UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 6-K
REPORT OF FOREIGN
PRIVATE ISSUER PURSUANT TO RULE 13a-16 OR 15d-16 UNDER
THE SECURITIES EXCHANGE ACT OF 1934
June 1, 2026
Commission File Number: 001-39363
IMMATICS N.V.
Paul-Ehrlich-Straße 15
72076 Tübingen, Federal Republic of Germany
(Address of principal executive office)
Indicate by check mark whether the registrant files or will file annual reports under cover of Form 20-F or Form 40-F:
| Form 20-F |
☒ |
Form 40-F |
☐ | |
INFORMATION CONTAINED IN THIS REPORT ON FORM 6-K
IMA203CD8 Data Release
On May 30, 2026, Immatics N.V. (the “Company” or “Immatics”) announced updated Phase 1 data for its IMA203CD8 PRAME TCR T-cell therapy in gynecologic cancers and synovial sarcoma.
Gynecologic Cancers
Patient Population. As of the March 30, 2026 data cutoff, 27 heavily pretreated patients with gynecologic cancers (24 patients with ovarian carcinoma and three with uterine cancer) received a one-time infusion of IMA203CD8. The median total infused dose across seven escalating dose levels was 3.3×109 TCR T cells (range 0.5×109 – 12.5×109) for ovarian carcinoma and 3.2×109 TCR T cells (range 1.3×109 – 10.1×109) for uterine cancer. All patients were heavily pretreated, including at least one prior line of platinum-based regimen. Patients with ovarian carcinoma had a median of four prior lines of systemic treatment (range 1 – 7), patients with uterine cancer had a median of two prior lines (range 1 – 3). The efficacy-evaluable patient population included 26 patients, 19 of whom were treated at clinically relevant doses (≥DL4c, median 5.4x109 TCR T cells, range 1.4×109 – 12.5×109): 17 with ovarian carcinoma and two with uterine cancer.
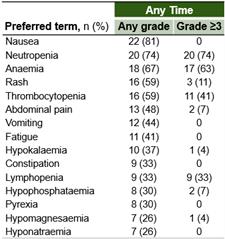
Safety Data. IMA203CD8 demonstrated predictable and manageable tolerability. The most frequent treatment-emergent adverse events (“TEAEs”) were anticipated cytopenias associated with lymphodepletion. Expected and manageable cytokine release syndrome (“CRS”) was observed, consistent with the mechanism of action (Grade 1: 44%, Grade 2: 44%, Grade 3: 7%). Some patients infrequently experienced immune effector cell-associated neurotoxicity syndrome (“ICANS”) and hemophagocytic lymphohistiocytosis (“HLH”) (any Grade: 7% each). No Grade 5 IMA203CD8-related adverse event was observed. Two dose-limiting toxicities (“DLT”) occurred and the maximum tolerated dose (“MTD”) was not reached. The following table shows TEAEs occurring in 25% or more of patients:
Based on the manageable tolerability profile, the Company expects to determine the recommended Phase 2 dose (“RP2D”) in 2026.
Anti-Tumor Activity. A one-time infusion of IMA203CD8 PRAME cell therapy showed anti-tumor activity in gynecologic cancers at clinically relevant doses (≥ DL4c):
| · | Objective response rate (“ORR”) was 63% (12/19) and confirmed ORR (“cORR”) was 50% (9/18) |
| o | There were two confirmed complete responses and two unconfirmed complete responses |
| o | 89% (8/9) of confirmed responses were ongoing as of the data cutoff with longest ongoing response at 12 months post infusion (metabolic complete response) |
| o | Responses were observed with and without low-dose IL-2 |
| · | Tumor reduction was 78% (14/18) |
| · | Disease Control Rate (“DCR”) at week 6 was 68% (13/19) |
| · | Median duration of response (“mDOR”), median progression free survival (“mPFS”) and median overall survival (“mOS”) were not reached, with median follow-up times (“mFU”) of 3.9, 5.3 and 5.3 months, respectively |
The graphic below sets forth the observed anti-tumor activity at clinically relevant doses (≥ DL4c).
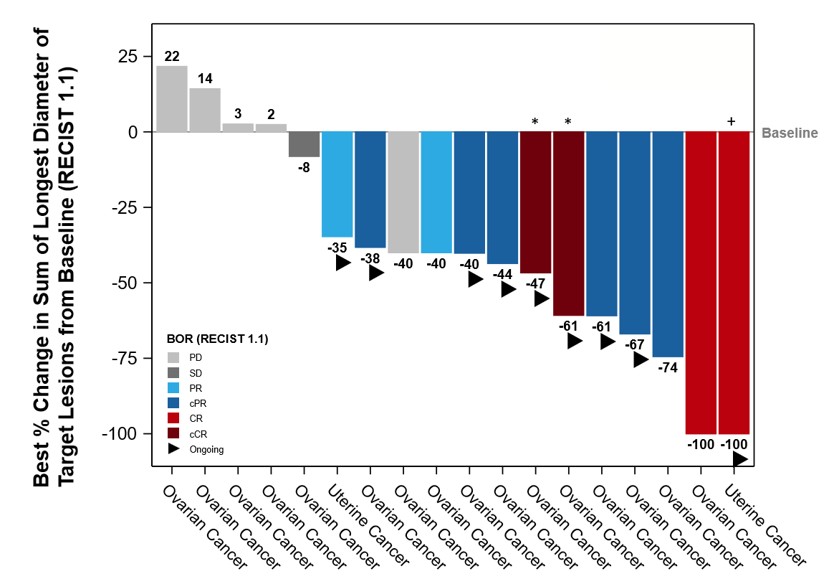
* For those patients who achieved a (c)CR with <100% changes from baseline, target lesions were lymph nodes that resolved to <10 mm. + Patient had a PR prior to CR. BOR, best overall response; (c)CR, (confirmed) complete response; (c)ORR, (confirmed) objective response rate; PD, progressive disease; (c)PR, (confirmed) partial response; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease.
Synovial Sarcoma
Patient Population. As of the March 30, 2026 data cutoff, 12 heavily pretreated patients with synovial sarcoma were treated with a one-time infusion of IMA203CD8. The median total infused dose was 1.59×109 TCR T cells (range 0.89×109 – 10.00×109). Patients had a median of two prior lines of systemic therapy (range, 1 – 5).
Safety Data. IMA203CD8 demonstrated expected and manageable tolerability. The most frequent TEAEs were anticipated cytopenias associated with lymphodepletion. Expected and manageable CRS was observed, consistent with the mechanism of action (Grade 1: 42%, Grade 2: 42%, Grade 3: 17%). No patient experienced ICANS or HLH. No Grade 5 IMA203CD8-related adverse event was observed. One DLT occurred and the MTD was not reached. The following table shows TEAEs occurring in 25% or more of patients:
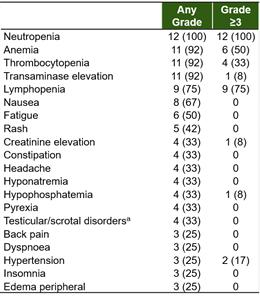
a Testicular/scrotal disorders includes grouped terms.
Anti-Tumor Activity. A one-time infusion of IMA203CD8 showed promising anti-tumor activity with deep and durable response in synovial sarcoma across all doses:
| · | ORR was 67% (8/12) and cORR was 64% (7/11) |
| o | 4 ongoing responses, including 1 confirmed complete response, with longest response ongoing at ~ 3 years |
| · | Tumor reduction was 92% (11/12) |
| · | DCR at week 6 was 100% (12/12) |
| · | mDOR was 14.8 months (3.7, 31.8+) at mFU of 31.0 months |
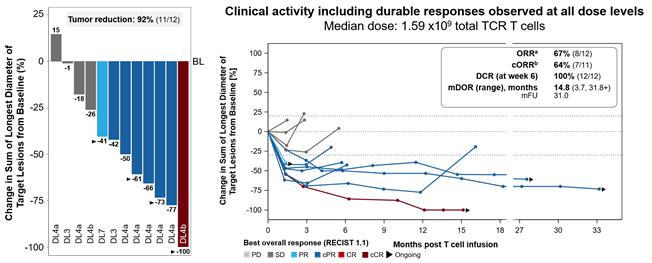
a ORR: according to RECIST 1.1 at any post-BL scan, PD or death at any prior timepoint; b cORR for patients with ≥2 post-BL scans per RECIST 1.1, PD or death at any prior timepoint, those with ongoing unconfirmed PR/CR at the data cutoff were excluded. BL, baseline; BOR: best overall response; (c)CR, (confirmed) complete response; (c)ORR, (confirmed) objective response rate; (c)PR, (confirmed) partial response; DCR, disease control rate; mDOR, median duration of response; mFU, median follow-up; NR, not reached; PD, progressive disease; SD, stable disease; TCR, T-cell receptor.
Next Development Steps
The clinical activity observed in ovarian cancer, a tumor type generally associated with lower levels of PRAME expression, together with the observed activity across tumor types with different and distinct tumor microenvironments, supports the broad applicability of IMA203CD8 across solid tumors with differing levels of PRAME and tumor biology, starting with ovarian and uterine cancer. Updated data from the ongoing study, including durability follow-up at the RP2D, are planned for presentation in the second half of 2026. The Company is expanding clinical evaluation of IMA203CD8 into additional PRAME-positive solid tumor indications to more fully assess its therapeutic potential.
IMA401 Data Release
On May 31, 2026, the Company announced extended data from the ongoing Phase 1 clinical trial evaluating its TCR bispecific (TCER®) candidate IMA401 targeting MAGEA4/8 in heavily pretreated patients with solid tumors, including head and neck cancer and lung cancer.
Patient Population. As of the March 2, 2026 data cutoff, 61 heavily pretreated patients with recurrent and/or refractory solid tumors across more than 15 different tumor types were treated with IMA401 with or without pembrolizumab, an immune checkpoint inhibitor (“ICI”). Patients had a median of three prior lines of systemic therapy (range: 1 – 8). 44 patients were treated at RP2D (1 – 2 mg), with 32 receiving monotherapy and 12 receiving the combination of IMA401 and pembrolizumab. Among these patients, head and neck cancer represented the largest subgroup treated at RP2D (n=14).
Safety Data. IMA401 demonstrated manageable tolerability. The tolerability profile of IMA401 with or without pembrolizumab was consistent across patient populations. The most frequent treatment-related adverse events (“TRAEs”) were expected and manageable CRS and transient lymphopenia, consistent with the mechanism of action, as well as neutropenia, mostly transient and manageable. No patient experienced ICANS. Five DLTs occurred (which were manageable in four cases) but no DLTs occurred at RP2D with dexamethasone premedication, and the MTD was not reached. Tolerability of IMA401 at RP2D in combination with pembrolizumab was consistent with IMA401 as a monotherapy at RP2D, with no overlapping and/or additive toxicity observed. At RP2D, tolerability was observed to be favorable, supporting broad combinability of IMA401. The following table shows TRAEs for IMA401 as monotherapy and IMA401 at RP2D with and without pembrolizumab:
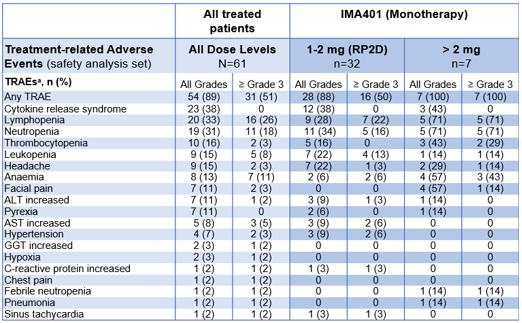
a All TRAEs at least possibly related to IMA401 infusion and/or pembrolizumab infusion with grade 1-2 occurring in at least 10% of all patients, all events with ≥ Grade 3; b in patients with and without dexamethasone pre-medication; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyltransferase.
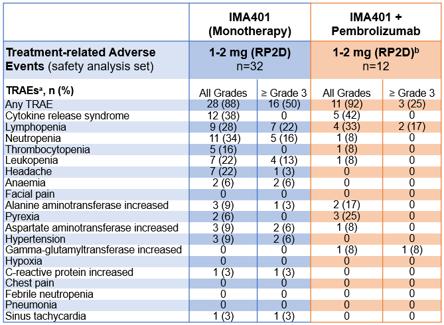
a All TRAEs at least possibly related to IMA401 infusion and/or pembrolizumab infusion with grade 1-2 occurring in at least 10% of all patients, all events with ≥ grade 3 and typical ICI-associated toxicities; b IMA401 dose in pembrolizumab expansion cohorts were 1 mg (n=8) or 1.5 mg (n=4).
Anti-Tumor Activity. Patients treated with IMA401 at RP2D as a monotherapy or in combination with pembrolizumab demonstrated clinical activity across multiple solid tumor indications, including melanoma, sqNSCLC, head and neck cancer and others:
| · | For head and neck cancer patients (largest patient subgroup treated at RP2D), cORR was 29% (4/14), DCR was 64% (9/14) and mDOR was 8.8 months. The 12-month overall survival (“OS”) rate was 63% and the six-month progression-free survival (“PFS”) rate was 43%. All responders achieved deep tumor reduction ranging from 60% – 100% and three of four responders were ongoing at data cutoff. |
| · | For melanoma patients: cORR was 33% (2/6) and DCR was 67% (4/6). Both confirmed responses lasted beyond six months post treatment, with one ongoing for >2.5 years. |
| · | A patient case highlighted a patient with ICI-resistant sqNSCLC who received IMA401 plus pembrolizumab in fifth-line (prior best overall response: stable disease) and achieved a partial response with shrinkage of all target lesions. |
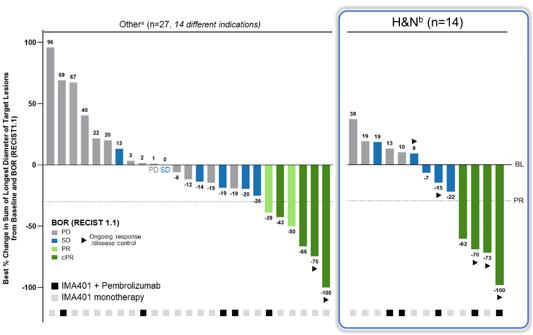
a Two patients not shown in plot due to clinical progression before post-infusion scan. b One patient not shown in plot due to clinical progression before post-infusion scan. BL, Baseline; BOR, Best overall response; (c)PR, (confirmed) partial response; H&N, head and neck cancer; PD, progressive disease; RECIST, response evaluation criteria in solid tumors; SD, stable disease.
Preclinical Data. Target expression data from analyzed tumor samples showed that > 90% of patients with sqNSCLC are positive for PRAME and/or MAGEA4/8, and ~60% of patients with sqNSCLC are positive for both
targets, suggesting that a combination therapy against both targets could boost anti-tumor activity and counteract potential tumor escape mechanisms. IMA401/IMA402 combination demonstrated synergistic anti-tumor activity in MAGEA4/8 and PRAME double-positive tumor cell lines.
Anzu-cel Data Release
On June 1, 2026, the Company announced extended data from the ongoing Phase 1b clinical trial evaluating anzu-cel (anzutresgene autoleucel, IMA203) PRAME TCR T-cell therapy in heavily pretreated patients with advanced melanoma.
Patient Population. As of the September 24, 2025 data cutoff, 33 heavily pretreated patients with metastatic (stage IV) melanoma received a one-time infusion of anzu-cel at RP2D (1 – 10×109 TCR T cells). The treated patient population consisted of cutaneous melanoma (n=14), uveal melanoma (n=16), mucosal melanoma (n=2) and melanoma of unknown primary (n=1). All patients with cutaneous melanoma, mucosal melanoma and melanoma of unknown primary had metastatic stage IV disease including lesions in liver, brain and/or lung. All patients with uveal melanoma had metastatic stage IV disease with liver and/or extrahepatic metastases. Patients had a median of two prior lines of systemic treatment. The subgroup of patients with cutaneous melanoma (n=14) had a median of 2.5 lines of prior systemic treatments, thereof a median of two prior lines of immune checkpoint inhibitors. Of these, 64% (9/14) received a combination of ipilimumab and nivolumab and 29% (4/14) received a combination of nivolumab and relatlimab prior to anzu-cel infusion.
Safety Data. Anzu-cel has maintained a predictable and manageable tolerability profile, which was consistent across patients with different melanoma subtypes. The most frequent TEAEs were anticipated cytopenias associated with lymphodepletion. Expected and manageable CRS was observed, consistent with the mechanism of action (Grade 1 or 2: 82%, Grade ≥ 3: 18%). Some patients infrequently experienced ICANS (Grade 1 or 2: 6%, Grade ≥ 3: 6%) and HLH (Grade 1 or 2: 3%, Grade ≥ 3: 3%). The following table shows TEAEs occurring in 30% or more of patients:
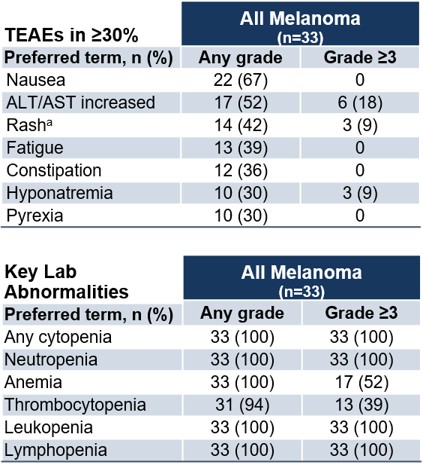
a Includes rash and rash maculopapular.
Anti-Tumor Activity.
| All melanoma1 (n=33) | Cutaneous melanoma (n=14) | Uveal melanoma1 (n=16) | |
| cORR | 56% (18/32) | 50% (7/14) | 67% (10/15) |
| ORR | 64% (21/33) | 57% (8/14) | 69% (11/16) |
| DCR | 91% (30/33) | 93% (13/14) | 88% (14/16) |
| mDOR (range) / mFU [mo] | 14.6 (4.2, 38.2+) / 18.7 | 17.9 (4.2, 38.2+) / 18.7 | 11.0 (4.4, 31.6) / Not defined |
| mPFS (range) / mFU [mo] | 6.1 (1.4, 39.6+) / 20.0 | 6.0 (1.4, 39.6+) / 20.0 | 8.5 (1.4, 32.9) / 10.4 |
| mOS (range) / mFU [mo] | 16.2 (2.4, 39.6+) / 17.3 | 13.9 (2.4, 39.6+) / 20.0 | Not reached (4.5, 34.2) / 14.3 |
1 cORR excludes one patient with uveal melanoma who left study (withdrew consent) with ongoing unconfirmed PR.
The PFS rate was 55% at six months and 37% at 12 months. The overall survival rate was 70% at 12 months and 46% at 24 months. 42% (14/33) of patients experienced a deep response (≥50% tumor reduction). In these patients, mPFS was 15.9 months at 39.6 months mFU.
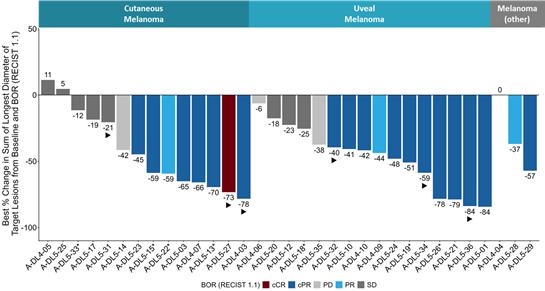
* Maximum change of target lesions and RECIST1.1 response at different timepoints. BL, baseline; BOR, best overall response; (c)CR, (confirmed) complete response; (c)PR, (confirmed) partial response; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease.
Anzu-cel induced systemic anti-tumor activity across multiple metastatic sites, including difficult-to-treat metastases, such as liver, lung, lymph node, abdomen/peritoneum, skin and others. Even patients who had a best overall response of Progressive Disease (PD) according to RECIST 1.1 (n=3) experienced shrinkage of individual lesions. Progressive disease was frequently the result of new lesions, progression of non-target lesions, or selective outgrowths of individual lesions, while many target lesions remained controlled, indicating continued control of baseline disease. Responses occurred rapidly (median time to BOR: 1.4 months) and were durable across multiple metastatic sites, including target and non-target lesions.
These findings support the continued development of anzu-cel in advanced melanoma. Immatics’ ongoing Phase 3 clinical trial, SUPRAME, is evaluating the efficacy, safety and tolerability of anzu-cel PRAME TCR T-cell therapy as a monotherapy vs. investigator's choice in patients with unresectable or metastatic cutaneous melanoma who have received prior treatment with a PD-1 immune checkpoint inhibitor.
In parallel, a Phase 2 cohort in metastatic uveal melanoma is ongoing and intended to support a potential label expansion for anzu-cel following expected initial approval in cutaneous melanoma.
* * *
Certain statements in this report may be considered forward-looking statements. Forward-looking statements generally relate to future events or the Company’s future financial or operating performance. For example, statements concerning timing of data read-outs for product candidates, observations from the Company’s clinical trials, the timing, outcome and design of clinical trials, the nature of clinical trials (including whether such clinical trials will be registration-enabling), the timing of IND, CTA or BLA filings, estimated market opportunities of product candidates, the Company’s focus on partnerships to advance its strategy, and other metrics are forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as “may”, “should”, “expect”, “plan”, “target”, “intend”, “will”, “estimate”, “anticipate”, “believe”, “predict”, “potential” or “continue”, or the negatives of these terms or variations of them or similar terminology. Such forward-looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ materially from those expressed or implied by such forward-looking statements. These forward-looking statements are based upon estimates and assumptions that, while considered reasonable by Immatics and its management, are inherently uncertain. New risks and uncertainties may emerge from time to time, and it is not
possible to predict all risks and uncertainties. Factors that may cause actual results to differ materially from current expectations include, but are not limited to, various factors beyond management's control including general economic conditions and other risks, uncertainties and factors set forth in the Company’s Annual Report on Form 20-F and other filings with the Securities and Exchange Commission (SEC). Nothing in this report should be regarded as a representation by any person that the forward-looking statements set forth herein will be achieved or that any of the contemplated results of such forward-looking statements will be achieved. You should not place undue reliance on forward-looking statements, which speak only as of the date they are made. The Company undertakes no duty to update these forward-looking statements. All the scientific and clinical data presented within this report are – by definition prior to completion of the clinical trial and a clinical study report – preliminary in nature and subject to further quality checks including customary source data verification.
* * *
In connection with the foregoing, the Company issued press releases, copies of which are attached hereto as Exhibit 99.1, Exhibit 99.2 and Exhibit 99.3, respectively, made available presentations, copies of which are attached hereto as Exhibit 99.4, Exhibit 99.5, Exhibit 99.6 and Exhibit 99.7, and made available an updated corporate presentation, a copy of which is attached hereto as Exhibit 99.8.
INCORPORATION BY REFERENCE
This Report on Form 6-K (other than the exhibits hereto) shall be deemed to be incorporated by reference into the registration statements on Form F-3 (Registration Nos. 333-240260, 333-274218 and 333-286151) of Immatics N.V. and to be a part thereof from the date on which this report is filed, to the extent not superseded by documents or reports subsequently filed or furnished.
EXHIBIT INDEX
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| IMMATICS N.V. | ||
| Date: June 1, 2026 | ||
| By: | /s/ Harpreet Singh | |
| Name: | Harpreet Singh | |
| Title: | Chief Executive Officer | |