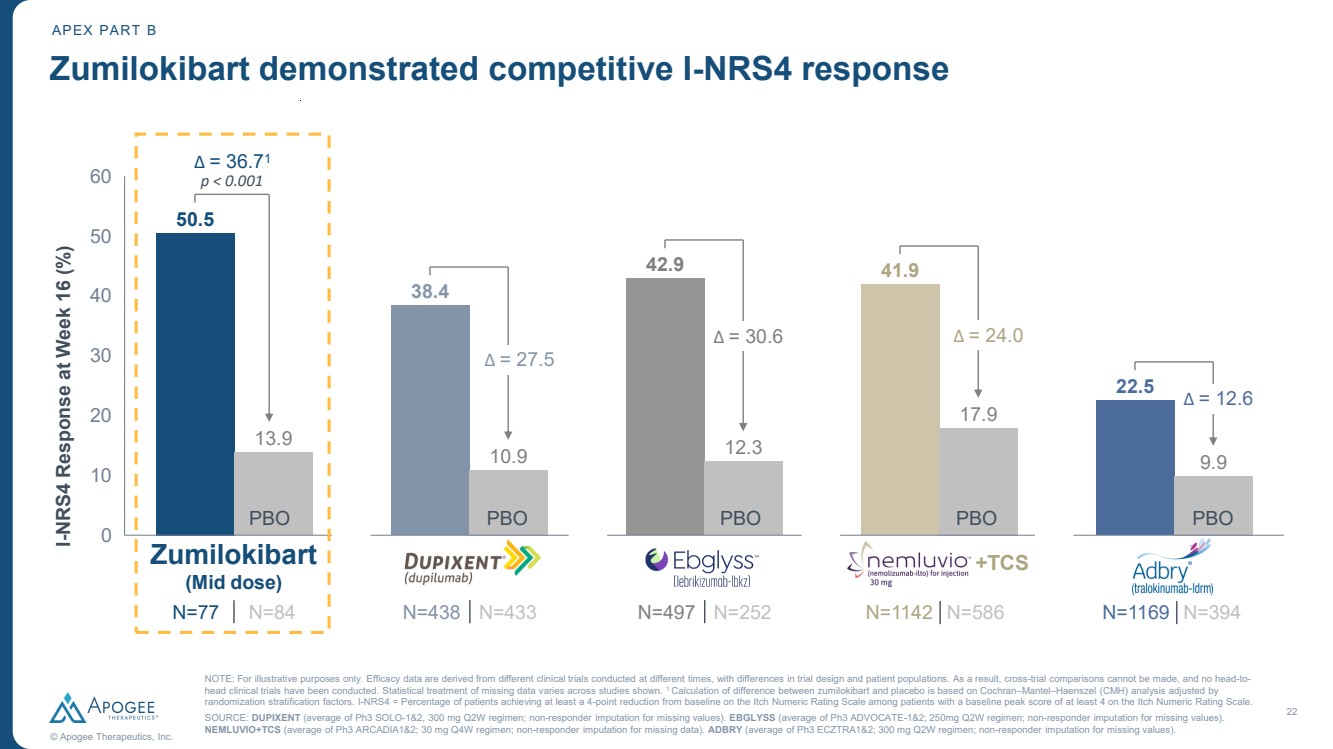
| 22 © Apogee Therapeutics, Inc. 50.5 13.9 38.4 10.9 42.9 12.3 41.9 17.9 22.5 9.9 0 10 20 30 40 50 60 I-NRS4 Response at Week 16 (%) N=77 N=84 Zumilokibart demonstrated competitive I-NRS4 response Δ = 36.71 p < 0.001 Δ = 30.6 Δ = 27.5 Δ = 24.0 PBO PBO PBO PBO PBO Zumilokibart (Mid dose) +TCS Δ = 12.6 APEX PART B N=438 N=433 N=497 N=252 N=1142 N=586 N=1169 N=394 NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Statistical treatment of missing data varies across studies shown. 1 Calculation of difference between zumilokibart and placebo is based on Cochran–Mantel–Haenszel (CMH) analysis adjusted by randomization stratification factors. I-NRS4 = Percentage of patients achieving at least a 4-point reduction from baseline on the Itch Numeric Rating Scale among patients with a baseline peak score of at least 4 on the Itch Numeric Rating Scale. SOURCE: DUPIXENT (average of Ph3 SOLO-1&2, 300 mg Q2W regimen; non-responder imputation for missing values). EBGLYSS (average of Ph3 ADVOCATE-1&2; 250mg Q2W regimen; non-responder imputation for missing values). NEMLUVIO+TCS (average of Ph3 ARCADIA1&2; 30 mg Q4W regimen; non-responder imputation for missing data). ADBRY (average of Ph3 ECZTRA1&2; 300 mg Q2W regimen; non-responder imputation for missing values). |
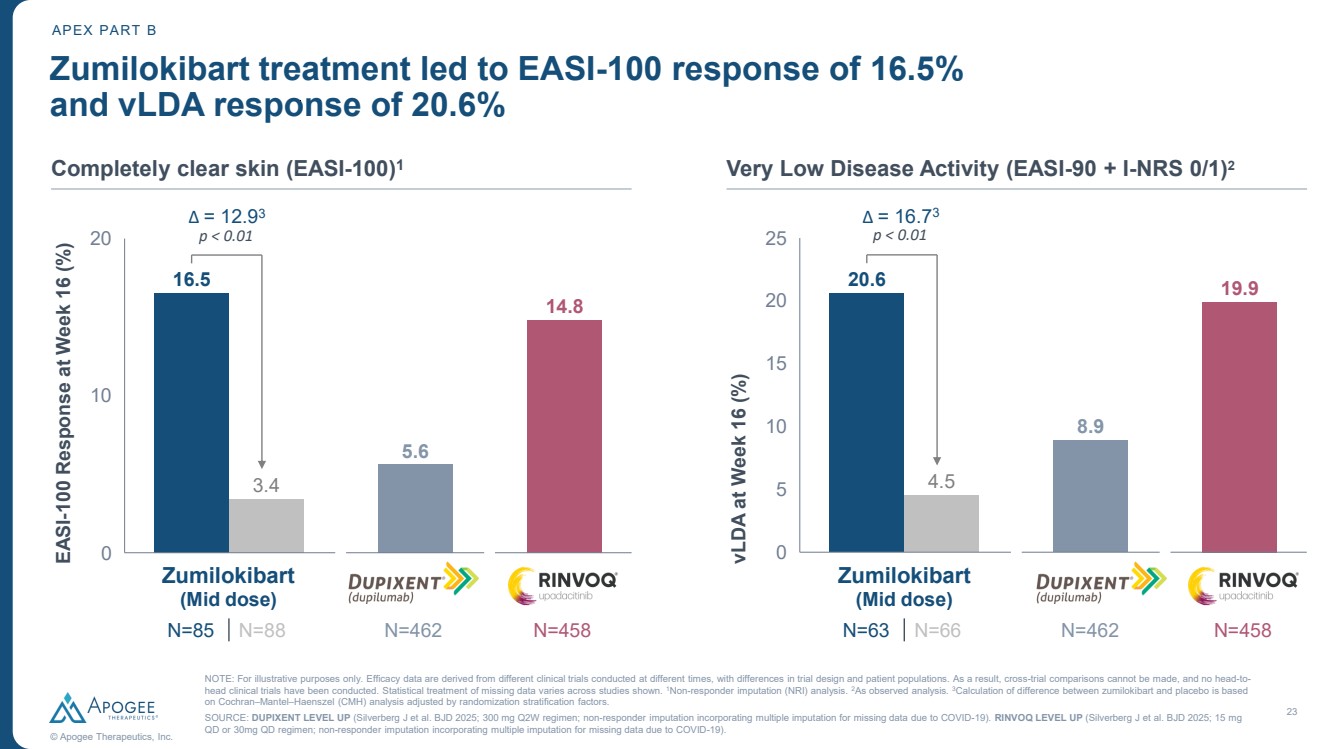
| 23 © Apogee Therapeutics, Inc. Zumilokibart treatment led to EASI-100 response of 16.5% and vLDA response of 20.6% APEX PART B Completely clear skin (EASI-100)1 Very Low Disease Activity (EASI-90 + I-NRS 0/1)2 16.5 3.4 5.6 14.8 0 10 20 EASI-100 Response at Week 16 (%) Δ = 12.93 p < 0.01 20.6 4.5 8.9 19.9 0 5 10 15 20 25 vLDA at Week 16 (%) Δ = 16.73 p < 0.01 N=462 N=458 N=462 N=458 Zumilokibart (Mid dose) N=85 N=88 Zumilokibart (Mid dose) N=63 N=66 NOTE: For illustrative purposes only. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Statistical treatment of missing data varies across studies shown. 1Non-responder imputation (NRI) analysis. 2As observed analysis. 3Calculation of difference between zumilokibart and placebo is based on Cochran–Mantel–Haenszel (CMH) analysis adjusted by randomization stratification factors. SOURCE: DUPIXENT LEVEL UP (Silverberg J et al. BJD 2025; 300 mg Q2W regimen; non-responder imputation incorporating multiple imputation for missing data due to COVID-19). RINVOQ LEVEL UP (Silverberg J et al. BJD 2025; 15 mg QD or 30mg QD regimen; non-responder imputation incorporating multiple imputation for missing data due to COVID-19). |
| Treatment Gaps in Atopic Dermatitis Ruth Ann Vleugels, MD, MPH, MBA Heidi and Scott C. Schuster Distinguished Chair in Dermatology Director, Atopic Dermatitis Program Mass General Brigham Department of Dermatology Professor of Dermatology, Harvard Medical School |
| 25 Atopic dermatitis is a severe, systemic disease that profoundly impacts patient quality of life 1) Primary Care Dermatology Society . 2) Bridgman et al., 2018. Ann Allergy Asthma Immunol. 3) Irish Skin Foundation. Loss of sleep Hospitalizations Growth restriction Depression Work sick leave Reduced physical activity |
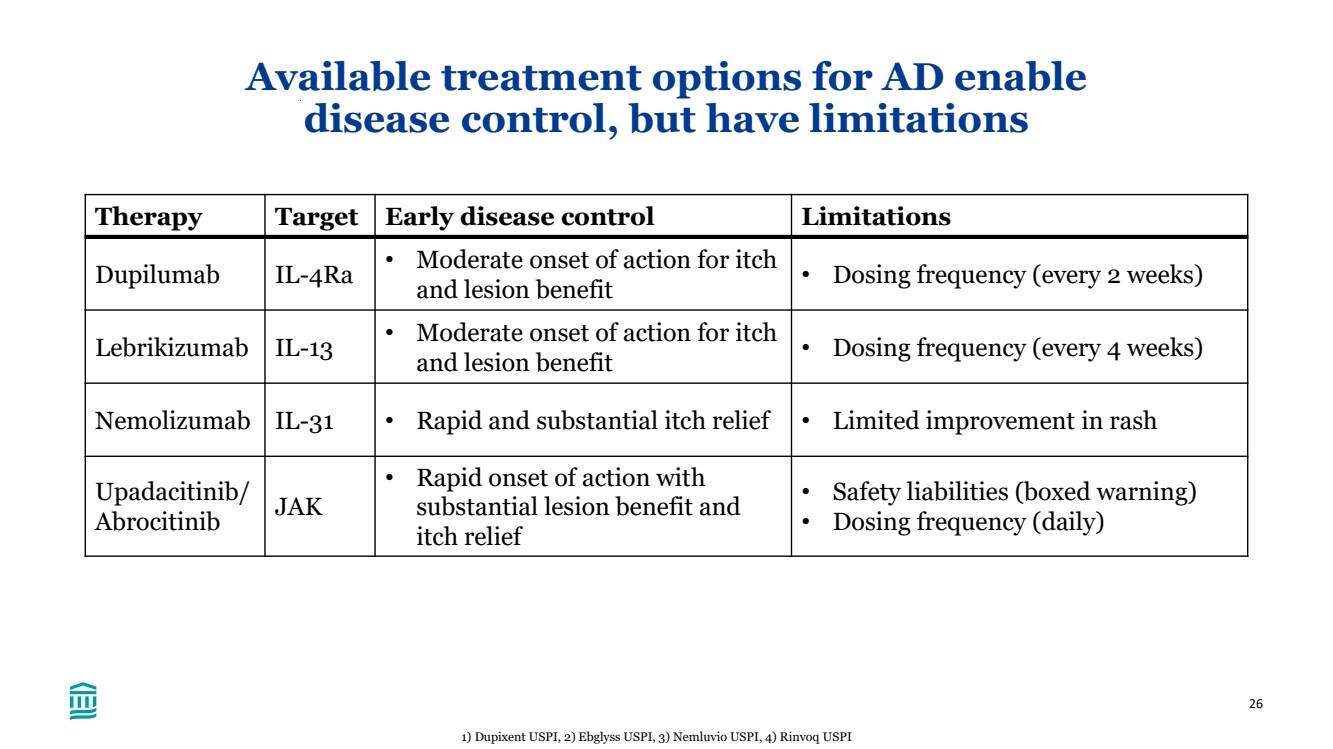
| 26 Available treatment options for AD enable disease control, but have limitations Therapy Target Early disease control Limitations Dupilumab IL-4Ra • Moderate onset of action for itch and lesion benefit • Dosing frequency (every 2 weeks) Lebrikizumab IL-13 • Moderate onset of action for itch and lesion benefit • Dosing frequency (every 4 weeks) Nemolizumab IL-31 • Rapid and substantial itch relief • Limited improvement in rash Upadacitinib/ Abrocitinib JAK • Rapid onset of action with substantial lesion benefit and itch relief • Safety liabilities (boxed warning) • Dosing frequency (daily) 1) Dupixent USPI, 2) Ebglyss USPI, 3) Nemluvio USPI, 4) Rinvoq USPI |
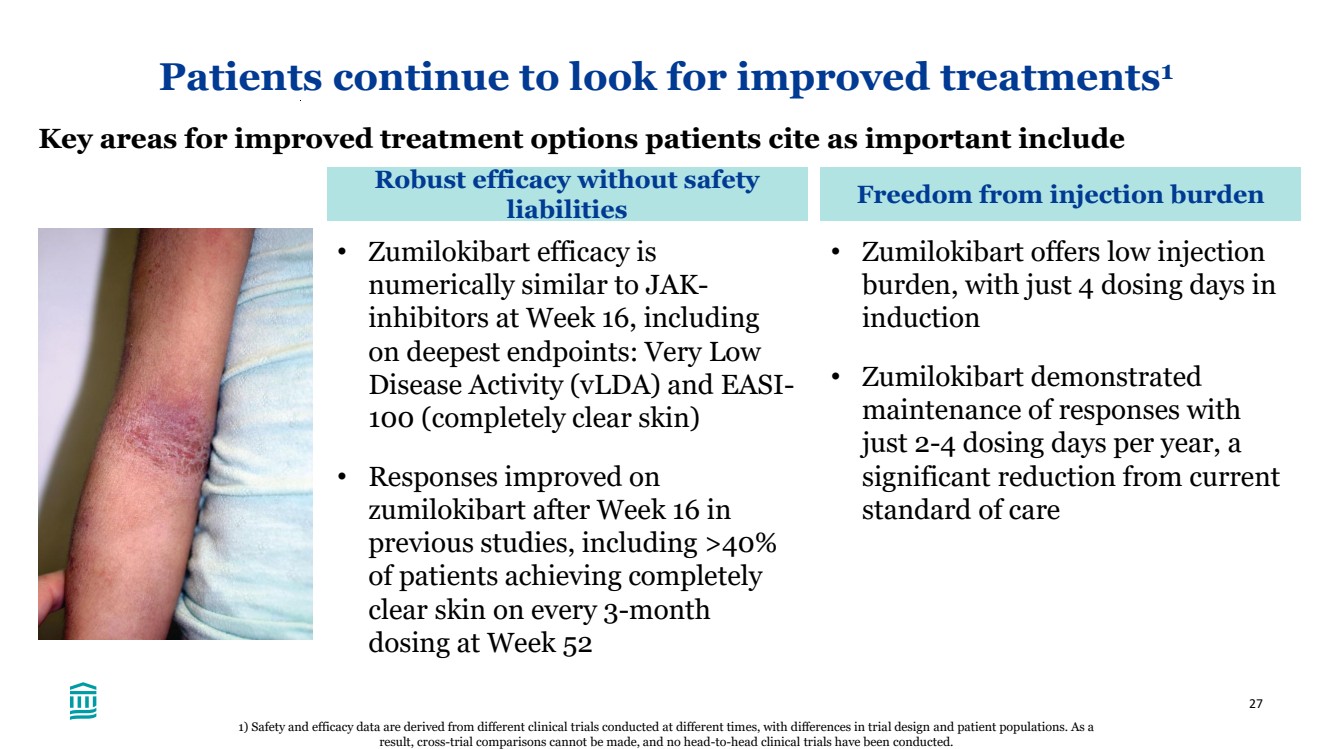
| 27 Patients continue to look for improved treatments1 Key areas for improved treatment options patients cite as important include Robust efficacy without safety liabilities Freedom from injection burden • Zumilokibart efficacy is numerically similar to JAK-inhibitors at Week 16, including on deepest endpoints: Very Low Disease Activity (vLDA) and EASI-100 (completely clear skin) • Responses improved on zumilokibart after Week 16 in previous studies, including >40% of patients achieving completely clear skin on every 3-month dosing at Week 52 • Zumilokibart offers low injection burden, with just 4 dosing days in induction • Zumilokibart demonstrated maintenance of responses with just 2-4 dosing days per year, a significant reduction from current standard of care 1) Safety and efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. |
| 28 Zumilokibart could address several unmet needs in AD1 • Although newer therapies have greatly improved the lives of patients with AD, substantial unmet need still exists for therapies that are safe and give patients freedom from disease burden • Zumilokibart was well-tolerated with a safety profile generally in line with the IL-4/13 class • Moreover, zumilokibart data presented today demonstrated efficacy numerically similar to that of JAK inhibitors and itch data numerically similar to nemolizumab • From previously presented data, zumilokibart showed improved responses over time with as infrequent dosing as every 3- to 6-months, providing patients freedom from their disease burden long-term • Together, zumilokibart data support its potential to become the biologic of choice for patients with moderate-to-severe atopic dermatitis 1) Safety and efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. |
| Zumilokibart Development Program Kristine Nograles, MD SVP, Clinical Development & Medical Affairs Amol Kamboj, MD SVP, Head of Clinical Development |

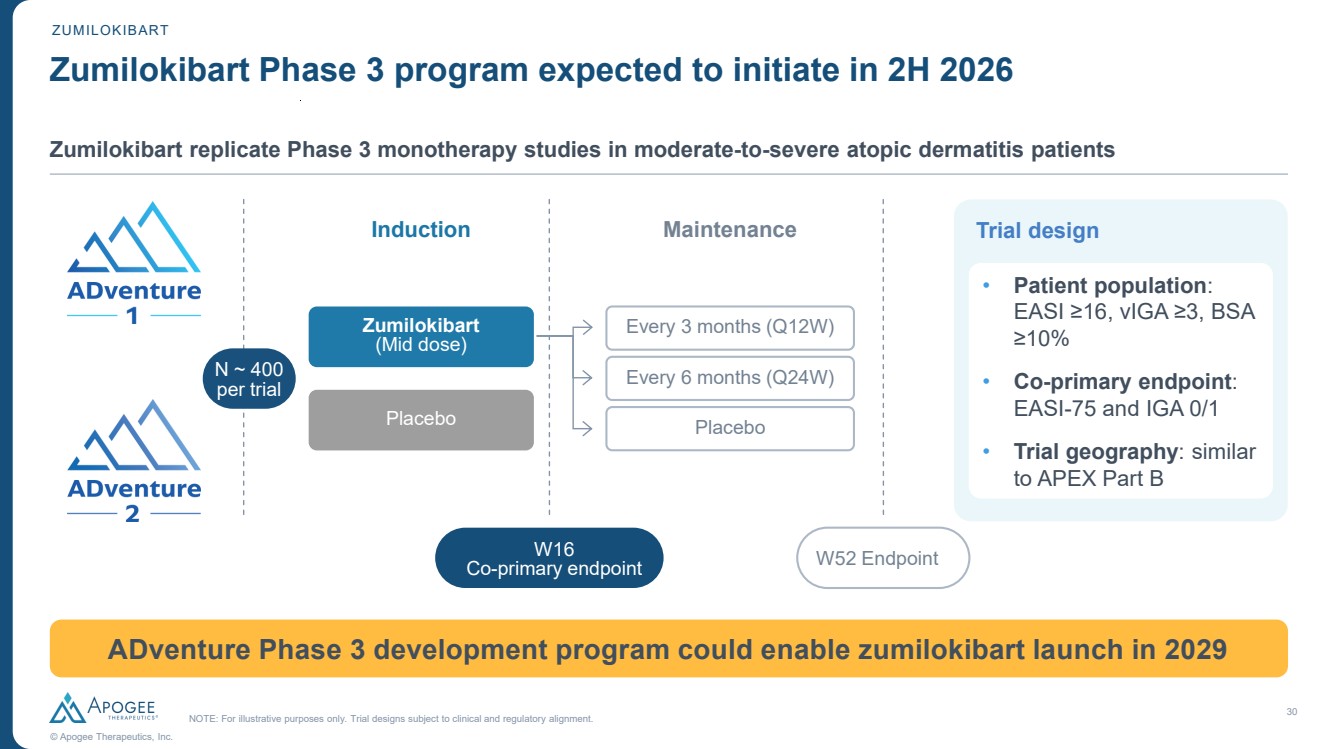
| 30 © Apogee Therapeutics, Inc. ZUMILOKIBART Zumilokibart Phase 3 program expected to initiate in 2H 2026 NOTE: For illustrative purposes only. Trial designs subject to clinical and regulatory alignment. Zumilokibart replicate Phase 3 monotherapy studies in moderate-to-severe atopic dermatitis patients Trial design • Patient population: EASI ≥16, vIGA ≥3, BSA ≥10% • Co-primary endpoint: EASI-75 and IGA 0/1 • Trial geography: similar to APEX Part B Every 3 months (Q12W) Maintenance W16 Co-primary endpoint W52 Endpoint Induction N ~ 400 per trial Zumilokibart (Mid dose) Placebo Placebo Every 6 months (Q24W) ADventure Phase 3 development program could enable zumilokibart launch in 2029 |
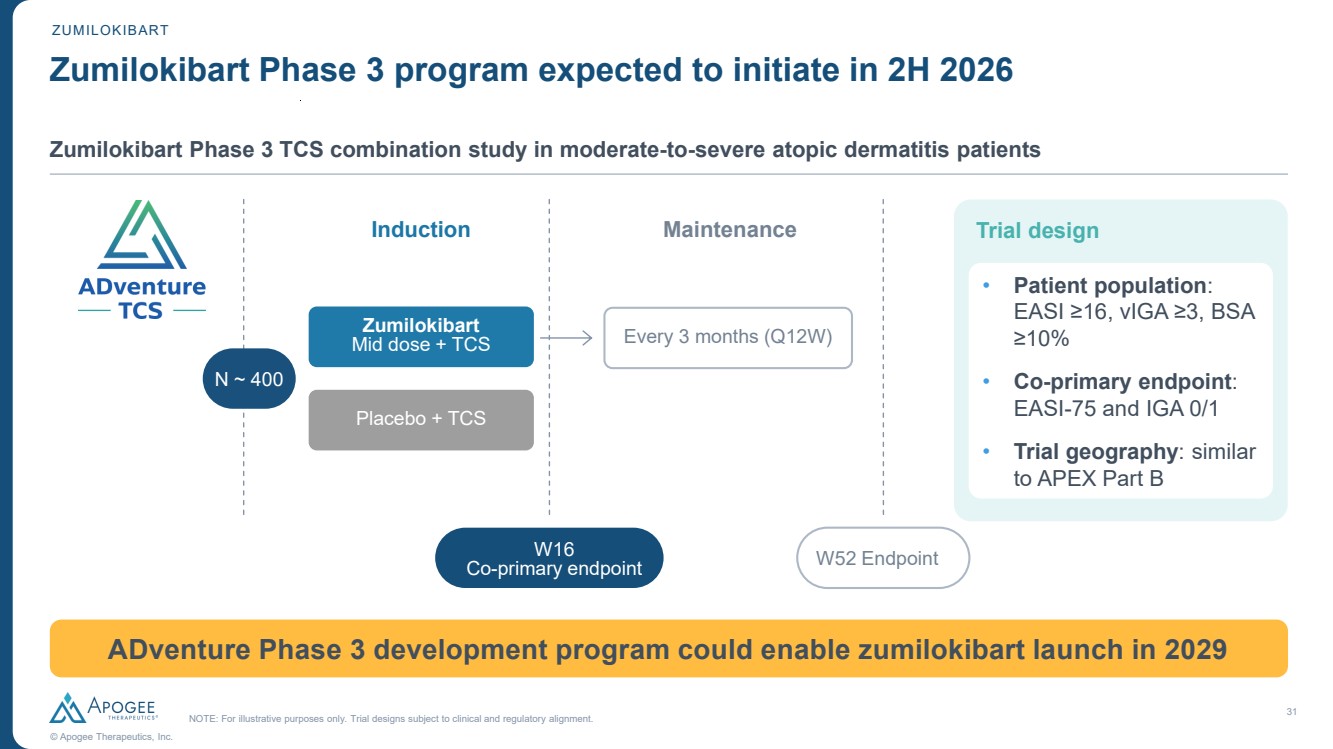
| 31 © Apogee Therapeutics, Inc. ZUMILOKIBART Zumilokibart Phase 3 program expected to initiate in 2H 2026 NOTE: For illustrative purposes only. Trial designs subject to clinical and regulatory alignment. Zumilokibart Phase 3 TCS combination study in moderate-to-severe atopic dermatitis patients Trial design • Patient population: EASI ≥16, vIGA ≥3, BSA ≥10% • Co-primary endpoint: EASI-75 and IGA 0/1 • Trial geography: similar to APEX Part B Maintenance W16 Co-primary endpoint W52 Endpoint Induction N ~ 400 Zumilokibart Mid dose + TCS Placebo + TCS ADventure Phase 3 development program could enable zumilokibart launch in 2029 Every 3 months (Q12W) |
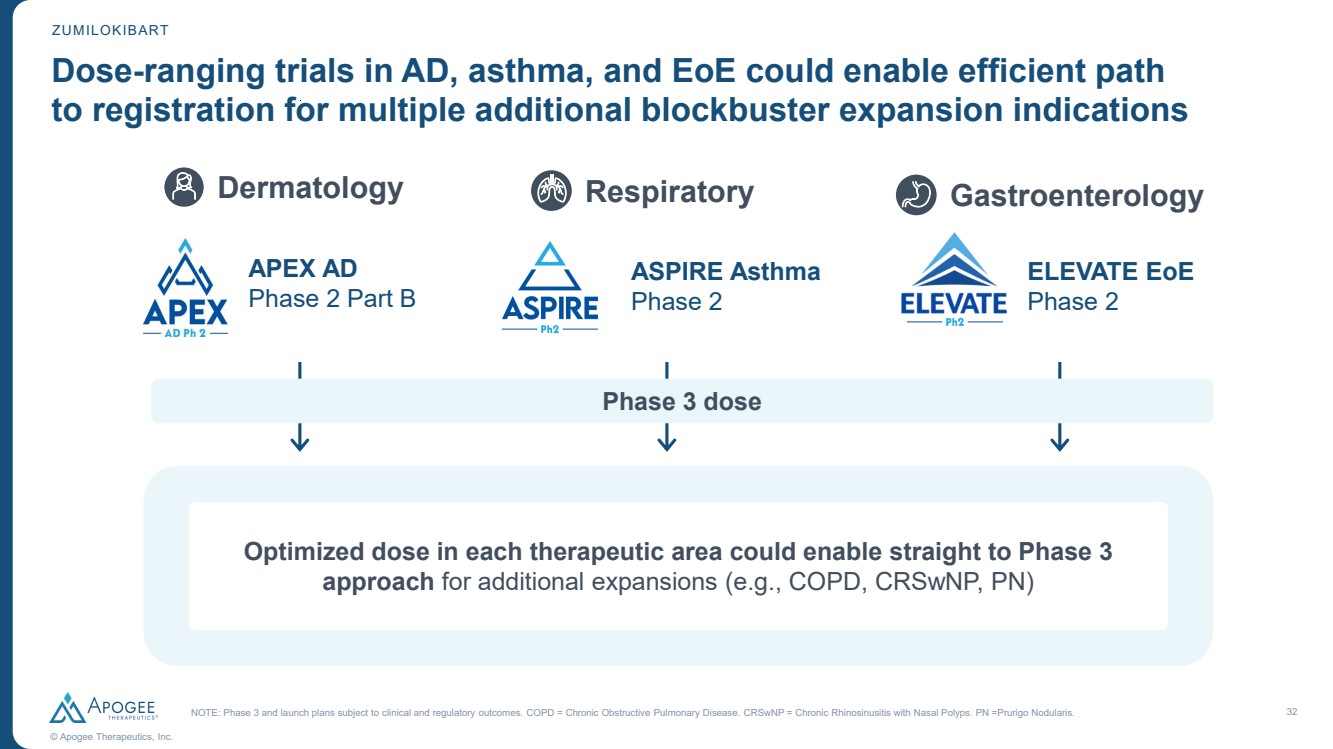
| 32 © Apogee Therapeutics, Inc. Dose-ranging trials in AD, asthma, and EoE could enable efficient path to registration for multiple additional blockbuster expansion indications ZUMILOKIBART NOTE: Phase 3 and launch plans subject to clinical and regulatory outcomes. COPD = Chronic Obstructive Pulmonary Disease. CRSwNP = Chronic Rhinosinusitis with Nasal Polyps. PN =Prurigo Nodularis. Respiratory ASPIRE Asthma Phase 2 Dermatology APEX AD Phase 2 Part B Gastroenterology ELEVATE EoE Phase 2 Phase 3 dose Optimized dose in each therapeutic area could enable straight to Phase 3 approach for additional expansions (e.g., COPD, CRSwNP, PN) |
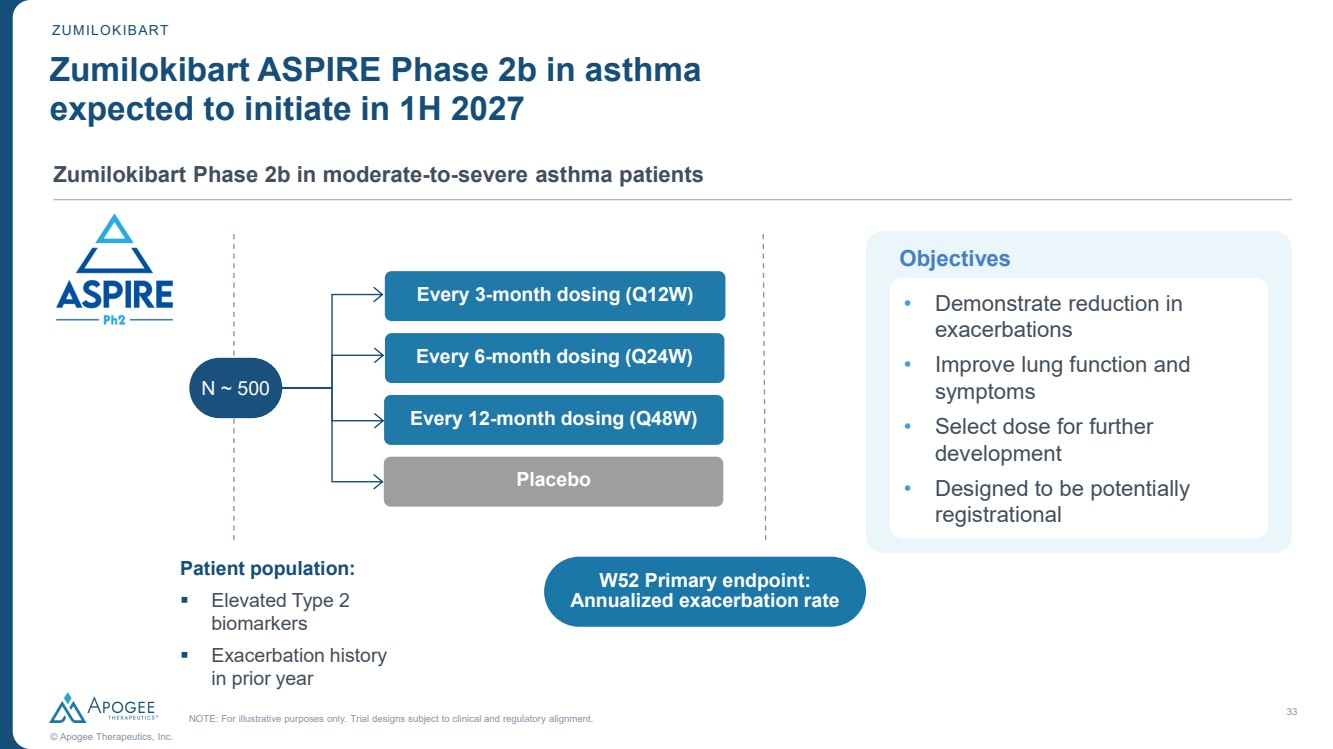
| 33 © Apogee Therapeutics, Inc. ZUMILOKIBART Zumilokibart ASPIRE Phase 2b in asthma expected to initiate in 1H 2027 NOTE: For illustrative purposes only. Trial designs subject to clinical and regulatory alignment. Zumilokibart Phase 2b in moderate-to-severe asthma patients W52 Primary endpoint: Annualized exacerbation rate Patient population: ▪ Elevated Type 2 biomarkers ▪ Exacerbation history in prior year Objectives • Demonstrate reduction in exacerbations • Improve lung function and symptoms • Select dose for further development • Designed to be potentially registrational Every 3-month dosing (Q12W) Every 6-month dosing (Q24W) Placebo Every 12-month dosing (Q48W) N ~ 500 |
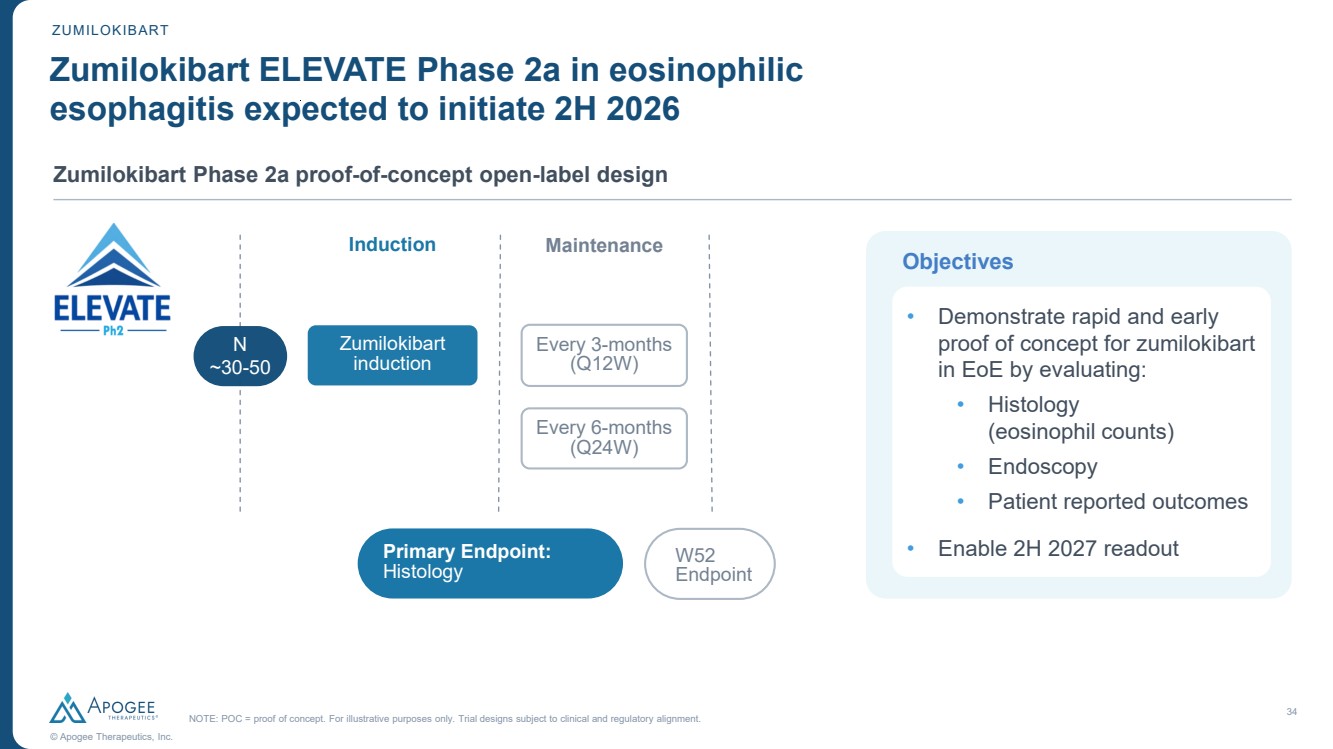
| 34 © Apogee Therapeutics, Inc. NOTE: POC = proof of concept. For illustrative purposes only. Trial designs subject to clinical and regulatory alignment. Induction Maintenance Primary Endpoint: Histology W52 Endpoint N ~30-50 Every 3-months (Q12W) Zumilokibart induction Every 6-months (Q24W) ZUMILOKIBART Zumilokibart ELEVATE Phase 2a in eosinophilic esophagitis expected to initiate 2H 2026 Zumilokibart Phase 2a proof-of-concept open-label design Objectives • Demonstrate rapid and early proof of concept for zumilokibart in EoE by evaluating: • Histology (eosinophil counts) • Endoscopy • Patient reported outcomes • Enable 2H 2027 readout |
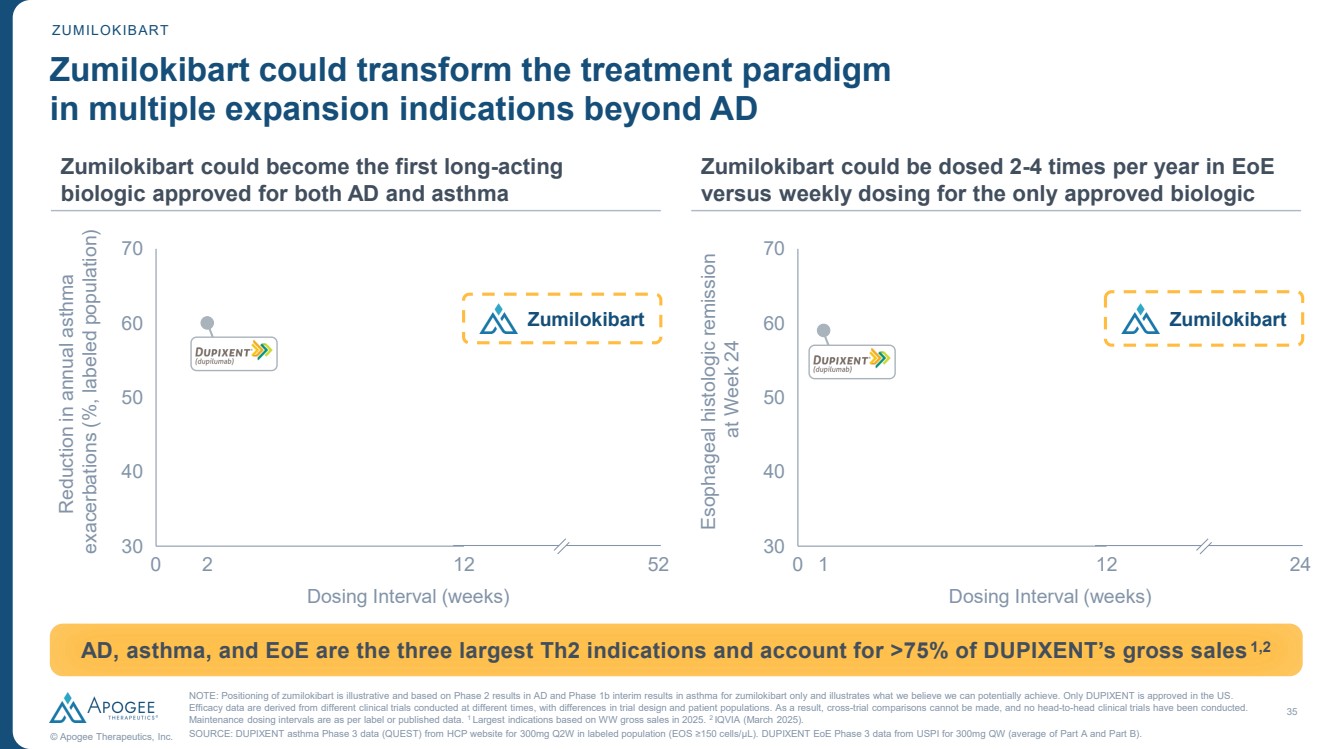
| 35 © Apogee Therapeutics, Inc. ZUMILOKIBART Zumilokibart could transform the treatment paradigm in multiple expansion indications beyond AD Zumilokibart could become the first long-acting biologic approved for both AD and asthma Zumilokibart could be dosed 2-4 times per year in EoE versus weekly dosing for the only approved biologic 0 2 12 30 40 50 60 70 Reduction in annual asthma exacerbations (%, labeled population) Dosing Interval (weeks) Zumilokibart AD, asthma, and EoE are the three largest Th2 indications and account for >75% of DUPIXENT’s gross sales1,2 52 0 1 12 30 40 50 60 70 Esophageal histologic remission at Week 24 Dosing Interval (weeks) Zumilokibart 24 NOTE: Positioning of zumilokibart is illustrative and based on Phase 2 results in AD and Phase 1b interim results in asthma for zumilokibart only and illustrates what we believe we can potentially achieve. Only DUPIXENT is approved in the US. Efficacy data are derived from different clinical trials conducted at different times, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Maintenance dosing intervals are as per label or published data. 1 Largest indications based on WW gross sales in 2025. 2 IQVIA (March 2025). SOURCE: DUPIXENT asthma Phase 3 data (QUEST) from HCP website for 300mg Q2W in labeled population (EOS ≥150 cells/μL). DUPIXENT EoE Phase 3 data from USPI for 300mg QW (average of Part A and Part B). |
| Building a Leading I&I Company Michael Henderson, MD Chief Executive Officer |

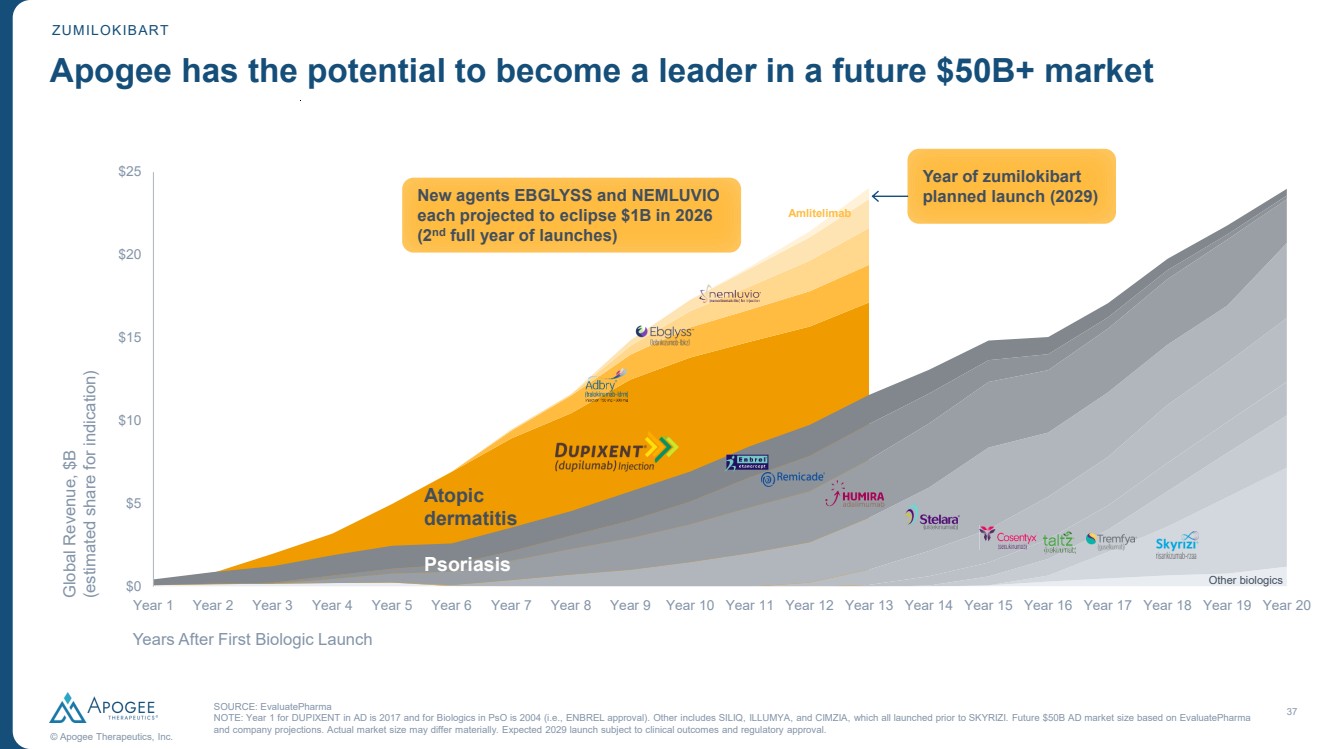
| 37 © Apogee Therapeutics, Inc. SOURCE: EvaluatePharma NOTE: Year 1 for DUPIXENT in AD is 2017 and for Biologics in PsO is 2004 (i.e., ENBREL approval). Other includes SILIQ, ILLUMYA, and CIMZIA, which all launched prior to SKYRIZI. Future $50B AD market size based on EvaluatePharma and company projections. Actual market size may differ materially. Expected 2029 launch subject to clinical outcomes and regulatory approval. Apogee has the potential to become a leader in a future $50B+ market $0 $5 $10 $15 $20 $25 Global Revenue, $B (estimated share for indication) Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Year 10 Year 11 Year 12 Year 13 Year 14 Year 15 Year 16 Year 17 Year 18 Year 19 Year 20 Years After First Biologic Launch $0 $5 $10 $15 $20 $25 Psoriasis Atopic dermatitis Other biologics Year of zumilokibart planned launch (2029) Amlitelimab New agents EBGLYSS and NEMLUVIO each projected to eclipse $1B in 2026 (2nd full year of launches) ZUMILOKIBART |
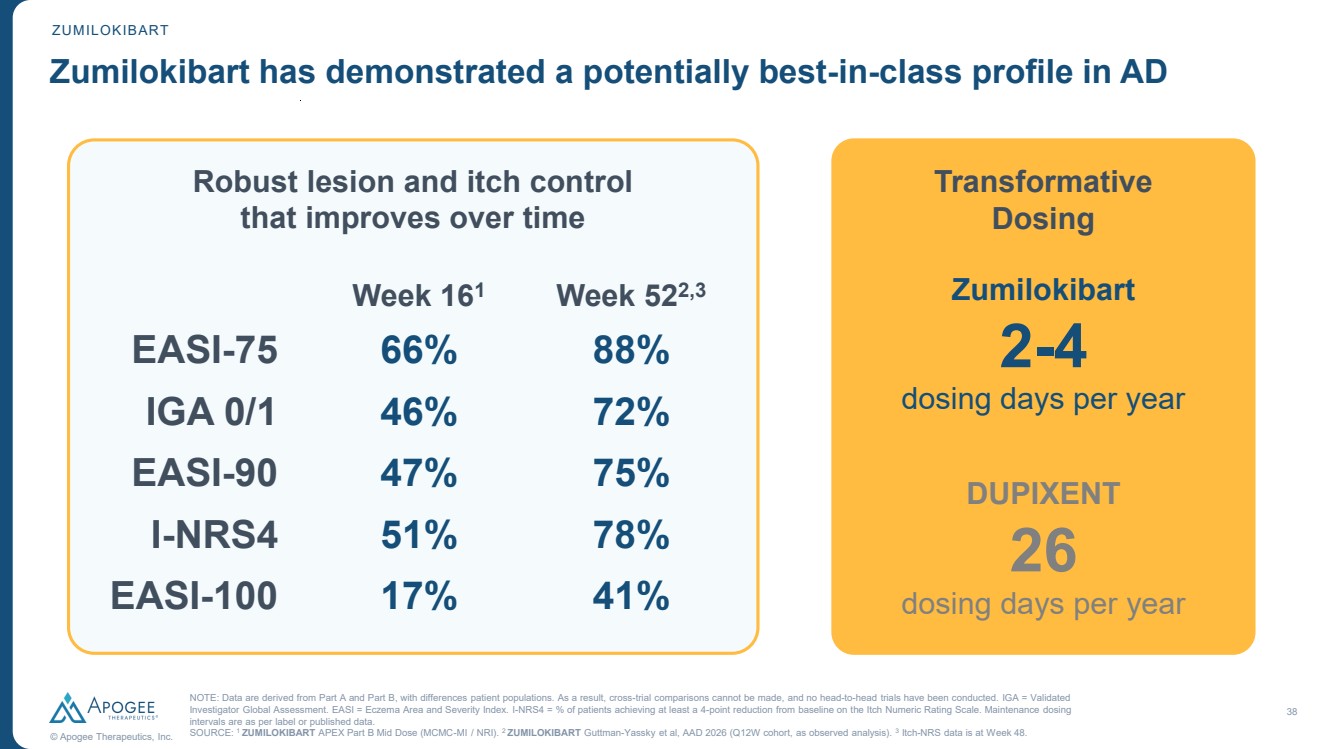
| 38 © Apogee Therapeutics, Inc. Zumilokibart has demonstrated a potentially best-in-class profile in AD Robust lesion and itch control that improves over time Week 161 Week 522,3 EASI-75 66% 88% IGA 0/1 46% 72% EASI-90 47% 75% I-NRS4 51% 78% EASI-100 17% 41% Transformative Dosing 2-4 Zumilokibart dosing days per year 26 DUPIXENT dosing days per year ZUMILOKIBART NOTE: Data are derived from Part A and Part B, with differences patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head trials have been conducted. IGA = Validated Investigator Global Assessment. EASI = Eczema Area and Severity Index. I-NRS4 = % of patients achieving at least a 4-point reduction from baseline on the Itch Numeric Rating Scale. Maintenance dosing intervals are as per label or published data. SOURCE: 1 ZUMILOKIBART APEX Part B Mid Dose (MCMC-MI / NRI). 2 ZUMILOKIBART Guttman-Yassky et al, AAD 2026 (Q12W cohort, as observed analysis). 3 Itch-NRS data is at Week 48. |
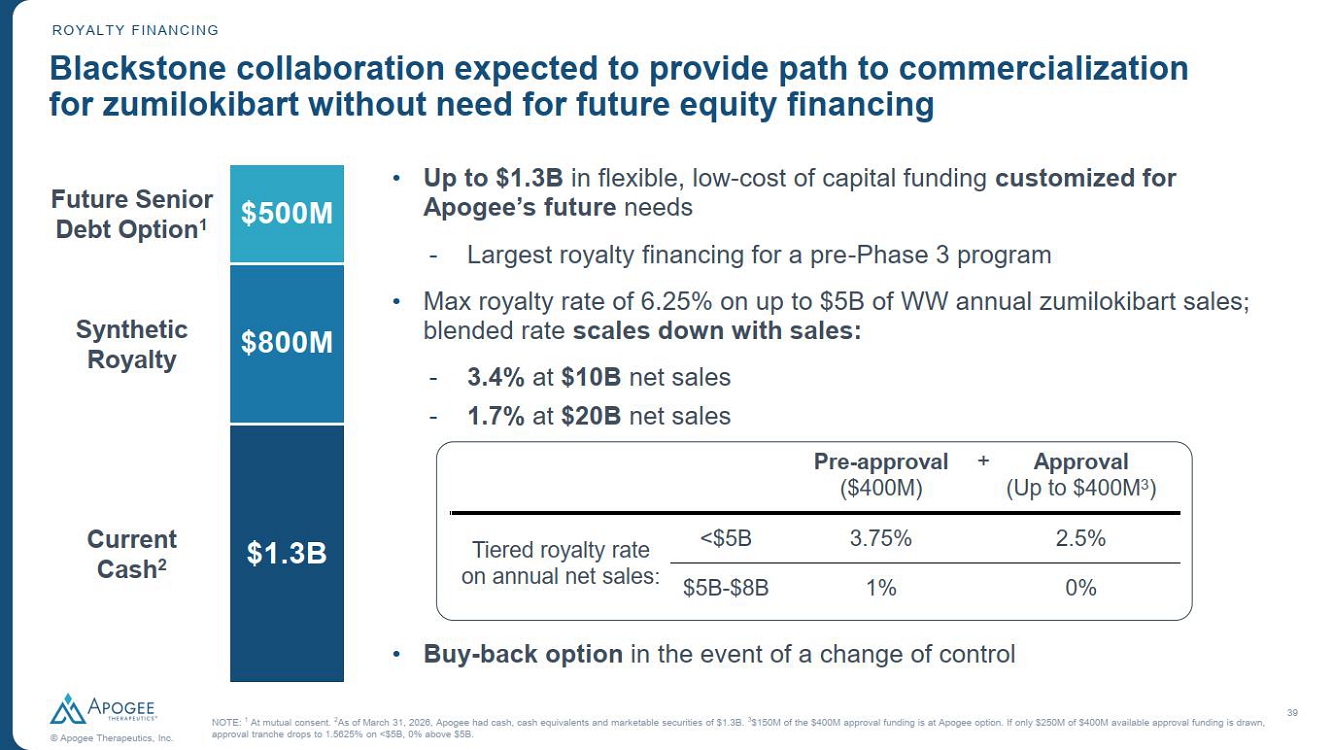
| 39 © Apogee Therapeutics, Inc. ROYALTY FINANCING Blackstone collaboration expected to provide path to commercialization for zumilokibart without need for future equity financing $500M $800M $1.3B Future Senior Debt Option1 Synthetic Royalty Current Cash2 3 • Up to $1.3B in flexible, low-cost of capital funding customized for Apogee’s future needs - Largest royalty financing for a pre-Phase 3 program • Max royalty rate of 6.25% on up to $5B of WW annual zumilokibart sales; blended rate scales down with sales: - 3.4% at $10B net sales - 1.7% at $20B net sales • Buy-back option in the event of a change of control NOTE: 1 At mutual consent. 2As of March 31, 2026, Apogee had cash, cash equivalents and marketable securities of $1.3B. 3$150M of the $400M approval funding is at Apogee option. If only $250M of $400M available approval funding is drawn, approval tranche drops to 1.5625% on <$5B, 0% above $5B. Pre-approval ($400M) Approval (Up to $400M3 ) Tiered royalty rate on annual net sales: <$5B 3.75% 2.5% $5B-$8B 1% 0% + |
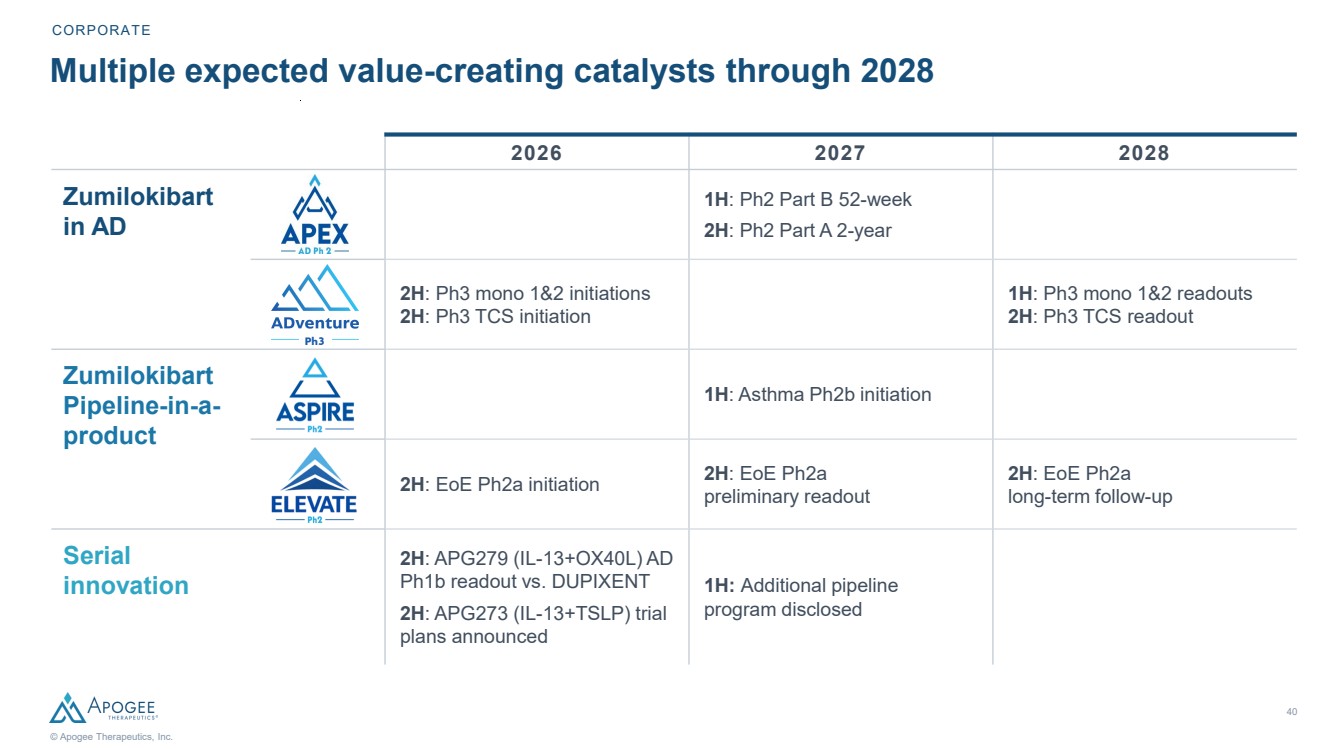
| 40 © Apogee Therapeutics, Inc. 2026 2027 2028 1H: Ph2 Part B 52-week 2H: Ph2 Part A 2-year 2H: Ph3 mono 1&2 initiations 2H: Ph3 TCS initiation 1H: Ph3 mono 1&2 readouts 2H: Ph3 TCS readout 1H: Asthma Ph2b initiation 2H: EoE Ph2a initiation 2H: EoE Ph2a preliminary readout 2H: EoE Ph2a long-term follow-up 2H: APG279 (IL-13+OX40L) AD Ph1b readout vs. DUPIXENT 2H: APG273 (IL-13+TSLP) trial plans announced 1H: Additional pipeline program disclosed Multiple expected value-creating catalysts through 2028 CORPORATE Zumilokibart in AD Zumilokibart Pipeline-in-a-product Serial innovation Ph3 |
| Apogee /ˈapəjē/ noun The highest point in the development of something; a climax or culmination |
